

Abstract
Background:
There is inconsistency in accepting waist circumference (WC) as mandatory and also regarding its significance for diagnosis of metabolic syndrome (MetS) for different populations.
Aim:
To study the association of individual parameters of MetS with WC cutoffs suitable for South Asian Indians.
Materials and Methods:
From an ongoing hospital-based study on MetS as per the criteria of diagnosis of modified NCEP ATP III, 713 subjects having a minimum three of the four parameters, i.e., dyslipidemia [low high density lipoprotein (HDL), high triglycerides], dysglycemia and hypertension, without regard to cutoffs of WC, were included in the present study.
Results:
Receiver operator characteristic curve analysis of WC cut-off points for males was 90 cm with a sensitivity and specificity of 71% and 96%, respectively, and for females was 85 cm with a sensitivity and specificity of 86% and 93%, respectively, associated with the risk factors of MetS. Multiple logistic regression analysis for low density lipoprotein (LDL) cholesterol concentration of ≥3.38 mmol/l showed an odds ratio of 5.03 (95% CI = 1.29–19.5) in males and 3.17 (95% CI = 1.14–8.76) in females which was statistically significant (P < 0.02); in addition to higher WC, higher level of triglyceride (P ≤ 0.0001) and lower level of high density lipoprotein cholesterol (P ≤ 0.02) were observed.
Conclusion:
This study suggests that WC of 90 cm in males and 85 cm in females should be a mandatory criterion of MetS in our subset of population. LDL may be considered one of the components of MetS along with the currently defined WC cutoffs.
Keywords: Asian Indians, low density lipoprotein cholesterol, metabolic syndrome, receiver operator characteristic curve, waist circumference
INTRODUCTION
Subjects with the metabolic syndrome (MetS) have increased risk of development of type 2 diabetes and cardiovascular diseases.[1,2] Various studies suggest abdominal obesity[3,4] and insulin resistance,[5] which are components of this syndrome, as interdependent risk factors for cardiovascular disease (CVD). Subsequent studies on the other components of the MetS showed hypertension, hypertriglyceridemia and low high density lipoprotein (HDL) cholesterol to be independent risk factors for CVD.[6] At present, there are three internationally recognized and most popular definitions of the MetS, namely, those of the World Health Organization (WHO),[7] the National Cholesterol Education Program's Adult Treatment Panel III (NCEP ATP III)[6] and the International Diabetes Federation (IDF).[1] The definition for MetS according to IDF[1] has abdominal obesity as its pre-requisite with ethnicity-specific cut-off values for waist circumference (WC) and that relates to a major difference between IDF[1] and NCEP ATP III[2,6] defined MetS criteria. The IDF has strongly recommended that more extensive investigations should be performed before suitable cut-off levels are established for use in clinical practice.[8] The Indian consensus[9,10] recommends a new cutoff of WC but not mandatory for the diagnosis of MetS, similar to modified NCEP ATP III[6,11,12] definition of MetS. In a recent publication, experts associated with IDF have upheld their views that WC might not be mandatory criteria of MetS.[8] We designed the current study to make a cutoff of WC value and its status as mandatory for the diagnosis of MetS in our subset of population.
MATERIALS AND METHODS
The study was approved by the institutional ethics committee. Study subjects included patients and their first-degree relatives visiting endocrine out-patient clinic of the university hospital, located in the northeastern part of India. All individuals enrolled were ≥20 years of age. All participants enrolled were recruited from an ongoing hospital-based study. Detailed clinical data of the participants, including age, sex, anthropometry, family history, duration of complications like diabetes, hypertension, dyslipidemia, previously prescribed drugs for therapy, were noted on a preset proforma. Individuals with the habit of smoking, alcohol consumption, tobacco chewing were excluded from the study. Informed consent was obtained from all the participants. WC was measured as the midpoint between lowest rib and iliac crest in the standing position at the end of a gentle expiration. Mean of two blood pressure (BP) readings taken 5 min apart in resting state was used. An oral glucose tolerance test (OGTT) was done to determine the glycemic status as normal glucose tolerant (NGT), prediabetic (IFG and IGT) and diabetic by the WHO criteria.[7] MetS was screened for dyslipidemia as (a) fasting triglycerides (TG) ≥ 150 mg/dl; (b) HDL < 40 mg/dl in males and <50 mg/dl in females; and (c) hypertension ≥ 130/85 mmHg, and for dysglycemia as fasting plasma glucose (FPG) ≥ 100 mg/dl (5.6 mmol/l) or previously diagnosed diabetes or on specific treatment for the respective abnormality without regard to cutoff of WC. Blood samples were collected after 10 hours of fasting, but before 11 AM for the estimation of plasma glucose, total cholesterol, TG and HDL. Low density lipoprotein (LDL) cholesterol (Freidewald's method) and very low density lipoprotein (VLDL) cholesterol were calculated.[13]
Statistical analysis
Receiver operator characteristic curves were plotted for WC using sensitivity and 1 -specificity to identify the presence of any two out of four above-mentioned CVD risk factor components of MetS definition. Logistic regression analysis was done to associate the variables with factors of MetS. Data were analyzed using SPSS 15.0 (SPSS, Chicago, IL, USA).
RESULTS AND DISCUSSION
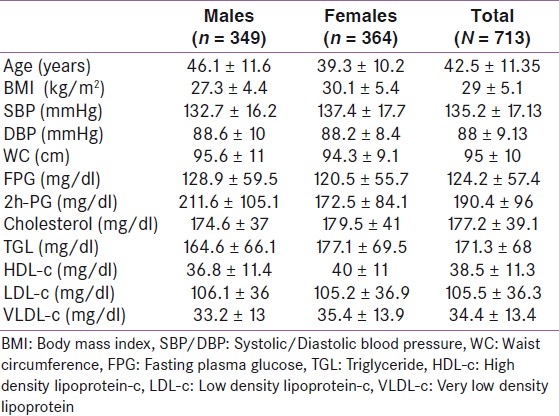
A total of 713 subjects (349 males and 364 females) as per the criteria given in the section “Materials and Methods” were selected from an ongoing hospital-based study, with the mean age of the subjects being 42.5 ± 11.3 (±SD) years. Based on OGTT, 58.6% were found to be NGT, prediabetics, i.e., those with IFG and IGT formed 20.3% and 18.6%, respectively, while 42.3% of the study subjects were found to be diabetic. Low HDL was found in 37.5% and 41% males and females, respectively; raised triglycerides was found in 34.9% and 19.2% males and females, respectively; hypertension was found in 42.6% and 33.4% males and females, respectively; body mass index (BMI) of ≥25 kg/m2 was observed in 40.4% and 67.4% males and females, respectively. Demographic and biochemical profile of the enrolled subjects have been shown in Table 1.
Table 1.
Demographic and biochemical parameters of the enrolled subjects
In the receiver operator characteristic (ROC) curve analysis [Figure 1], the most predictive cut-off point for WC was 90 cm for males (71% sensitivity, 96% specificity) while it was 85 cm (86% sensitivity, 93% specificity) for females. A cut-off value of 87 cm in males showed 89% and 66% sensitivity and specificity, respectively, while 83 cm cut-off value in females showed 89% and 90% sensitivity and specificity, respectively, for various parameters of MetS. Multiple logistic regression analysis showed lower level of HDL with an odds ratio (OR) of 2.58 (95% CI = 1.2–5.52; P ≤ 0.02) in males and higher WC had an OR of 4.16 (95% CI = 2.95–5.85; P ≤ 0.0001) in females. The remaining parameters showed a similar and significant (P ≤ 0.0001) pattern of OR in both males and females.
Figure 1.
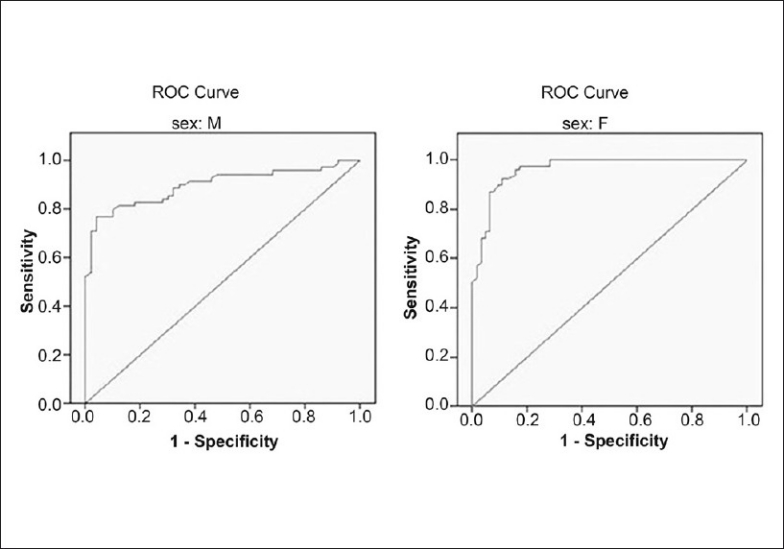
Receiver operator characteristic curve for determination of waist circumference cutoffs in males and females
CONCLUSION
Based on the ROC analysis of this study, it is suggested that WC >90 cm in males and >85 cm in females should be a mandatory criterion in making the diagnosis of MetS. Our study showed that the WC cut-off value for men and women should have a minimal difference of 5 cm. Additionally, using these cutoffs, LDL (calculated) level ≥2.6 to ≤3.38 mmol/l has an OR of 1.73 (95% CI = 0.78–3.84) in males and 1.75 (95% CI = 0.76–4.03) in females. Although LDL is not a parameter of MetS according to any of the present definitions, it showed a high OR of 5.03 (95% CI = 1.29–19.5; P ≤ 0.02) in males and 3.17 (95% CI = 1.14-8.76; P < 0.02) in females when the value was ≥130 mg/dl. To our knowledge, the present study of determining WC cut-off values for MetS is the first of its kind considering LDL as one of the determinants of MetS. There is only one caveat to this fact that the LDL was calculated (Friedewald's formula) and not directly measured. We also suggest that LDL (estimated) may be considered as a part of MetS if other parameters are not met in an individual with higher WC cutoff.
There are a few limitations in this pilot study. Measurement of fat distribution in peripheral or visceral region was not performed using Dual energy X-ray absorptiometry (DEXA) or subcutaneous skin fold thickness. This measurement would have given additional information indicating a stronger relation between WC and biochemical profile. A follow-up study considering changes in biochemical profile of MetS in study subjects in relation to WC changes is also proposed in our opinion to substantiate the present observation. Even though these were not possible in this pilot study, the statistical outcome of ORs by multiple logistic regression analysis as well as WC cutoff by ROC curve suggested the importance of WC cut-off value to be redefined. In a very recent publication, the ethnic-specific WC has been suggested to be 83–84 cm in males and females for diagnosis of MetS based on the ROC analysis of the Japanese population.[14]
In conclusion, our study emphasizes WC as an obligatory diagnostic criterion for South Asian Indians, like IDF but not as modified NCEP ATP III definition for MetS. Nevertheless, further population-based studies taking large sample size are required to prepare a more ethnic-specific definition of MetS.
ACKNOWLEDGMENTS
We thank Mr. Ram Mohan R., Biostatistician, NIH-TMRC project, Department of Medicine, IMS, BHU, for helping in the statistical analysis of the study. Research fellowship to DDP was provided by University Grants Commission, New Delhi, India.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Alberti KG, Zimmet P, Shaw J. The IDF epidemiology task force consensus group: Metabolic syndrome: A new worldwide definition. Lancet. 2005;366:1059–62. doi: 10.1016/S0140-6736(05)67402-8. [DOI] [PubMed] [Google Scholar]
- 2.Expert panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation and treatment of high blood cholesterol in adults (Adult Treatment Panel III) JAMA. 2001;285:2486–97. doi: 10.1001/jama.285.19.2486. [DOI] [PubMed] [Google Scholar]
- 3.Lebovitz HE, Baneji MA. Point: Visceral adiposity is causally related to insulin resistance. Diabetes Care. 2005;28:2322–5. doi: 10.2337/diacare.28.9.2322. [DOI] [PubMed] [Google Scholar]
- 4.De Koning L, Merchant AT, Pogue J, Anand SS. Waist circumference and waist-to-hip ratio as predictors of cardiovascular events: Meta regression analysis of prospective studies. Eur Health J. 2007;28:850–6. doi: 10.1093/eurheartj/ehm026. [DOI] [PubMed] [Google Scholar]
- 5.Bonora E, Kiechl S, Willeit J, Oberhollenzer F, Egger G, Meigs JB, et al. Insulin resistance as estimated by homeostasis model assessment predicts incident symptomatic cardiovascular disease in Caucasian subjects from the general population: The Bruneck study. Diabetes Care. 2007;30:318–24. doi: 10.2337/dc06-0919. [DOI] [PubMed] [Google Scholar]
- 6.Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckl RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung and Blood Institute Scientific statement. Circulation. 2005;112:e285–90. doi: 10.1161/CIRCULATIONAHA.105.169404. [DOI] [PubMed] [Google Scholar]
- 7.Geneva: WHO Department of Noncommunicable Disease Surveillance; 1999. [Last cited on 2011 Jul 20]. World Health Organisation. Definition, diagnosis and classification of diabetes mellitus and its complications. Report of a WHO consultation. 1999. Part 1: Diagnosis and classification of Daibetes Mellitus; pp. 1–59. Available from: http://www.who.int. [Google Scholar]
- 8.Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: A joint interim statement of the Internaional Diabetes Federation Task Force on Epidemiology and Prevention; national Heart, Lung and Blood Institute; American Heart Association; World Health Federation; International Atherosclerosis society; and International Association for the study of obesity. Circulation. 2009;120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644. [DOI] [PubMed] [Google Scholar]
- 9.Misra A, Vikram NK, Gupta R, Pandey RM, Wasir JS, Gupta VP. Waist circumference cut off points and action levels for Asian Indians for identification of abdominal obesity. Int J Obes. 2006;30:106–11. doi: 10.1038/sj.ijo.0803111. [DOI] [PubMed] [Google Scholar]
- 10.Misra A, Chowbey P, Makkar BM, Vikram NK, Wasir JS, Chadha D, et al. Consensus group. Consensus statement for diagnosis of Obesity, Abdominal Obesity and the Metabolic syndrome for Asian Indians and Recommendations for Physical Activity, Medical and Surgical management. J Assoc Physicians India. 2009;57:163–70. [PubMed] [Google Scholar]
- 11.Heng D, Ma S, Lee JJ, Tai BC, Mak KH, Hughes K, et al. Modifi cation of the NCEP ATP III defi nitions of the metabolic syndrome for use in Asians identifies individuals at risk of ischemic heart disease. Atherosclerosis. 2006;18:367–73. doi: 10.1016/j.atherosclerosis.2005.07.020. [DOI] [PubMed] [Google Scholar]
- 12.Tan CE, Ma S, Wai D, Chew SK, Tai ES. Can we apply the National Cholesterol Education Program Adult Treatment Panel definition of the metabolic syndrome to Asians? Diabetes Care. 2004;27:1182–6. doi: 10.2337/diacare.27.5.1182. [DOI] [PubMed] [Google Scholar]
- 13.Warnick GR, Knopp RH, Fitzpatrick V, Branson L. Estimating low-density lipoprotein cholesterol by the Friedewald equation is adequate for classifying patients on the basis of nationally recommended cutpoints. Clin Chem. 1990;36:15–9. [PubMed] [Google Scholar]
- 14.Kawada T, Otsuka T, Inagaki H, Wakayama Y, Li Q, Li YJ, et al. Optimal cut-off levels of body mass index and waist circumference in relation to each component of metabolic syndrome (MetS) and the number of MetS component. Diab Met Syndr: Clin Res Rev. 2011;5:25–28. doi: 10.1016/j.dsx.2010.05.012. [DOI] [PubMed] [Google Scholar]