

Abstract
Background:
Utilization of Ante natal care (ANC) services is poor in the tribal areas, causing increased maternal morbidity and mortality.
Objective:
This study was carried out to find out ANC services utilization, delivery practices and factors affecting them in a tribal area of North Maharashtra in Nashik district.
Design:
Cross-sectional study.
Materials and Methods:
The study was carried out in two tribal blocks of Nashik district. Cluster sampling technique was used. 210 mothers in the selected clusters, who had delivered within last 1 year, were interviewed. Information about the ANC services utilization and place of delivery was recorded. Relevant socio-demographic data were also collected.
Results:
Adequate ANC services utilization was found to be 64.76%. Home deliveries were 34.29% and home deliveries conducted by untrained persons were 15.24%.
Conclusion:
The utilization of ANC services and deliveries at health centers were significantly associated with education of the women and their spouses, and the socioeconomic status of the family. Main reasons for inadequate utilization of ANC services were financial, unawareness about ANC services, etc. Place of delivery was associated with the type of the family. Traditional practices were the most common reason for conducting the deliveries at home.
Keywords: Ante natal care, home deliveries, tribal, utilization
Introduction
Every minute a woman dies as a result of pregnancy or childbirth. Loss per annum of 500,000 women is mind boggling.(1) Thus, maternal mortality continues to be a major public health problem. The focus on maternal mortality was sharpened when reduction in maternal mortality became one of the eight goals for development in the Millennium Declaration (Millennium Development Goal 5 or MDG 5).(2) The target for MDG 5 is to reduce the maternal mortality ratio (MMR) by three quarters from 1990 to 2015.(3)
India has the dubious distinction of having the highest estimated number of maternal deaths in any country (136,000).(4) Current maternal mortality in India is 254 per 100,000 live births.(5) In addition to the number of deaths each year, over 50 million women suffer from maternal morbidity due to acute complications from pregnancy.(6)
High-quality antenatal, intranatal and postnatal care is the most important way to reduce the maternal morbidity and mortality. There are many national programs aimed at reducing the maternal morbidity and mortality. But despite the existence of these national programs for improving maternal and child health, maternal mortality and morbidity continue to be at higher side, at an unacceptable level. There are multiple reasons for this situation. Early marriages, malnutrition, illiteracy, ignorance, lack of health services, and unavailability of transport facilities are the major contributors. One of the most important reasons for the same is nonacceptance or non-utilization/underutilization of maternal health care services, especially amongst the tribal population. In other words, utilization of these services by the target population continues to be poor.(7)
For effective implementation of the programs, understanding of the factors affecting the utilization of maternity care during pregnancy and delivery is required. If these factors are correctly identified, then the program efforts can be concentrated to increase the acceptance/utilization rates. Therefore, the present study was carried out to find out the factors associated with utilization of maternal care services in remote tribal area of Nashik District.
Aims and objectives
To find out the Ante natal care (ANC) services utilization rates and factors affecting them.
To find out the percentage of deliveries conducted at health centers.
To find out the factors responsible for home deliveries.
Materials and Methods
This cross-sectional study was carried out in two tribal blocks, Peth and Surgana, of Nashik District. These blocks are located at the northern end of the Maharashtra, bordering Gujarat. The estimated ANC utilization rates were approximately 80%. So, with a precision of 10%, 95% confidence interval and design effect of two, the required sample size was 192.(8) Thirty clusters in these two blocks were identified. Seven mothers who had delivered within last 1 year were selected randomly in each cluster. A total of 210 mothers were identified and included in the study with their consent.
All the mothers were interviewed using a predesigned, pretested, semi-open proforma. Relevant information about the ANC services utilization and place of the delivery was recorded along with the socio-demographic data. Adequate utilization of services was considered, if the pregnant women had fulfilled the following criteria.
ANC registration, at any time
Received required TT injections
Consumption of minimum 100 iron folic acid tablets
Minimum three ANC visits
Information was cross-checked with the available records to minimize the recall bias. The data were analyzed using SPSS. Chi-square test was used wherever necessary.
Results
A total of 210 mothers were interviewed in the study. Out of the 212 delivered children (two twin pregnancies), 205 were alive at the time of interview.
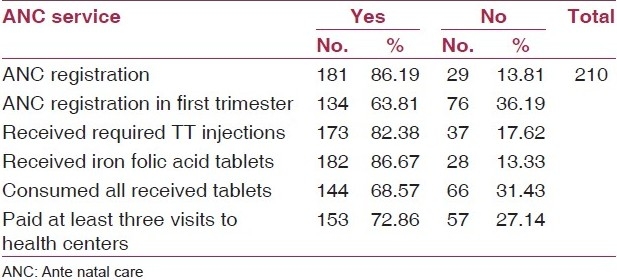
Only 134 (63.81%) pregnant women were registered in the first trimester. The figure increased to 181 (86.19%), if time of registration was ignored. It was observed that the least utilized services were ANC checkups and consumption of iron and folic acid tablets. The utilization rates for these services were 72.86% and 68.57%, respectively [Table 1].
Table 1.
ANC services utilization by the mothers
Only 136 (64.76%) pregnant women utilized the minimum four ANC services decided for this study. It meant that 74 (35.24%) pregnant women had underutilized or not utilized the services. There were 12 (5.71%) pregnant women who had not utilized a single ANC service. Six (50%) of them were belonging to Kokni Tribe and 9 (75%) were from Class V socioeconomic status. All these 12 mothers were illiterate.
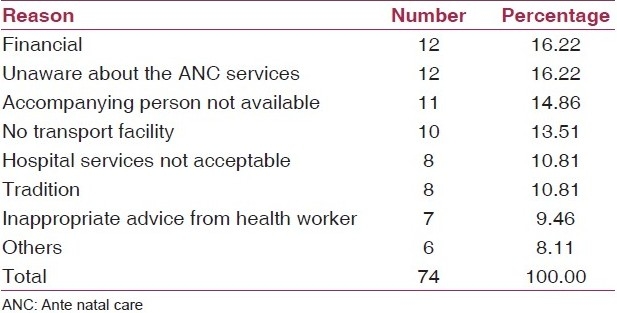
It was observed that the adequate utilization of ANC services was significantly associated with education of the mother, education of the father, and socioeconomic status of the family (P<0.05). But it was not associated with the age of the mother or the type of the family (P>0.05) [Table 2]. Main reasons for inadequate utilization of ANC services were financial, unawareness about ANC services, unavailability of suitable accompanying person, unavailability of transport facilities, etc. [Table 3].
Table 2.
Socio-demographic factors affecting adequate ANC services utilization (minimum four services)
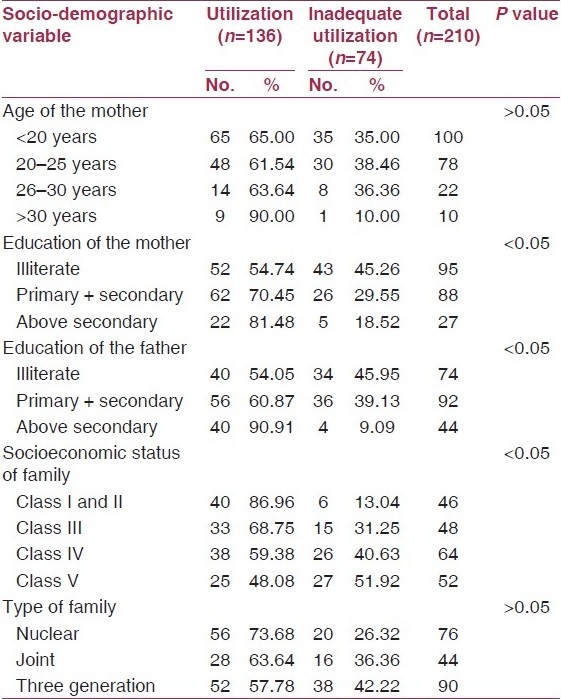
Table 3.
Main reason for inadequate utilization of ANC services
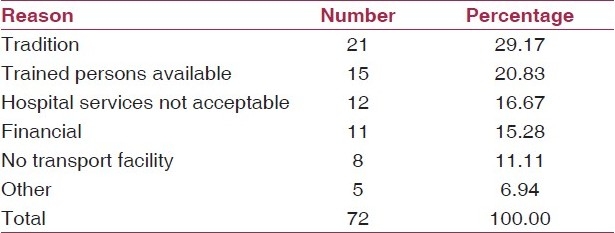
There were 138 (65.71%) deliveries conducted at the various health centers and 72 (34.29%) home deliveries. Out of them, 32 (15.24 %) deliveries were conducted by an untrained person [Table 4]. Traditional practices were the single most important main reason for conducting the deliveries at home. Other main reasons were availability of trained person at home and unsatisfactory or unacceptable hospital services [Table 5].
Table 4.
Distribution of deliveries according to the place of delivery
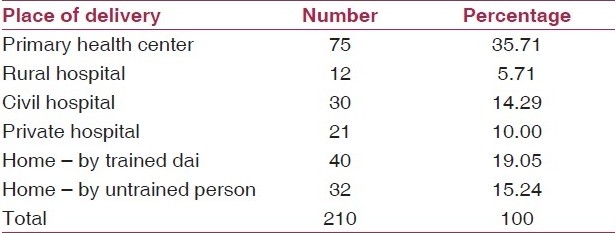
Table 5.
Main reason for conducting delivery at home
It was observed that the socioeconomic status, education of the mother and father were significantly associated with the delivery practices (P<0.05). As the education of the mother and father improved, the preference toward deliveries conducted at health centers increased. This association was equally applicable for the socioeconomic status of the family [Table 6].
Table 6.
Place of deliveries according to various socioeconomic and demographic variables
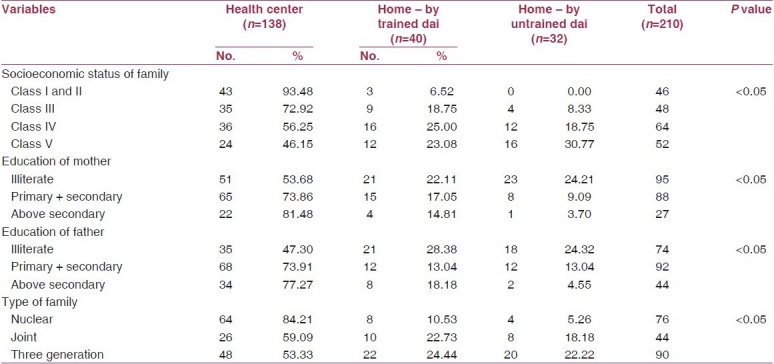
Type of family was not associated with ANC services utilization, but it was found to be significantly associated with the delivery practices. Nuclear families preferred deliveries at health center, but significantly less proportion of three generation families preferred institutional deliveries (P<0.05). In three generation families, 22.22% deliveries were conducted by untrained person [Table 6].
Discussion
The present study was carried out in two tribal blocks of the Nashik District. 210 women, who had delivered within last 1 year, were interviewed and analyzed for the ANC services utilization, delivery practices and factors affecting them.
Adequate ANC services utilization rate in the present study was 64.76%. Reports of the coverage evaluation survey carried out throughout the sampled districts of India showed more utilization of antenatal care, averaging 75% across the country.(9) This means that there is need of more efforts by the health functionaries to strengthen the ANC services and to improve the utilization of them.
Utilization of individual ANC services like ANC registration in first trimester (63.81%), TT injections (82.38%), and three ANC checkups (72.86%) was more than the Nashik rural utilization rates as found in DLHS-3 which reported these rates as 49.4%, 81.4%, 62.4%, respectively.(10) It shows that though the utilization is still less than the average figures for India, the situation is improving in this tribal area.
In this study, various socio-demographic factors such as education of mother and father and socioeconomic status of the family showed a significant association with the utilization of antenatal care services. It emphasizes the impact of education on awareness and utilization of health services by the community.
The proportions of institutional deliveries (65.71%) and home deliveries conducted by a trained person (19.05%) in this study were more than the corresponding figures of 47.3% and 11.4%, respectively, reported in DLHS-3 for Nashik rural area.(10)
Traditional practice was the main reason for conducting the deliveries at home, followed by unsatisfactory or unacceptable hospital services and lack of transport facilities. This emphasizes the need of health education as well as strengthening of health services to increase the rate of deliveries conducted at health center or at least by a trained person.
Various socio-demographic factors such as education of mother and father and socioeconomic status of the family showed a significant association with the delivery practices. It again emphasizes the impact of education on awareness and utilization of health services by the community.
One of the interesting findings in the present study was the significant association of the type of the family and delivery practices, though the type of family was not associated with ANC services utilization. It was found that the home deliveries, either by trained or untrained person, were significantly more in the three generation families as compared with the nuclear families. This explains the impact of the traditional practices in three generation families in this tribal belt. Health education will play a vital role in improving the ANC services utilization rates and delivery practices in this area.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Estimates developed by WHO, UNICEF, UNFPA. Geneva: WHO; 2003. WHO, UNICEF, UNFPA. Maternal mortality in 2000. [Google Scholar]
- 2.Ronsmans C, Graham WJ. Lancet maternal survival series steering group. Lancet. 2006;368:1189–200. doi: 10.1016/S0140-6736(06)69380-X. [DOI] [PubMed] [Google Scholar]
- 3.New York: United Nations; 2000. United Nations General Assembly. United Nations Millennium Declaration. A/RES/55/2. [Google Scholar]
- 4.Punita Arora., Surg VAdm Maternal Mortality-Indian Scenario. MJAFI. 2005;61:214–5. doi: 10.1016/S0377-1237(05)80155-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hogan MC, Foreman KJ, Naghavi M, Ahn SY, Wang M, Makela SM, et al. Maternal mortality for 181 countries, 1980-2008: A systematic analysis of progress towards Millennium Development Goal 5. [Last accessed on 2010 Apr 12];Lancet. 2010 375:1609–23. doi: 10.1016/S0140-6736(10)60518-1. Available from: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(10)60518-1/abstract# . [DOI] [PubMed] [Google Scholar]
- 6.New York: NICEF; 1996. The Progress of Nations. [Google Scholar]
- 7.Kumar R, Singh MM, Kaur A, Kaur M. Reproductive health behaviour of rural women. J Indian Med Assoc. 1995;93:129–31. [PubMed] [Google Scholar]
- 8.VK Chadha. Sample size determination in health studies. NTI Bull. 2006;42:55–62. [Google Scholar]
- 9.Gupta JP, Murali I. National review of immunization programmes. Indian J Community Med. 1990;15:217–21. [Google Scholar]
- 10.Results of district level household survey III 2007 - 08. Ministry of Health and Family Welfare. [Last accessed on 2010 Aug 10]. Available from: http://mohfw.nic.in/dlhs/MAHARASTRA/DISTRICT%20FACT%20SHEET/Copy%20of%20Final%20FACT%20SHEET-Nashik.xls .