

Abstract
BACKGROUND:
Applying an effective management system in emergency incidents provides maximum efficiency with using minimum facilities and human resources. Hospital Emergency Incident Command System (HEICS) is one of the most reliable emergency incident command systems to make hospitals more efficient and to increase patient safety. This research was to study requirements, barriers, and strategies of HEICS in hospitals affiliated to Isfahan University of Medical Sciences (IUMS).
METHODS:
This was a qualitative research carried out in Isfahan Province, Iran during 2008-09. The study population included senior hospital managers of IUMS and key informants in emergency incident management across Isfahan Province. Sampling method was in non-random purposeful form and snowball technique was used. The research instrument for data collection was semi-structured interview; collected data was analyzed by Colaizzi Technique.
RESULTS:
Findings of study were categorized into three general categories including requirements (organizational and sub-organizational), barriers (internal and external) of HEICS establishment, and providing short, mid and long term strategies. These categories are explained in details in the main text.
CONCLUSIONS:
Regarding the existing barriers in establishment of HEICS, it is recommended that responsible authorities in different levels of health care system prepare necessary conditions for implementing such system as soon as possible via encouraging and supporting systems. This paper may help health policy makers to get reasonable framework and have comprehensive view for establishing HEICS in hospitals. It is necessary to consider requirements and viewpoints of stakeholders before any health policy making or planning.
KEYWORDS: Hospital Emergency Incident Command System (HEICS), Hospital Management, Disaster Planning, Contingency Planning, IUMS, Iran
Critical incidents are sudden, unanticipated events or situations that require quick decisions and responses.1 Some researches pointed out that today crisis management and disaster planning in necessary for Iranian organizations.2 It is obvious that among various components of management, crisis management, relief and rescue in emergency incidents plays the most important role in health care systems (especially hospitals as the main unit for providing services), and thus there is a need for a plan to deal with incidents.3
Experience in all around the world and especially in our country shows that confusion and chaos are the most common issues which are confronted in hospitals when there is a crisis. It is clear that if an effective management system with accurate organization and preplanned activities strikes out quickly, negative consequences of such incidents might be minimized and maximum efficiency of medical services by utilizing minimum facilities and human recourses can be achieved.2,4,5
Incident command system (ICS) is currently the most common system of incident management in the world which its acceptability is increasingly growing regarding its successful outcomes.2,5 In ICS, one person is appointed as incident commander, who is responsible for directing emergency team or taskforce group. ICS is founded on some basic principles, which on one hand, ensure using resources effectively, and on the other hand, reduce disorders in policy making and operations of responsible groups or organizations.6
Successful response of hospitals to the crisis requires coordination among all hospital units, planning and coordination of police, fire-fighting and pre-hospital emergency forces in order to make sure communication lines are established and there is needed flexibility for responding to extent and severity of incident.7
For preparing and increasing efficiency in hospitals in such circumstances, various protocols have been proposed around the world which HEICS is one of the most reliable ones.2 In fact, HEICS is an incident management system composed of some specific roles in the form of an organizational table. Each of these roles has a specific mission during crisis situation, and there is a list of individual job description which guide appointed person in the crisis situation carefully. Actually HEICS allows providing as much responsibilities as required at any time, and it means more effectiveness and lower cost. Thus, HEICS has capability of adapting with different kinds of incidents and crisis in any scale.8
HEICS help to provide more coordination between hospitals and other institutions involved in emergency incidents by utilizing logical management structure, duty descriptions, creating clear reporting channels as well as developing a common and simple nomenclature system.2,5,9
HEICS provides a commanding system which doesn’t rely on specific people, but it is flexible.7 Significant and effective features in HEICS, especially in its third version have made it one of the most common and most comprehensive hospital management systems. Familiarity with this system and using it seems necessary regarding our country's condition.10
According to research done in this area, hospitals of Isfahan University of Medical Sciences have failed to establish HEICS completely and successfully. Regarding the fact that the lack of full deployment of this system would have irreparable consequences for the society and there is no similar research on barriers and requirements of the establishment of this system,11 this study has been done with the aim of studying requirements, barriers and strategies for establishment of HEICS in hospitals of Isfahan University of Medical Sciences.
Methods
This study was a qualitative research carried out in Isfahan Province, Iran during 2008-09. The study population included senior hospital managers, senior managers with management experience and key informants in emergency incident management across Isfahan Province, Iran. Sampling method was non-random purposeful method, and snowball technique was used. First, five key informant persons were selected and then, other members were selected by consulting with them in snowball technique. Participants included general physicians and specialists experienced in the field of disaster as well as those having experience in hospital or health center management in national and regional levels. At the end, after gathering and analyzing content of eleven interviews, the research process saturated in findings. Data collection tool was semistructured interview. Several questions were prepared about HEICS establishment, and the number of questions was increased depending on interview conditions.
The method used for interview data analysis was content analysis in Colaizzi method.12
All three researchers analyzed the content of interviews collaboratively. First, all contents of interviews including explanations and comments of those interviewed were fully studied and key components, concepts and statements of participants were determined as study codes. Then, key statements of each interview were extracted and summarized. In the next step, basic parts of materials of samples were combined and final conclusions were gained. In qualitative studies, unlike some quantitative methods, it is not possible to use accurate tools for measuring reliability and validity of research findings. However, due to being two-stage interviews, after interviews were completed, all interviewees’ talks were inscribed on paper and findings were provided to the participants for getting their feedback about validity of content and verifying the results.
Results
Findings of study were classified in three general categories including requirements of HEICS establishment, barriers of HEICS establishment and providing respective strategies. Barriers for HEICS establishment are classified into two categories: internal and external. Internal barriers are related to organizational requirements. Some of the internal barriers have organizational requirements and some of them don’t. Also, External barriers are related to the infrastructure requirements (Figures 1 and 2).
Figure 1.
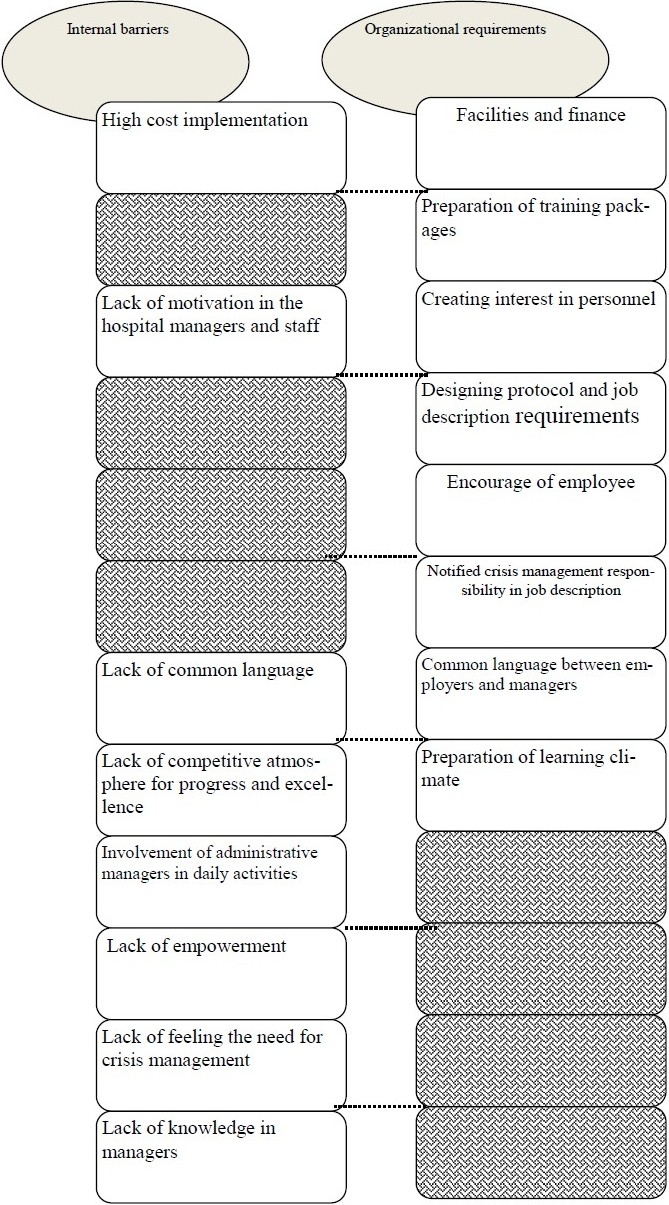
Internal barriers and organizational requirements
Figure 2.
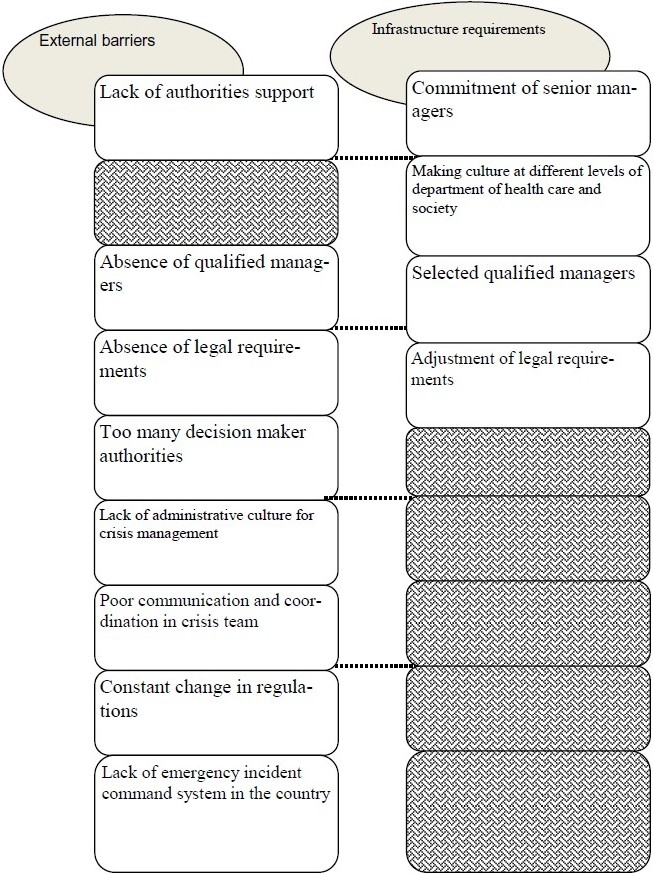
External barriers and infrastructure requirements
About organizational requirements for establishment of HEICS, for example Code 02 said “requirements include management, resources and organizational culture that each have special subset.” In addition, about infrastructure requirements, Code 07 said “the first and the last requirement is belief and commitment of senior managers, at least in provincial level.”
Findings of this research showed that internal and external barriers have prevented the establishment of such a system. In this regard, for example about internal barriers code 11 said “managers are not trained about application of this system; so we should design training system and justify them about its importance.”
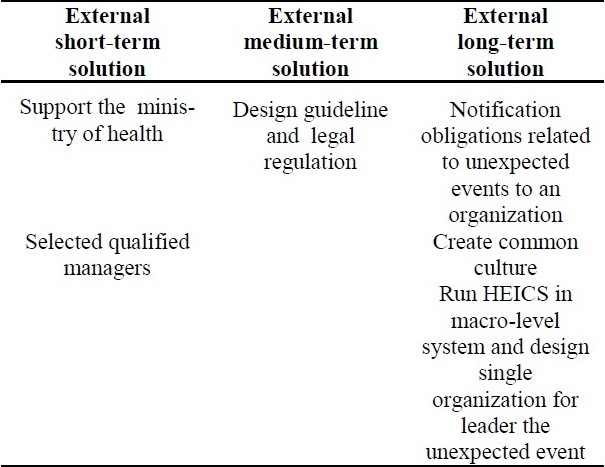
According to these barriers, interviewees suggested some solutions. These solutions are classified in two categories: internal solutions and external solutions. In each category, we have three periods of time for implementing the strategies. Each strategy belongs to a special period including short-term, medium-term and long-term (Tables 1 and 2). For example, code 03 said “we should allocate dedicated funding for establishment of this system and training the managers.”
Table 1.
Internal solutions for establishment of HEICS
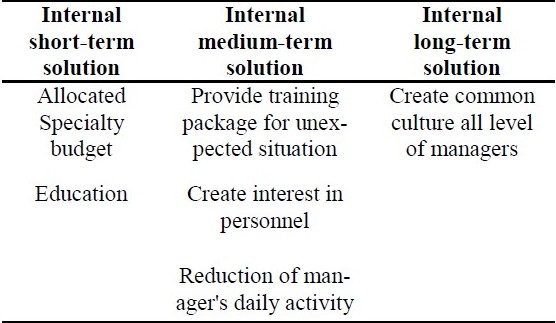
Table 2.
External solutions for establishment of HEICS
Discussion
According to interviewees’ transcripts, none of hospitals of Isfahan University of Medical Sciences established such system completely and activities done in this direction had been incomplete. Findings of this study indicated that barriers of establishment of this system in hospitals include lack of administrative culture for crisis management, lack of need for establishment of such system on behalf of managers, absence of statutory requirements and instructions related to crisis management, too many decision maker authorities, high cost implementation, lack of authorities support and non-commitment of managers, lack of qualified managers in different levels, poor communication and coordination in crisis team, lack of competitive atmosphere for progress and excellence and planning among hospitals, attention to daily activities by managers, absence of a common management language, constant change in regulations, absence of ICS in the country and lack of unity of command in hospitals. Research results are summarized in a conceptual framework.
Akhavan-moghaddam argues that lack of understanding of system's goals and the spirit governing it, non-conformity of existing organization with target organization and high cost of change in organization are among the main barriers of this system; and, justifying senior managers of hospitals about requirements, benefits and features of this system, formation of hospital crisis committee for implementing this system, training managers and staff are some strategies for implementing this system which are consistent with findings of this study.2 Findings of this study were consistent with those of Yarmohammadian related to non-commitment of managers about unexpected incidents, insufficient education of personnel and lack of planning and non-formation of emergency incident committee as barriers of establishment of this system.10,11 Similarly, findings of Ebrahimipur's work are consistent with key findings of this study including non-formation of unexpected incidents committee, lack of theoretical and practical training courses for staff and managers and lack of planning for unexpected incidents.13 Results of Ghayeman's work indicated that there is no clear process for reflecting incidents and it is done based on hospital managers and their personalized action, which is in consistency with findings of this study including lack of written guidelines in the field of crisis management and absence of ICS system in most hospitals.14 Research results of Anbari showed that there was no plan for emergencies and required training for staff related to tasks in emergencies and staffs were not organized appropriately. This is consistent with the results of this study related to lack of written guidelines in the field of crisis management, lack of planned educational program and unexpected incidents committee.15 According to the research carried out by Kavari for studying preparation level of educational hospitals affiliated to Shiraz University of Medical Sciences on crisis management, there were no rescue and relief programs in any of these centers, which is in consistency with the findings of this study related to lack of educational programs for staffs.16 In Sadegh-Goli's work done by Red Crescent organization, poor management and lack of careful planning, existing parallel organizations and absence of intersection coordination are introduced as the main problems in providing relief and health care services of this organization, which are matched with key findings of this study including lack of knowledgeable managers familiar with HEICS and scientific management, not feeling the need for planning and lack of writing and clear task descriptions for different responsible organization.17 Results of Kianpur's work entitled as “review of emergency management in the health sector in Iran” implied that regulations, policies, strategies and national plan of health sector for emergency management are not codified and documented. As well, offices affiliated to health ministry act independently in dealing with incidents. This is consistent with key findings of this study, that is, lack of codified regulations and strategies in the field of emergency management and non inter-section coordination between subsets of health deputy.18 Onil argued that familiarity with organizational structure of HEICS and ICS and correct understanding of them are among requirements for successful response to disasters and incidents, and suggested staff training is necessary in this way. Findings of this study approved it too.19 Richard Zan stated that planning and appropriate training of major actors, especially nursing supervisors and physicians of emergency department is very effective in deploying HEICS, and findings of his work are consistent with requirements stated in this study regarding training managers and staffs. He suggested that the following 4 factors are requirements of establishment of this system: adherence to rules, correct knowledge and understanding of this system, interaction with other organizations and interpart coordination.7
Conclusion
Since this system is one of the necessary needs of hospitals, it is recommended that such barriers should be eliminated and responsible entities including health ministry, hospitals of universities of medical sciences and affiliated hospitals provide codified and ordered plans for establishment of this system. In addition, financial barriers should be eliminated and hospital managers should be financed for establishment of HEICS, learning environment should be provided and the necessary rules and regulations must be formulated. Also, governance and health commission of parliament should do policy making to provide infrastructures in national level. Thus, among necessary measures in this direction are training managers and staffs and creating commitment in them for establishment of this system, codifying complete instruction of HEICS and informing it to hospitals for implementation, boosting unexpected incident committee and directing it in line with goals and tasks of HEICS, which can be done in universities of medical sciences.
Authors’ Contributions
MHY provided main idea and design of study and also coordinated the study as well as participated in analyzing data. GA and LSH did interviews and collected the data and participated in data analysis. AH participated in design and analyzing the contents. All authors read and approved the content of the manuscript.
Acknowledgments
This article is extracted from the research project number 287025 approved by Health Management and Economic Research Center (HMERC), Isfahan University of Medical Sciences. The authors would like to acknowledge and appreciate the kind assistance and financial support provided by HMERC. They also convey their thanks to all of Experts and managers who participated to the research.
Footnotes
Conflict of Interests Authors have no conflict of interests.
References
- 1.Trans. Group Translators of School of Medical Sciences. Isfahan: Isfahan University of Medical Sciences Publication; 2006. Disaster Management Center, University Vynkansyn America. Disaster Management. [Google Scholar]
- 2.Akhavan Moghaddam J, Adib Nazhad S, Mousavi Naeini S. Study of Hospital Emergency Incident Comamand System and How Execute. Journal of Military Medicine. 2005;7(2):167–75. [Google Scholar]
- 3.Sztajnkrycer MD. Hospital preparedness: A public health mandate remainsunder-appreciated. Internet Journal of Rescue and Disaster Medicine. 2004;4(2):16–20. [Google Scholar]
- 4.Abolghasemi H, Fortutan Q, Radfr MH, AMID A. Review Operations of Sepah Pasdaran Islamic Revolution in bam. Journal of Military Medicine. 2003;5(4):253–8. [Google Scholar]
- 5.Iraqi Zadeh H, Saghafi Nia M, Entezari V. Review the treatment of disaster management: Review of the Bam earthquake experience. Journal of Military Medicine. 2003;5(4):259–68. [Google Scholar]
- 6.Ebrahimi M, Jenab Hosseini V. Proceedings of the 1st International Congress on Health and crisis management disaster; 2003. Tehran, Iran: 2003. Mar 6-8, Incident command system (ICS) [Google Scholar]
- 7.Zane RD, Prestipino AL. Implementing the Hospital Emergency Incident Command System: an integrated delivery system's experience. Prehosp Disaster Med. 2004;19(4):311–7. doi: 10.1017/s1049023x00001941. [DOI] [PubMed] [Google Scholar]
- 8.Pletz B, Cheu D, Russell P. 3rd ed. California: San Mateo County Health Services Agency, Emergency Medical Services; 1998. HEICS: the hospital emergency incident command system. [Google Scholar]
- 9.Jagminas L, Bubly G. The Hospital Emergency Incident Command System--are you ready? Med Health R I. 2003;86(7):193–5. [PubMed] [Google Scholar]
- 10.Yarmohamadian MH, Shams L, Atighechian G, Haghshenas A. Proceedings of the International Disaster and Risk Conference IDRC; 2010. Davos, Switzerland: 2010. May, June. Assessing infrastructures and needs for establishing Hospital Emergency Incidence Command System (HEICS) in teaching hospitals, Isfahan, Iran. [Google Scholar]
- 11.Yarmohammadian MH, Shadkam N. Isfahan: Isfahan University of Medical Sciences; 2006. Evaluation hospitals affiliated to Isfahan University of Medical Sciences in the field of disaster, [Project] [Google Scholar]
- 12.Boeije H. London: SAGE Publications Ltd; 2009. Analysis in Qualitative Research. [Google Scholar]
- 13.Ebrahimi Pour H, Dehnaviyeh R. Proceedings of the 2nd International Congress on Health and crisis management disaster; 2004. Tehran, Iran: 2011. Dec 3-5, Readiness review public hospitals Iran University of Medical Sciences to deal with disasters. 2011. [Google Scholar]
- 14.Qyman Z, Moghimi E. Proceedings of the 2nd International Congress on Health and crisis management disaster; 2004. Tehran, Iran: 2004. Dec 3-5, Events occurred during the past 25 years in hospitals affiliated to Tehran University of Medical Sciences. [Google Scholar]
- 15.Anbari Z. Proceedings of the 1st International Congress on Health and crisis management disaster; 2003. Tehran, Iran: 2003. Mar 6-8, Readiness review medical centers affiliated to University of Medical Sciences of the crisis point of disaster. [Google Scholar]
- 16.Kvary H, Panahi A. Proceedings of the 2nd International Congress on Health and crisis management disaster; 2004. Tehran, Iran: 2004. Dec 3-5, Readiness review teaching hospitals affiliated to Shiraz University of Medical Sciences of crisis management in 2003. [Google Scholar]
- 17.Sadegh Goli M, Sajjadi H. Proceedings of the 2nd International Congress on Health and crisis management disaster; 2004. Tehran, Iran: 2004. Dec 3-5, Population of Red Crescent and earthquake in Bam. [Google Scholar]
- 18.Kianpour Atabaki V, Sadeghi Pour HR. Proceedings of the 1st International Congress on Health and crisis management disaster; 2003. Tehran, Iran: 2003. Mar 6-8, Emergency management in the health sector. [Google Scholar]
- 19.O’Neill PA. The ABC's of disaster response. Scand J Surg. 2005;94(4):259–66. doi: 10.1177/145749690509400403. [DOI] [PubMed] [Google Scholar]