

Abstract
Context:
Traditionally, circumcision wounds are closed by absorbable sutures. However, certain alternative methods are also being utilized to overcome the shortcomings of the conventionally used method for circumcision wound closuring. In the current study, the use of tissue glue ((iso amyl 2-cyanoacrylate) has been compared with traditional suturing for the approximation of circumcision wounds. In our study, both the methods were found to be comparable with significantly less time consumed in glue group.
Aims:
The purpose of the present study has been to compare directly cyanoacrylate as a better alternative to conventional suture material in terms of cosmetic result, time consumed and incidence of infection (comparative study).
Materials and Methods:
The results of all the patients seen in outpatient department for circumcision were included in this study. The study was conducted from Aug 2009 to May 2010. The tissue glue (iso amyl 2-cyanoacrylate) was compared to sutures as a method of wound approximation in circumcision.
Results:
Tissue glue group has been observed to have less wound inflammation, bleeding or hematoma rate and was cosmetically superior as compared to suture group; however, none of these findings could reach statistically significant level. The mean time taken for circumcision was 14.2 min (SD 2.42), when tissue glue was used for wound approximation. However, it was 24.4 min (SD 5.06) in case of the use of sutures. This difference was found as highly significant (P value < 0.001). However, regarding postoperative pain no significant reduction was observed when glue was used.
Conclusions:
This study showed that the use of tissue glue in comparison to sutures is having the following advantages:
Cosmetically superior
Less time consuming
All other parameters measured were nearly the same and statically insignificant.
Keywords: Cyanoacrylate, sutureless circumcision, tissue glue
INTRODUCTION
In the modern time with the advent of elective surgery, more energy has been directed for achieving an efficient and uncomplicated healing of the deliberately inflicted wound.[1] Every surgeon dreams of perfect wound healing while performing surgeries. Although spectacular achievements are made in science and technology in recent years, yet the oldest surgical problem of perfect wound closure still persists. The use of tissue adhesive as an attractive alternative to sutures has recently been invoked immense interest in the field of wound healing.
Circumcision is a commonly performed operation and absorbable sutures have traditionally been used for closure. The two most common complications of circumcision are bleeding and wound infection.[2] The cyanoacrylate tissue glue has been claimed to have the advantages of being hemostatic,[3] bacteriostatic[4,5] and easy to use.
Objective
The ethical committee of our hospital gave approval for this study to be undertaken in dept. of urology. The purpose of the present study has been to compare directly iso amyl 2-cyanoacrylate as a better alternative to conventional suture material in terms of cosmetic result, time consumed, incidence of infection and complications.
MATERIALS AND METHODS
All the patients seen in outpatient department for circumcision were fully informed about the study and informed consent was obtained. The study was conducted from Aug 2009 to May 2010. Totally, 88 patients of 12 to 64 years (mean 30.8 years, SD 13.2) of age underwent elective circumcision because of various reasons [Figure 1].
Figure 1.
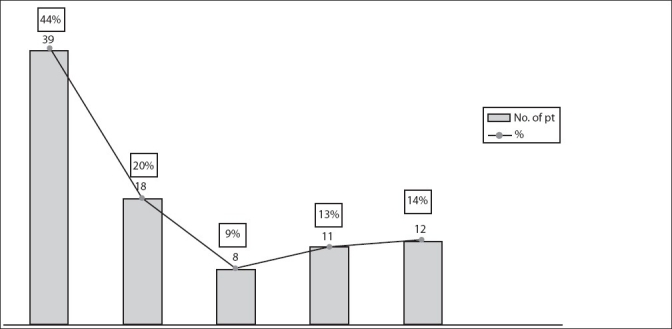
Circumcision-etiology, BXO-Balantis xerotica obliterens, Cong phimosis-congenital phimosis, Rec BP-Recurrent balanoprosthatitis
Totally, 44 patients were selected for the experimental group (glue group) and 44 for control group (suture group). The wound approximation was compared between these two groups. All circumcisions were done by one surgeon to avoid the bias. Patients with active infection were excluded from the study. The operation was performed in local or local anesthesia supplemented with IV sedation in apprehensive patients. Skin was marked by surgical pen to ensure tension free skin closure. The technique of dorsal slit followed by removal of foreskin and frenulotomy has been used. Meticulous hemostasis was ensured by bipolar cautery.
In the control group, the mucocutaneous approximation was done by interrupted 3/0 chromic catgut. In the experimental group, cyanoacrylate glue was used for wound approximation. Antibiotic ointment was applied to urethral meatus to avoid accidental contact with glue. Mucocutaneous approximation was achieved by using pair of toothed forceps holding the two edges of wound firmly together [Figure 2].
Figure 2.
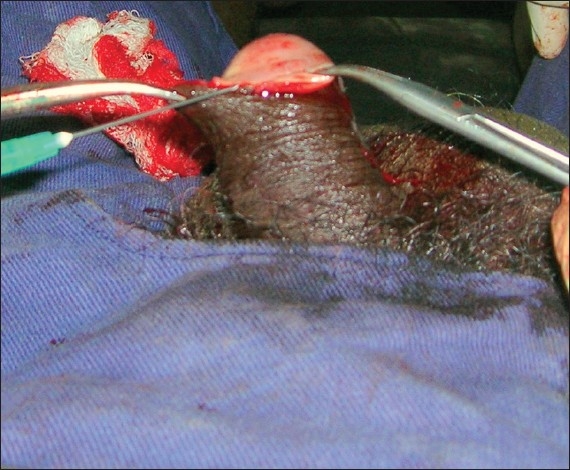
Mucocutaneous approximation
Oozing blood was cleaned with saline and wound area was dried by gauge as far as possible. After approximation, few drops of iso amyl 2-cyanoacrylate were applied at interval on one side to facilitate holding, then a thin layer applied through the wound and allowed to dry for about 10-15 s. The width of glue was not wider than 5 mm. Application of glue between the edges was avoided as it could delay the healing. Accidental spillage of glue over glans causes denudation of mucosa in one case, which was managed conservatively [Figures 3a and 3b]. No dressing was used in these cases.
Figure 3a.

Spillage of glue- after five days
Figure 3b.

Spillalage of Glue over glans after 3 days
Patients were allowed to bath after 48 h of surgery. Iso amyl 2-cyanoacrylate glue held the skin edges together for seven-eight days and then started to fall off. Postoperative pain was assessed after 5 h interval for two times using visual analogue scale in all patients. Wound infection was defined as wound discharge with positive culture. Inflammation was defined as redness around the wound edges. All patients received postoperative antibiotic. Wound healing was followed by repeated observations on 3rd, 7th, and 30th day postoperatively. After one month, assessment of cosmesis was carried out by another surgeon, who had not performed the surgery. Five patients from glue group and eight from suture group did not come for review at one month.
RESULTS
Totally, 88 patients admitted for elective circumcision were studied. The age ranged from 12 to 64 years. The comparison of complications using the cyanoacrylate and the suturing for wound approximation of circumcision is shown in Table 1. No major complication was noted in both the groups. Tissue glue group had higher rate of partial dehiscence as compared to suture group but a comparable or less wound inflammation, bleeding or hematoma rate. However, none of these findings could reach to statistically significant level.
Table 1.
Postoperative complications in two groups

The mean time taken for circumcision was 14.2 min (SD 2.42) when tissue glue was used. However, the mean time taken for circumcision was 24.4 min (SD 5.06) when sutures were used. This difference was found as highly significant (t test, P value < 0.0001).
Regarding postoperative pain, there was no significant reduction when glue was used [Table 2] and circumcision done in glue group was found to be cosmetically superior than sutured group in which sutured marks are usually seen.
Table 2.
Visual analogue score of postoperative pain

DISCUSSION
Male circumcision is removal of the foreskin (prepuce) from the penis. Early description of circumcision was found in cave drawings and Ancient Egyptian tombs.[6] According to the World Health Organization (WHO), global estimates suggest that 30% of males are circumcised.[7] In India incidence of circumcision in general population is approximately 33%.[8] Most circumcisions are performed during adolescence for cultural or religious reasons. The prevalence of circumcision varies mostly with religious affiliation, and sometimes due to culture. Adult and adolescent circumcision is carried out using one of the methods: Dorsal slit method or sleeve method. Local anesthesia is the preferred method. The widely used dorsal slit method is used in the present study. All the methods of adult and adolescent circumcision require suturing and dressing. Surgical complications of male circumcision can include excessive bleeding, hematoma formation, sepsis, unsatisfactory cosmetic effect, lacerations of the penis and injury to the glans, too little or too much of foreskin excised, meatal stenosis, urinary retention, phimosis and buried penis.[2] Among all these complications, hemorrhage and infection are the most common complications.[2]
The circumcision wound was closed by absorbable sutures, traditionally. Currently, alternative methods are being utilized to overcome the shortcomings of the conventional closure like complications, postoperative pain, time consumed and cosmetic problems. The most recent advancement is the technique of closure carrying out without sutures. In the year 1940′s, variety of cyanoacrylate adhesives were developed which are series of homologous compounds known as alkyl-cyanoacrylates.[9] These glues get polymerize on contact with basic substances such as blood or water. The polymerization occurs at room temperature and does not require the use of solvent or an added catalyst. The material can be spread easily in a thin film, readily wets the surfaces to which it is applied, and produces very little heat. It should not be placed inside the wound. Coover et al., has discovered the adhesive properties of cyanoacrylate adhesive and suggested their use as a surgical adhesive for the first time.[10] Adhesive glue is especially useful for day care surgery like circumcision. Cyanoacrylate is a better alternative to sutures and gained increased clinical popularity due to the ease of application, decreased scarring, decreased pain and better cosmetic results with no discomfort as seen with sutures getting to or snagging the clothings and dressing. Most of the studies done earlier were limited to pediatric age group. Frase and Geode in their study found that 2-octyl cyanoacrylate is the feasible option over suture material for circumcision, especially in children.[11] Similar to our finding, Arunachalam et al. showed that 2-octyl cyanoacrylate is cosmetically superior and its operative time is significantly less in comparison to suture group.[12] In opposition to this, Cheng and Saing concluded that tissue glue has no significant advantage over suturing and time taken was longer in tissue glue group.[13] Recently Jonathan et al. published their wide experience with sutureless circumcision and they concluded that it is safe, efficient, financially beneficial and a cosmetically appealing alternative to sutures which support our finding.[14] Sharma PP in their study showed it as a feasible alternative to suture for adult population with less postoperative pain.[15] In the present study, the cyanoacrylate and the suture group had similar mean age and clinical indication for circumcision. There is no significant difference in pain score or complications in both groups. Wound dehiscence is slightly more in tissue glue group mostly at frenular junction, which is healed without any intervention. The wound separations were mostly in early part of study and were due to faulty application of glue. Although not significant, there was less bleeding in tissue glue group as it may have hemostatic effect. The most striking difference in this study is operation time. On an average, the tissue glue group takes 10 min shorter than the control group. Initially the time taken was more in learning phase but gradually it got reduced. Demerits of this procedure are the following: Less availability of tissue glue in India, storage problem due to short shelf life outside refrigeration (glue harden at temp >25°C), cost (cost of 0.25 ml of glue is Rs. 125 compared to 3-0 catgut Rs. 55), proper application of glue as it may incorporate surrounding tissue.
Another advantage of glue is that the stitch marks are absent as compared to sutures. This method obviates the use of traditional dressings like supra tulle, many of which are incorporated within sutures, and hence cause pain during their removal. Absence of sutures also avoids early snagging and gives good cosmetic result.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Bucknall TE. Abdominal wound closure: Choice of suture. J R Soc Med. 1981;74:580–5. doi: 10.1177/014107688107400805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Weiss HA, Larke N, Halperin D, Schenker I. Complications of circumcision in male neonates, infants and children: A systematic review. BMC Urol. 2010;16:10–2. doi: 10.1186/1471-2490-10-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bessmann M. Cyanoactylate spray in the treatment of prolonged oral bleeding. Int J Oral Surg. 1977;6:233–40. doi: 10.1016/s0300-9785(77)80015-x. [DOI] [PubMed] [Google Scholar]
- 4.Mertz PM, Davis SC, Cazzaniga AL, Drosou A, Eaglstein WH. Barriers and antibacterial properties of 2-octyl cyanoacrylate derived wound treatment films. J Cutan Med Surg. 2003;7:1–6. doi: 10.1007/s10227-002-1154-6. [DOI] [PubMed] [Google Scholar]
- 5.Narang U, Mainwaring L, Spath G, Barefoot J. In vitro analysis for microbial barrier properties of 2-octyl cyanoacrylate derived wound treatment films. J Cutan Med Surg. 2003;7:13–9. doi: 10.1007/s10227-002-1155-5. [DOI] [PubMed] [Google Scholar]
- 6.Hodges FM. The ideal prepuce in ancient Greece and Rome: Male genital aesthetics and their relation to lipodermos, circumcision, foreskin restoration, and the kynodesme. Bull Hist Med. 2001;75:375–405. doi: 10.1353/bhm.2001.0119. [DOI] [PubMed] [Google Scholar]
- 7.WHO/UNAIDS. Male circumcision: Global trends and determinants of prevalence, safety and acceptability. World Health Organization. 2008 [Google Scholar]
- 8.Reynolds SJ, Shepherd ME, Risbud AR, Gangakhedkar RR, Brookmeyer RS, Divekar AD, et al. Male circumcision and risk of HIV-1 and other sexually transmitted infections in India. Lancet. 2004;363:1039–40. doi: 10.1016/S0140-6736(04)15840-6. [DOI] [PubMed] [Google Scholar]
- 9.Quinn J, Wells G, Sutcliffe T, Jarmuske M, Maw J, Stiell I, et al. A randomized trial comparing octylcyanoacrylate tissue adhesive and sutures in the management of lacerations. JAMA. 1997;277:1527–30. [PubMed] [Google Scholar]
- 10.Coover HW, Joyner FB, Shearer NH, Wicker TH. Chemistry and performance of cyanoacrylate. J Soc Plan Surg Eng. 1959;15:413–7. [Google Scholar]
- 11.Fraser ID, Goede AC. Sutureless circumcision. BJU Int. 2002;90:467–8. doi: 10.1046/j.1464-410x.2002.02891.x. [DOI] [PubMed] [Google Scholar]
- 12.Arunachalam P, King PA, Orford J. A prospective comparison of tissue glue versus sutures for circumcision. Pediatr Surg Int. 2003;19:18–9. doi: 10.1007/s00383-002-0893-1. [DOI] [PubMed] [Google Scholar]
- 13.Cheng W, Saing H. A prospective randomized study of wound approximation with tissue glue in circumcision in children. J Paediatr Child Health. 1997;33:515–6. doi: 10.1111/j.1440-1754.1997.tb01661.x. [DOI] [PubMed] [Google Scholar]
- 14.Kaye JD, Kalisvaart JF, Cuda SP, Elmore JM, Cerwinka WH, Kirsch AJ. Sutureless and scalpel-free circumcision--more rapid, less expensive and better.? J Urol. 2010;184(4 Suppl):1758–62. doi: 10.1016/j.juro.2010.03.081. [DOI] [PubMed] [Google Scholar]
- 15.Sharma PP. Sutureless circumcision: Wound closure after circumcision with cyanoacrylate glue-A preliminary Indian study. Indian J Surg. 2004;66:286–8. [Google Scholar]