

Abstract
BACKGROUND:
The present study sought to 1) investigate the degrees of correlations between different disease activity scores (DASs) and health-related quality of life (HRQoL), and 2) determine if DASs correlate with either physical or mental HRQoL.
METHODS:
Eighty patients with rheumatoid arthritis (RA) were assessed for different DASs, measured with erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP), namely DAS4-ESR, DAS-3 ESR, DAS4-CRP, DAS3-CRP, DAS4-28 ESR, DAS3-28 ESR, DAS4-28 CRP, and DAS3-28 CRP, and Simplified Disease Activity Indexes namely SDAI-ESR, and SDAI-CRP. Physical and mental HRQoL were measured using the SF-36. The Pearson correlation test was employed to examine the correlations between HRQoL and different DAS indices. PASS 2000 (Power Analysis and Sample Size) software was utilized to find significant differences between the correlations.
RESULTS:
SF-36 total score showed a significant inverse correlation with the DAS4-ESR, DAS-3 ESR, DAS4-CRP, DAS3-CRP, DAS4-28 ESR, DAS3-28 ESR, DAS4-28 CRP, and DAS3-28 CRP, with correlation coefficients of -0.320, -0.314, -0.330, -0.323, -0.327, -0.318, -0.360 and -0.348, respectively (P < 0.01 for all). The correlation coefficients between different DAS indices and the HRQoL score were not significantly different. In addition, all DASs showed significant correlations with physical HRQoL, but not with mental HRQoL.
CONCLUSIONS:
Among patients with RA, disease severity indices are associated with physical, but not mental HRQoL. However this study failed to show any differences between various DASs in their clinical use.
KEYWORDS: Health-Related Quality of Life, Rheumatoid Arthritis, Disease Activity Score
Disease activity score (DAS) is defined as a cascade of immunological and inflammatory reactions which cannot be measured by one single variable. In clinical practice, an opinion on the disease activity is formed on the basis of information about findings on clinical variables in a combination of different laboratory measures.1 Various DAS indices have been extensively developed for rheumatoid arthritis (RA). These indices are being used both in clinical trials and routine rheumatology practice.2–7
Several formulas are available for the calculation of DAS, which may cause some confusion.8 In addition, various DAS indices have shown different correlations with clinical and laboratory variables.9,10 These variables are known to be the common features of RA which affect all the aspects of the health-related quality of life (HRQoL).11 Therefore, their improvement is increasingly recognized as a major treatment goal.12 Thus, a clear understanding of the relationship between various conventional DAS indices and HRQoL outcomes in RA patients is highly important.11,12
Our knowledge regarding the possible link between DAS and HRQoL is limited. The primary objective of this study was to investigate the degrees of association between various DAS indices and HRQoL among patients with RA. As a secondary aim, we also assessed the associations between different DAS indices. To our knowledge, this is the first report on the comparison between the correlation coefficients (r) of the various DAS scores and HRQoL.
Methods
As a part of ten conditions ten morbidity measure study,13 this cross-sectional study invited 100 consecutive patients (both male and female at a minimum age of 18 years) diagnosed with RA, confirmed by a rheumatologist based on the American Rheumatism Association criteria.14 The patients were recruited between June and December 2006 to the outpatient rheumatology clinic of Baqiyatallah Hospital, Tehran, Iran. Exclusion criteria were association with a necrotic vascular disease or a handicap prior to RA.15 Eighty patients met the inclusion criteria. The study was approved by the Ethics Committee on Human Research of Baqiyatallah University of Medical Sciences. Written informed consents were obtained from all participants.
Data collection
A checklist containing questions on demographic data (age, gender, marital status, living place, monthly family income, and education level) was completed by every patient and was collected by a research nurse upon enrollment.
The patients’ global assessment of disease activity (PatGA) and pain (Pain-VAS) over the previous month were recorded using a visual analogue scale (VAS). A 100-mm rating scale was applied, with one end bearing the statement “no problem whatsoever” and the other end “unbearable”. The patients were instructed to place a vertical mark on the scale reflecting their own health status. The distance from the “no problem whatsoever” end was measured in millimeters. All the patients underwent a medical examination by a board-certified rheumatologist, who also determined the duration of their disease and performed a standard 28-joint assessment for tender and swollen joints making use of pain score and swelling score described in the EULAR manual of clinical methods.16 A similar VAS was utilized to determine the physician's global assessment of the disease activity (PhyGA).
DASs
Laboratory investigations comprised of determining erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) by Westergren method and Nephelometry, respectively.17 DAS indices, namely DAS-ESR-3, DAS-ESR-4, DAS-CRP-3, DAS-CRP-4, DAS28-ESR-3, DAS28-ESR-4, DAS28-CRP-3, DAS28-CRP-4, and Simplified Disease Activity Index [SDAI (ESR), SDAI (CRP)], were calculated using the formula described in previous reports.17,18
The patients’ HRQoL was measured via the Medical Outcomes Study 36-Item Short Form Health Survey (SF-36).19 SF-36 is a generic multidimensional measure of HRQoL that contains eight subscales representing physical functioning, social functioning, role limitations due to physical health problems, role limitations attributable to emotional problems, mental health, vitality, bodily pain, and general health perceptions. Higher scores of each subscale (which can range from 0 to 100) indicate a better HRQoL. The physical and mental components of the eight scales are combined into physical (PCS) and mental (MCS) component summary scale scores. SF-36 has been proved reliable and valid in RA patients.20 A Persian version of SF-36 was used to ensure face validity and maximize the acceptability in our participants, all of whom were Persian speakers.21,22 SF36 has been used for RA studies in Iran.23
Statistical analysis
SPSS statistical software was employed in statistical analyses. The Pearson correlation was utilized to examine 1) the correlations between the SF-36 scores and the DAS indices and 2) the correlations between different DAS indices. The correlation coefficients of the SF-36 scores and the DAS indices were compared using PASS 2000 (Power Analysis and Sample Size) software. P-values below 0.05 were considered significant.
Results
Patients
The patients were predominantly female (70, 87.5%). Mean (SD) age of the participants was 43.2 (11.7) years. Median (first and second quartiles) disease duration was 60 (24-99) months. Table 2 depicts demographic and clinical characteristics of the patients.
Table 2.
Demographic and clinical characteristics of the studied population (n =80)
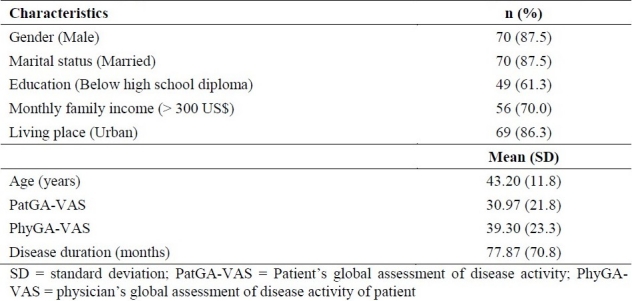
Table 1.
Different disease activity score (DAS) indices and formulas

DAS scores
Mean serum levels of ESR and CRP were 2 6.0 ± 19.6 mm/h and 1.14 ± 0.34 mg/l, respectively. The mean (SD) DAS4 score was 1.7 ± 0.8 (range, 0.2 to 4.2), and the mean values of the DAS-ESR-3, DAS- CRP -4, and DAS-CRP-3 CRP scores were 1.9 ± 0.8 (range, 0.4 to 4.4), 1.5 ± 0.7 (range, 0.5 to 4.3), and 1.6 ± 0.7 (range, 0.7 to 4.5), respectively. In addition, the mean (SD) DAS28-ESR-4 score was 3.0 ± 1.0 (range, 0.5 to 5.6), and the mean values of the DAS28-ESR-3, DAS28-CRP-4, and DAS28-CRP-3 scores were 3.3 ± 1.1 (range, 0.6 to 6.0), 2.4 ± 0.9 (range, 1.2 to 5.3), and 2.7 ± 0.9 (range, 1.4 to 5.8), respectively. Also, the respective mean (SD) SDAI and SDAI (CRP) scores were 36.5 ± 23.3 (range, 5.7 to 106.3) and 12.0 ± 7.4 (range, 1.8 to 39.2).
Table 3 dpresents the correlations between different DASs.
Table 3.
Correlations among different disease activity indices

HRQoL
The mean (SD) SF-36 total score among all patients was 49.8 ± 16.7 (range, 18.1 to 91.5). The correlation coefficients between HRQoL and different DAS indices are depicted in Table 3. As it is seen in Table 4, the DASs correlated with physical HRQoL but they did not relate with mental HRQoL.
Table 4.
Correlations between different disease activity indices and health-related quality of life in rheumatoid arthritis

The use of PASS 2000 software showed no significant difference in terms of correlation coefficients between different DAS indices and HRQoL scores.
Discussion
Our study failed to show any significant difference between correlation coefficients (r) regarding the association between various DAS scores and HRQoL. On the other hand, although no association was found between DAS indices and mental HRQoL, they were found to be linked with physical HRQoL.
To our knowledge, this is the first report on the comparison between the correlation coefficients (r) of various DAS scores and HRQoL. One study in Lithuania showed that patients with higher disease activity scores, as expressed by DAS-ESR-28, had worse physical function, more frequent comorbidities, and worse general health measured by SF-36.24 Patients of certain races may report a more pronounced impact of DAS on their daily life.25 Also, groups of RA patients with similar disease activity may report different health status across several dimensions of health. These show that the correlation between DAS and HRQoL may be more complicated than it is thought.
In our study, RA disease activity scores showed only a moderate correlation with HRQoL. This may be due to the fact that variance of general HRQoL questionnaires are attributable to non disease-related aspects, which are not measured by DAS indices.26
In this study, DASs had a correlation with physical HRQoL but not with mental HRQoL. Previous studies have demonstrated that disease related variables are strong determinants of physical disability, but not necessarily the mental health.27–30 Nevertheless, in some studies, disease activity has been shown to be correlated with both physical and psychological domains of HRQoL. It is worth mentioning that in all of these studies, disease activity has a stronger correlation with physical health than with mental health.31–33
To explain the mechanism of the correlation between DASs and physical health, one should note that disease activity is closely related to the extent of joint destruction and that surrogates of inflammation include the degree of clinical disease activity, the major expressions of which are pain, stiffness, and swelling of the joints. Furthermore, the variables of disease activity are rapid loss of working capacity, premature mortality, and a reduction of quality of life.27–30
Another finding of the present study was the almost perfect correlation between DAS28-ESR-4 and DAS28-CRP-4 (r = 0.861). One study had previously reported this correlation coefficient to be 0.946. The strong correlation between DAS28-ESR and DAS28-CRP means that these can be used interchangeably in clinical settings.34 In contrast, some researchers believe that in comparison to DAS28-ESR, DAS28-CRP may underestimate the disease activity and overestimate the improvement in disease activity.35
This was a secondary analysis with its own limitations.36,37 The HRQoL of RA patients is influenced by several variables which were not measured in our study.11,12 This was a single center study with limited sample size, and because of the cross-sectional design, illustrating a causal relationship was beyond the scope of this study. Associations of different DASs with other morbidity measures such as disability, physical condition, and pain need further research.
Our results have some clinical implementations. Based on our results, there is no superiority for one of the DASs in comparison to others, to reflect the morbidity in RA. We believe that further prospective studies should be conducted to assess whether an improvement in the various DAS variables has a stronger correlation with the degrees of improvement in the HRQoL of RA patients. One important point that should be borne in mind in the interpretation of our results is the fact that our patients were experiencing mild to moderate DAS and none of them was experiencing severe, incapacitating disease. The low disease severity of RA patients has, however, been reported elsewhere.38,39
To conclude, in our RA patients the correlations between various DAS indices and HRQoL were similar, and the DAS indices had correlations with physical HRQoL but not with mental HRQoL.
Authors’ Contributions
All the authors have carried out the study, participated in the design of the study and acquisition of data performed the statistical analysis and wrote the manuscript. All authors read and approved the final manuscript.
Acknowledgments
This study was fully supported and funded by Baqiyatallah University of Medical Sciences.
Footnotes
Conflict of Interests Authors have no conflict of interests.
References
- 1.Arvidson NG. Disease activity in rheumatoid arthritis: studies on interleukin-6, tumour necrosis factor alpha, monocyte activity, acute phase markers, glucocorticoids, and disability. Uppsala: Acta Universitatis Upsaliensis; 2003. pp. 1248–88. [Google Scholar]
- 2.Rintelen B, Sautner J, Haindl PM, Andel I, Maktari A, Leeb BF. Comparison of three rheumatoid arthritis disease activity scores in clinical routine. Scand J Rheumatol. 2009;38(5):336–41. doi: 10.1080/03009740902932835. [DOI] [PubMed] [Google Scholar]
- 3.Salaffi F, Cimmino MA, Leardini G, Gasparini S, Grassi W. Disease activity assessment of rheumatoid arthritis in daily practice: validity, internal consistency, reliability and congruency of the Disease Activity Score including 28 joints (DAS28) compared with the Clinical Disease Activity Index (CDAI) Clin Exp Rheumatol. 2009;27(4):552–9. [PubMed] [Google Scholar]
- 4.Castrejon I, Ortiz AM, Toledano E, Castaneda S, Garcia-Vadillo A, Patino E, et al. Estimated cutoff points for the 28-joint disease activity score based on C-reactive protein in a longitudinal register of early arthritis. J Rheumatol. 2010;37(7):1439–43. doi: 10.3899/jrheum.091333. [DOI] [PubMed] [Google Scholar]
- 5.Pincus T, Yazici Y, Bergman MJ. RAPID3, an index to assess and monitor patients with rheumatoid arthritis, without formal joint counts: similar results to DAS28 and CDAI in clinical trials and clinical care. Rheum Dis Clin North Am. 2009;35(4):773–8. doi: 10.1016/j.rdc.2009.10.008. viii. [DOI] [PubMed] [Google Scholar]
- 6.Fransen J, van Riel PL. The Disease Activity Score and the EULAR response criteria. Clin Exp Rheumatol. 2005;23(5 Suppl 39):S93–S99. [PubMed] [Google Scholar]
- 7.Pincus T. Can RAPID3, an index without formal joint counts or laboratory tests, serve to guide rheumatologists in tight control of rheumatoid arthritis in usual clinical care? Bull NYU Hosp Jt Dis. 2009;67(3):254–66. [PubMed] [Google Scholar]
- 8.Van der Heijde DM, Jacobs JW. The original “DAS” and the “DAS28” are not interchangeable: comment on the articles by Prevoo et al. Arthritis Rheum. 1998;41(5):942–5. doi: 10.1002/1529-0131(199805)41:5<942::AID-ART26>3.0.CO;2-B. [DOI] [PubMed] [Google Scholar]
- 9.Van Leeuwen MA, Van der Heijde DM, van Rijswijk MH, Houtman PM, van Riel PL, van de Putte LB, et al. Interrelationship of outcome measures and process variables in early rheumatoid arthritis. A comparison of radiologic damage, physical disability, joint counts, and acute phase reactants. J Rheumatol. 1994;21(3):425–9. [PubMed] [Google Scholar]
- 10.Guillemin F, Briancon S, Pourel J. Functional disability in rheumatoid arthritis: two different models in early and established disease. J Rheumatol. 1992;19(3):366–9. [PubMed] [Google Scholar]
- 11.Ritchie DM, Boyle JA, McInnes JM, Jasani MK, Dalakos TG, Grieveson P, et al. Clinical studies with an articular index for the assessment of joint tenderness in patients with rheumatoid arthritis. Q J Med. 1968;37(147):393–406. [PubMed] [Google Scholar]
- 12.Eichler HG, Mavros P, Geling O, Hunsche E, Kong S. Association between health-related quality of life and clinical efficacy endpoints in rheumatoid arthritis patients after four weeks treatment with anti-inflammatory agents. Int J Clin Pharmacol Ther. 2005;43(5):209–16. doi: 10.5414/cpp43209. [DOI] [PubMed] [Google Scholar]
- 13.Assari S. Ten conditions Ten Morbidity measures. Dev World Epidemiol. 2010;1(1):40–9. [Google Scholar]
- 14.Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31(3):315–24. doi: 10.1002/art.1780310302. [DOI] [PubMed] [Google Scholar]
- 15.Vittecoq O, Pouplin S, Krzanowska K, Jouen-Beades F, Menard JF, Gayet A, et al. Rheumatoid factor is the strongest predictor of radiological progression of rheumatoid arthritis in a three-year prospective study in community-recruited patients. Rheumatology (Oxford) 2003;42(8):939–46. doi: 10.1093/rheumatology/keg257. [DOI] [PubMed] [Google Scholar]
- 16.Stucki G, Liang MH, Stucki S, Bruhlmann P, Michel BA. A self-administered rheumatoid arthritis disease activity index (RADAI) for epidemiologic research. Psychometric properties and correlation with parameters of disease activity. Arthritis Rheum. 1995;38(6):795–8. doi: 10.1002/art.1780380612. [DOI] [PubMed] [Google Scholar]
- 17.Van der Heijde DM, ’t Hof MA, van Riel PL, Theunisse LA, Lubberts EW, van Leeuwen MA, et al. Judging disease activity in clinical practice in rheumatoid arthritis: first step in the development of a disease activity score. Ann Rheum Dis. 1990;49(11):916–20. doi: 10.1136/ard.49.11.916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Van Riel PL, Van Gestel AM, Van de Putte LB. Development and validation of response criteria in rheumatoid arthritis: steps towards an international consensus on prognostic markers. Br J Rheumatol. 1996;35(Suppl 2):4–7. doi: 10.1093/rheumatology/35.suppl_2.4. [DOI] [PubMed] [Google Scholar]
- 19.Ware JE, Gandek B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. J Clin Epidemiol. 1998;51(11):903–12. doi: 10.1016/s0895-4356(98)00081-x. [DOI] [PubMed] [Google Scholar]
- 20.Talamo J, Frater A, Gallivan S, Young A. Use of the short form 36 (SF36) for health status measurement in rheumatoid arthritis. Br J Rheumatol. 1997;36(4):463–9. doi: 10.1093/rheumatology/36.4.463. [DOI] [PubMed] [Google Scholar]
- 21.Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The Short Form Health Survey (SF-36): translation and validation study of the Iranian version. Qual Life Res. 2005;14(3):875–82. doi: 10.1007/s11136-004-1014-5. [DOI] [PubMed] [Google Scholar]
- 22.Zargooshi J. Quality of life of Iranian kidney “donors”. J Urol. 2001;166(5):1790–9. [PubMed] [Google Scholar]
- 23.Alishiri GH, Bayat N, Fathi AA, Tavallaii SA, Assari S, Moharamzad Y. Logistic regression models for predicting physical and mental health-related quality of life in rheumatoid arthritis patients. Mod Rheumatol. 2008;18(6):601–8. doi: 10.1007/s10165-008-0092-6. [DOI] [PubMed] [Google Scholar]
- 24.Dadoniene J, Stropuviene S, Venalis A, Boonen A. High work disability rate among rheumatoid arthritis patients in Lithuania. Arthritis Rheum. 2004;51(3):433–9. doi: 10.1002/art.20415. [DOI] [PubMed] [Google Scholar]
- 25.Adebajo AO, Reid DM. The pattern of rheumatoid arthritis in West Africa and comparison with a cohort of British patients. Q J Med. 1991;80(292):633–40. [PubMed] [Google Scholar]
- 26.Dadoniene J, Uhlig T, Stropuviene S, Venalis A, Boonen A, Kvien TK. Disease activity and health status in rheumatoid arthritis: a case-control comparison between Norway and Lithuania. Ann Rheum Dis. 2003;62(3):231–5. doi: 10.1136/ard.62.3.231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980;23(2):137–45. doi: 10.1002/art.1780230202. [DOI] [PubMed] [Google Scholar]
- 28.Van Der Heijde DM, Van’t Hof MA, Van Riel PL, Van Leeuwen MA, Van Rijswijk MH, Van De Putte LB. Validity of single variables and composite indices for measuring disease activity in rheumatoid arthritis. Ann Rheum Dis. 1992;51(2):177–81. doi: 10.1136/ard.51.2.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Davis MJ, Dawes PT, Fowler PD, Sheeran TP, Shadforth MF, Ziade F, et al. Comparison and evaluation of a disease activity index for use in patients with rheumatoid arthritis. Br J Rheumatol. 1990;29(2):111–5. doi: 10.1093/rheumatology/29.2.111. [DOI] [PubMed] [Google Scholar]
- 30.Chikanza IC, Stein M, Lutalo S, Gibson T. The clinical, serologic and radiologic features of rheumatoid arthritis in ethnic black Zimbabwean and British Caucasian patients. J Rheumatol. 1994;21(11):2011–5. [PubMed] [Google Scholar]
- 31.Bell MJ, Bombardier C, Tugwell P. Measurement of functional status, quality of life, and utility in rheumatoid arthritis. Arthritis Rheum. 1990;33(4):591–601. doi: 10.1002/art.1780330420. [DOI] [PubMed] [Google Scholar]
- 32.Hagen KB, Smedstad LM, Uhlig T, Kvien TK. The responsiveness of health status measures in patients with rheumatoid arthritis: comparison of disease-specific and generic instruments. J Rheumatol. 1999;26(7):1474–80. [PubMed] [Google Scholar]
- 33.Suurmeijer TP, Waltz M, Moum T, Guillemin F, van Sonderen FL, Briancon S, et al. Quality of life profiles in the first years of rheumatoid arthritis: results from the EURIDISS longitudinal study. Arthritis Rheum. 2001;45(2):111–21. doi: 10.1002/1529-0131(200104)45:2<111::AID-ANR162>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 34.Inoue E, Yamanaka H, Hara M, Tomatsu T, Kamatani N. Comparison of Disease Activity Score (DAS)28-erythrocyte sedimentation rate and D. Ann Rheum Dis. 2007;66(3):407–9. doi: 10.1136/ard.2006.054205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Matsui T, Kuga Y, Kaneko A, Nishino J, Eto Y, Chiba N, et al. Disease Activity Score 28 (DAS28) using C-reactive protein underestimates disease activity and overestimates EULAR response criteria compared with DAS28 using erythrocyte sedimentation rate in a large observational cohort of rheumatoid arthritis patients in Japan. Ann Rheum Dis. 2007;66(9):1221–6. doi: 10.1136/ard.2006.063834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Assari SH, Moghani Lankarani M, Montazeri A, Soroush MR, Mousavi B. Are generic and disease-specific health related quality of life correlated? The case of chronic lung disease due to sulfur mustard. JRMS. 2007;14(5):285–90. [PMC free article] [PubMed] [Google Scholar]
- 37.Aslani J, Mirzamani SM, Abadi A, Farahani M, Moghani Lankarani M, Assari SH. Health-Related Quality of Life in Chronic Obstructive Pulmonary Disease: Are Disease-Specific and Generic Quality of Life Measures Correlated? Tanaffos Respiration Journal. 2008;7(2):28–35. [Google Scholar]
- 38.Birtane M, Kabayel DD, Uzunca K, Unlu E, Tastekin N. The relation of hand functions with radiological damage and disease activity in rheumatoid arthritis. Rheumatol Int. 2008;28(5):407–12. doi: 10.1007/s00296-007-0461-z. [DOI] [PubMed] [Google Scholar]
- 39.Irvine S, Capell HC. Great expectations of modern RA treatment. Ann Rheum Dis. 2005;64(9):1249–51. doi: 10.1136/ard.2005.039339. [DOI] [PMC free article] [PubMed] [Google Scholar]