

Abstract
BACKGROUND:
The objective of the present study was to evaluate the effect of the two methods of delivery, “hands-on” vs. “hands poised”, on perineal trauma and delivery outcome in primiparous women referred to Shariati Hospital of Isfahan during 2007-2008.
METHODS:
In a clinical trial study, 100 low risk primiparous pregnant women were randomly assigned to two hands-on and hand-poised (hands-off) groups. In the hands-on group, this method was used to control fetal head in the second stage of labor. It means that the fingers of one hand supported fetal occiput and the other hand applied slight pressure on the head to control the delivery of the head during the crowning process. In the hands-poised group, midwife observed the parturient woman and do not touch perineum during the second labor stage while fetal head was delivering. Then, the two groups were compared in terms of perineal trauma, as well as neonatal and delivery outcome.
RESULTS:
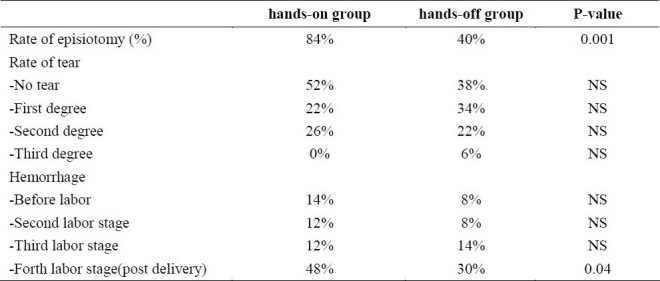
Demographic characteristics of all studied women were similar in two groups. The rate of episiotomy was higher in hands-on group (84% vs. 40%, p = 0.001). The rate of postpartum hemorrhage (4th stage) was higher in hands-on group (12% vs. 4%, p = 0.04). The rate of mild and moderate postpartum pain in hands-on group was higher than hands-off group (70% vs. 58% and 29% vs. 10%, p < 0.001) but sever pain was not different in two groups.
CONCLUSIONS:
It seems that hands-poised method is associated with less perineal trauma, particularly regarding the lower need for episiotomy and postpartum hemorrhage.
KEYWORDS: Hand-poised Method, Hands-on Method, Perineal Trauma, Delivery Outcome
There are different techniques to reduce the peripartum traumas. Some of these techniques are applied prepartum, but they are mostly used during delivery.1 One of the techniques that is employed to protect perineum during a vaginal delivery with cephalic presentation is as follows. Fingers of one hand support fetal occiput while the other hand applies a slight pressure on the head to control its delivery during crowning process.2
A systematic study showed that the techniques used to prevent perineal trauma during delivery are not ideal in this regard.3 Moreover, another study demonstrated that the role of episiotomy in preventing perineal trauma is unclear and the decision to perform episiotomy should be made based on the present circumstances. Thus, the procedure should not be carried out routinely owing to the higher risk of third and fourth degree perineal tear in episiotomy cases. Different studies showed that expectant management or hand-poised method is probably preferred in management of the active phase of the delivery to the active management or hands-on method.2
In hands-on method, when fetal head extended vulvae and perineum such that vaginal inlet was opened 5cm or more, the midwife can apply a forward pressure via perineum just in front of the coccyx on fetal chin with a gloved hand covered by a towel. Meanwhile, the other hand applies an upward pressure on occiput. This method, which is simpler to the method described by Ritgen, is commonly called Ritgen's maneuver or Ritgen's modified maneuver. This technique facilitates fetal head extension, and thus fetal head passes vaginal inlet on perineum with its smallest diameters.4 Ritgen's maneuver does not decrease the risk of anal sphincter injury at delivery, at least not when performed during a contraction.5
Some researchers have used hands-poised or hands-off method in which the role of midwife during delivery is as a guide and only applies slight pressure on fetal head, and child birth occurs without touching the perineum. In this method, the attendant does not touch the perineum during fetal head delivery. The rate of tears and neonatal outcome in hands-off method is similar to that of modified Ritgen's maneuver, but the rate of perineal trauma, particularly third degree tears is lower.6 Another studies showed that the hands-off or hand-poised perineum technique is prevalent in the management of labor. Ruben et al. hypothesized that a possible consequence might be an increased incidence of obstetric anal sphincter injury.7
The aim of this study was to evaluate the two methods, hands-on and hands-poised, routinely used in Iranian midwifery units for fetal head control during delivery, and comparing the two methods in terms of perineal traumas, need for episiotomy, severity of perineal tears, hemorrhage, perineal pain and hematoma, and delivery outcome including the duration of each labor stage, amount of hemorrhage in first, second, third and fourth stage of labor, and neonatal APGAR score and status.
Methods
This was a controlled randomized clinical trial study carried out to compare the effect of the two methods, hands-on and hands-poised, on perineal traumas and neonatal outcome. The study was carried out in labor ward of Shariati Hospital, in Isfahan. Primiparous women with term labor in the age range of 15-35 years, referred to this Hospital from 23 October 2008 to 23 October 2009 were enrolled.
Among the women referred to the ward and met the inclusion criteria of the study, 100 were randomly selected and randomly assigned to two groups, each included 50 participants. In one group, fetal head delivery was performed by hands-on and in the other group by hands-off method. From selected women, were assigned to two groups.
The study protocol was approved by the Ethics Committee of Islamic Azad University, Najaf Abad Branch. Written informed consent for participating in the study was obtained from all studied patients. Considering that hands-on method was performing routinely during delivery, another informed consent was obtained from those women who were selected for hands-off method.
The two groups were compared regarding their demographic characteristics, rate of episiotomy, rate of induction and different perineal trauma such as tear, peripartum hemorrhage, postpartum hemorrhage (it remains a major cause of maternal morbidity and mortality which is a clinical diagnosis defined by WHO as blood loss in excess of 500ml after delivery),8 postpartum pain (Macgill pain questionnaire with a 0-10 grade rating scale, 0 = no pain, 1-3 = mild pain, 4-6 = moderate pain, 7-9 = sever pain,10 = unbearable pain)9 and the delivery and neonatal outcomes including the duration of each stage of labor, induction status and neonates health (APGAR score).
Inclusion criteria were primiparity, term labor, cephalic presentation, and maternal age 15- 35 years. The women with preterm labor, special medical conditions, dystocia (prolonged or difficult labor), or those underwent analgesia during labor were excluded. The data was gathered using a questionnaire and analyzed by SPSS software.
Results
The demographic characteristics of participants in hands-on and hands-off groups are presented in Table 1. The distributions of different perineal trauma in two studied groups are presented in Table 2.
Table 1.
The demographic characteristics of studied population in hands-on and hands-off methods
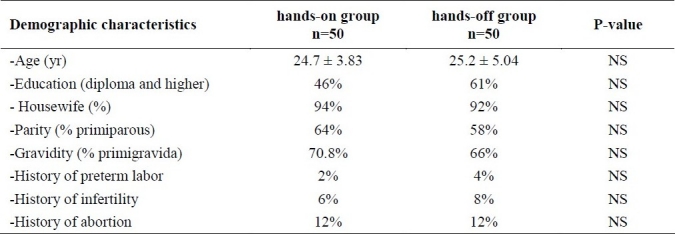
Table 2.
The distributions of different perineal trauma in hands-on and hands-off methods
Rate of induction was 82% in two groups and the frequency of using more than 10 units of syntocinon was 66% and 74% in hands-off and hands-on groups, respectively (p > 0.05). The rate of mild to moderate postpartum pain in hands-on group was higher than hands-off group (p < 0.001) but sever pain was not different in two groups. Regarding the delivery and neonatal outcomes including the duration of each stage of labor, induction status, and peripartum hemorrhage, the two studied groups were not significantly different. Differences in neonatal outcome, including one-minute and five-minute APGAR scores, weight, height, head circumference and chest circumference were not significant in two groups.
Discussion
In current study the characteristics of participants in two groups regarding age, educational level, occupation, years of marriage, history of infertility, and number of abortions were similar. It should be mentioned that most women referred to Shariati Hospital belonged to low to middle economic classes of the city. Therefore, most participants were housekeeper women within age range of 20-30 having high school diploma. These women become pregnant a short time after their marriage and there is a low rate of infertility or abortion history.
In a similar study, Costa et al. compared the hands-off and hands-on methods for decreasing perineal trauma during labor and indicated that the rate of laceration and neonatal outcomes were not different in two methods. They concluded that as the hands-off method did not change the frequency or degree of perineal lacerations in childbirth, it is not preferable to the hands-on method.10
Albers et al. reported a similar rate of labor-induced genital trauma in 1211 women in midwifery care who received one of the following procedures during the second stage of labor: Warm compresses to the perineal area, perineal massage with lubricant, and not touching the perineum until crowning of the fetal head.11
In another study on factors relates to the perineal trauma, Albers et al. evaluated 3049 pregnant women followed by midwives and midwifery students. During the delivery, the participants received hands-on perineum support and were positioned in lateral decubitus. It was concluded that mechanical maneuvers in perineum support or manual control of second labor stage, maternal position during labor, prolonged labor, oxytocin use and continuous fetal monitoring are directly related with increased perineum tears in primiparous women.12
Mayerhofer et al. compared the two methods of hands-on and hands-poised, and reported that 62.1% of participants with hands-on method had perineal trauma. A higher frequency of episiotomy was also observed in hands-on method. To explain these findings, they stated that perineal ischemia resulted from manual intervention is a major risk factor for sever perineal traumas.6 Obstetric anal sphincter injury (OASI) is a serious complication of vaginal delivery whose incidence has steadily increased in recent years worldwide.13 OASI carries a high risk of anal incontinence in the long term.14
According to the findings of this research, it seems that hands-off method is associated with less perineal trauma, particularly lower need for episiotomy. Episiotomy is a major risk factor for sever perineal traumas.15 Awareness about the relationship between episiotomy and women's health will help health care professionals develop policy and promote the application of restrictive episiotomy.16 Emily et al. reported Delivery options (episiotomy) that can markedly affect the rate of third/fourth degree perineal laceration (TFPL) for specific mothers.17
Costa et al. stated that the severity of perineal traumas in the two groups of hands-on and hands-poised were the same (82.7% versus 82.2% in first degree tears, and 17.3% versus 17.8% in second degree tears). Moreover, the position of the perineal tears in the two groups was the same. However, the hands-off group had a minor increase in anterior perineal tears (17.4% versus 62.1% in the hands-off group). In general, hands-off group had a higher frequency of anterior perineal tears (65.5% versus 16.7% in hands-on group). Anterior perineal tears were defined as the injuries to the clitoris, vestibule, periurethral region, labia major, labia minor and vaginal mucosa. They mentioned that the pressure applied to fetal head to support the anterior perineum in hands-on method shifts the head pressure on pubis arch. They reported a higher rate of posterior perineal tear in hands-on method.10
Findings of the current study demonstrated that there was a significant difference between the two groups in terms of episiotomy rate, such that 40% of hands-off group participants needed episiotomy. Though it was not higher significantly, but the rate of no tear was lower in hands-off method (38% vs. 52%). This can be explained by the higher frequency of episiotomy in hands-on group, which in turn led to lower frequency of tears. In addition, higher rate of first degree tears were observed in hands-off group (34% versus 22%), which can be due to lower frequency of episiotomy. The two groups were not significantly different considering second degree tears (26% and 22% for hands-on and hands-off groups, respectively). In general, low degree tears (minor lesions and traumas) were more frequent in hands-off group. Nonetheless, severe perineal trauma was absent or negligible in both groups. This finding is compatible with that of the study carried out by Albers et al. that examined the three methods of warm compress, lubricant perineal massage, and hands-off in the third step of the study.11
According to Albers et al.,11 mechanical maneuvers during labor is accompanied by perineal trauma. However, some studies like those carried out by Mayerhofer et al.6 and Costa et al.10 did not obtain such results. Moreover, the two groups of current study were not significantly different considering anterior perineal tears. Nevertheless, a higher rate of repaired anterior tears was observed in hands-on group, which can be due to perineal ischemia resulting from manual intervention. Costa et al. also reported a minor increase in anterior perineal tears in hands-on method.10
In the current study, The rate of hemorrhage was not significantly different in first, second and third stage of labor but it was higher in forth stage (postpartum) in hands-on group, which may be due to the high rate of episiotomy in mentioned group. The difference between the two groups regarding hemorrhage and hematoma at the episiotomy site was not significant. However, 82% of hands-on group participants did not have hemorrhage or hematoma at the site of episiotomy, while in the hands-off group the frequency was 74%. Thus, a mild increase in hemorrhage and hematoma was observed in the hands-off group which can be due to the tears caused by the absence of episiotomy, but the difference was not statistically significant. In general, the current study demonstrated that perineal tears were more frequent in the hands-on group.
This finding was similar to that obtained by Garcia.18 He evaluated the traditional hands-on method in which the midwife puts her hand-on perineum to control fetal head during the second labor stage against the non-interventional hand-poised method in terms of perineal trauma and neonatal outcome. The study was carried out on 1161 women out of 1501 women referred for labor to a University Hospital. His findings showed that 187 out of 574 women (32.5%) in the hands-on group had perineal trauma, while in hands-poised group 180 out of 502 women (34.58%) had perineal tears (p = 0.05). Sixty participant in the hands-on group (27%) and 5 in the hands-off group (0.9%) had third degree perineal tears (p < 0.05). In the hands-on group, 107 participants (17.6%) required episiotomy, while the frequency in the hand-poised group was 51 (10.1%) (p < 0.001). The finding was similar to what we obtained in the current study. Moreover, they did not observe any significant difference between the two groups regarding neonatal outcomes. They demonstrated that hands-poised method is more suitable in prevention of perineal trauma and can be employed as a safe and effective method in fetal head control during the second labor stage.18 Revicky et al. reported that rising incidence of Obstetric anal sphincter injury (OASI) after normal vaginal deliveries may be related to adoption of the hands-off technique or increased identification of tears.19
The study carried out by Costa et al.10 did not show a significant statistical difference between the two groups in the duration of fetal head delivery or the expulsion stage in the delivery with cephalic presentation. However, the time was longer for the hands-on group (21.3 versus 17.4 minutes). The duration of second labor stage was slightly shorter in hands-on group. In the current study, the duration of expulsion stage was not recorded. Considering the duration of the second labor stage, although the two groups were not significantly different in this regard, it was slightly longer in hands-off group (22 versus 23 minute). The duration of the first and third stages of labor was also recorded, but the two groups were not significantly different.
In another study, McCandlish et al.20 followed the two groups until ten days after delivery. It was shown that postpartum pain was less in hands-on group. Da costa, also, reported the pain 24 hours after delivery to be less in hands-on group. In the current study, the two groups were significantly different in this respect, such that mild to moderate pain was more frequent in hands-on group, while the two groups were not significantly different regarding severe pain.
Neonatal outcomes including 1- and 5-minute APGAR scores, height, weight, head circumference and oxygenation were not significantly different in the two groups, which is compatible with the findings of studies carried out by Da costa and McCandlish et al.20 in this regard. The rate of induction was similar in two groups and the frequency of using more than 10 unit syntocinon was not different between two groups.
In conclusion, regarding the findings of this research, it seems that hands-off method is associated with less perineal trauma, particularly lower need for episiotomy and less postpartum hemorrhage.
Authors’ Contributions
AF carried out the design and coordinated the study participated in all of the experiments and prepared the manuscript and data analysis and interpretation of the results. FF carried out the design of the study, AGH carried out the design and coordinated the study, VN and TH contributed to data collection.
Acknowledgments
We would like to thank the people who helped us through this research including all the staffs of the Labor Ward of Shariati Hospital, especially Ms. Bahreini and Mr. Basirat who sincerely and truthfully devoted his clinic to our sampling.
Footnotes
Conflict of Interests Authors have no conflict of interests.
References
- 1.Eason E, Labrecque M, Wells G, Feldman P. Preventing perineal trauma during childbirth: a systematic review. Obstet Gynecol. 2000;95(3):464–71. doi: 10.1016/s0029-7844(99)00560-8. [DOI] [PubMed] [Google Scholar]
- 2.Geranmayeh M, Rezaei Habibabadi Z, Fallahkish B, Farahani MA, Khakbazan Z, Mehran A. Reducing perineal trauma through perineal massage with vaseline in second stage of labor. Arch Gynecol Obstet. 2011 doi: 10.1007/s00404-011-1919-5. [DOI] [PubMed] [Google Scholar]
- 3.Meidan E, Walfisch A, Raz I, Levy A, Hallak M. Perineal massage during pregnancy: a prospective controlled trial. Isr Med Assoc J. 2008;10(7):499–502. [PubMed] [Google Scholar]
- 4.Downe S, Gerrett D, Renfrew MJ. A prospective randomised trial on the effect of position in the passive second stage of labour on birth outcome in nulliparous women using epidural analgesia. Midwifery. 2004;20(2):157–68. doi: 10.1016/S0266-6138(03)00052-4. [DOI] [PubMed] [Google Scholar]
- 5.Jnsson ER, Elfaghi I, Rydhstrm H, Herbst A. Modified Ritgen's maneuver for anal sphincter injury at delivery: a randomized controlled trial. Obstet Gynecol. 2008;112(2 Pt 1):212–7. doi: 10.1097/AOG.0b013e31817f2867. [DOI] [PubMed] [Google Scholar]
- 6.Mayerhofer K, Bodner-Adler B, Bodner K, Rabl M, Kaider A, Wagenbichler P, et al. Traditional care of the perineum during birth.A prospective, randomized, multicenter study of 1,076 women. J Reprod Med. 2002;47(6):477–82. [PubMed] [Google Scholar]
- 7.Trochez R, Waterfield M, Freeman RM. Hands on or hands off the perineum: a survey of care of the perineum in labour (HOOPS) Int Urogynecol J Pelvic Floor Dysfunct. 2011 doi: 10.1007/s00192-011-1454-8. [DOI] [PubMed] [Google Scholar]
- 8.Gogarten W. [Postpartum hemorrhage - an update] Anasthesiol Intensivmed Notfallmed Schmerzther. 2011;46(7-8):508–14. doi: 10.1055/s-0031-1284470. [DOI] [PubMed] [Google Scholar]
- 9.Fernandez E, Krusz JC, Hall S. Parsimonious collection of pain descriptors: classification and calibration by pain patients. J Pain. 2011;12(4):444–50. doi: 10.1016/j.jpain.2010.10.011. [DOI] [PubMed] [Google Scholar]
- 10.de Souza Caroci da Costa A, Gonzalez Riesco ML. A comparison of “hands off” versus “hands on” techniques for decreasing perineal lacerations during birth. J Midwifery Womens Health. 2006;51(2):106–11. doi: 10.1016/j.jmwh.2005.10.017. [DOI] [PubMed] [Google Scholar]
- 11.Albers LL, Sedler KD, Bedrick EJ, Teaf D, Peralta P. Midwifery care measures in the second stage of labor and reduction of genital tract trauma at birth: a randomized trial. J Midwifery Womens Health. 2005;50(5):365–72. doi: 10.1016/j.jmwh.2005.05.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Albers LL, Anderson D, Cragin L, Daniels SM, Hunter C, Sedler KD, et al. Factors related to perineal trauma in childbirth. J Nurse Midwifery. 1996;41(4):269–76. doi: 10.1016/0091-2182(96)00042-0. [DOI] [PubMed] [Google Scholar]
- 13.van Dillen J, Spaans M, van Keijsteren W, van Dillen M, Vredevoogd C, van Huizen M, et al. A prospective multicenter audit of labor-room episiotomy and anal sphincter injury assessment in the Netherlands. Int J Gynaecol Obstet. 2010;108(2):97–100. doi: 10.1016/j.ijgo.2009.08.021. [DOI] [PubMed] [Google Scholar]
- 14.Mous M, Muller SA, de Leeuw JW. Long-term effects of anal sphincter rupture during vaginal delivery: faecal incontinence and sexual complaints. BJOG. 2008;115(2):234–8. doi: 10.1111/j.1471-0528.2007.01502.x. [DOI] [PubMed] [Google Scholar]
- 15.Andrews V, Sultan AH, Thakar R, Jones PW. Risk factors for obstetric anal sphincter injury: a prospective study. Birth. 2006;33(2):117–22. doi: 10.1111/j.0730-7659.2006.00088.x. [DOI] [PubMed] [Google Scholar]
- 16.Chang SR, Chen KH, Lin HH, Chao YM, Lai YH. Comparison of the effects of episiotomy and no episiotomy on pain, urinary incontinence, and sexual function 3 months postpartum: a prospective follow-up study. Int J Nurs Stud. 2011;48(4):409–18. doi: 10.1016/j.ijnurstu.2010.07.017. [DOI] [PubMed] [Google Scholar]
- 17.Hamilton EF, Smith S, Yang L, Warrick P, Ciampi A. Third- and fourth-degree perineal lacerations: defining highrisk clinical clusters. Am J Obstet Gynecol. 2011;204(4):309. doi: 10.1016/j.ajog.2010.12.048. [DOI] [PubMed] [Google Scholar]
- 18.Garcia J. Policy of “hands poised” care by attendant in normal birth is not recommended. BMJ. 1999;319(7205):322. doi: 10.1136/bmj.319.7205.322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Revicky V, Nirmal D, Mukhopadhyay S, Morris EP, Nieto JJ. Could a mediolateral episiotomy prevent obstetric anal sphincter injury? Eur J Obstet Gynecol Reprod Biol. 2010;150(2):142–6. doi: 10.1016/j.ejogrb.2010.03.002. [DOI] [PubMed] [Google Scholar]
- 20.McCandlish R, Bowler U, van Asten H, Berridge G, Winter C, Sames L, et al. A randomised controlled trial of care of the perineum during second stage of normal labour. Br J Obstet Gynaecol. 1998;105(12):1262–72. doi: 10.1111/j.1471-0528.1998.tb10004.x. [DOI] [PubMed] [Google Scholar]
- 21.de Souza Caroci da Costa A, Gonzalez Riesco ML. A comparison of “hands off” versus “hands on” techniques for decreasing perineal lacerations during birth. J Midwifery Womens Health. 2006;51(2):106–11. doi: 10.1016/j.jmwh.2005.10.017. [DOI] [PubMed] [Google Scholar]