

Abstract
Background. In Uganda Malaria continues to be a major public health problem accounting for about 30–50% of all outpatient consultations and 35% of hospital admissions and a leading cause of mortality and morbidity. Pregnant women and their unborn children are vulnerable to malaria. Methods. A cross-sectional survey was conducted in 20 postconflict IDP camps of Gulu district selected randomly as clusters. 769 pregnant women were interviewed. Results. The majority of the respondents 85% have ever heard about malaria. Most (80%) 571 respondent attributed malaria to be transmitted by mosquito bites, 15 said cold weather, 53 said dirt, and 35 said not sleeping under net. Most (91%) 683 respondents mentioned that malaria was caused by mosquito, 28 mentioned cold food, 3 mentioned playing in the rain, 19 mentioned cold weather, and 6 mentioned eating mangos. Conclusion. Most pregnant women in the post conflict IDP camps have relatively high knowledge about malaria transmission, signs, symptoms, and consequences during pregnancy. However, majority of respondents had misconception about the cause of malaria while a few had misconception about the mode of malaria transmission.
1. Background
An estimated 30 million women living in malaria endemic areas of Africa become pregnant each year [1]. Pregnant women and their unborn children are vulnerable to malaria, which is a major cause of perinatal mortality, low birth weight, and maternal anaemia [2]. The poor bear the highest burden of malaria. They are at higher risk of becoming infected with malaria because they live in dwelling that offer little protection from mosquitoes [3]. Malaria prevention during pregnancy is a major public health challenge and the Roll Back Malaria (RBM) global Partnership has recommended a three prong approach for reducing the burden of malaria among pregnant women which are effective case management, use of insecticide treated nets (ITNs), and intermittent presumptive treatment (IPT) [4]. In Uganda, the government has promoted the use of insecticide treated nets (ITNs) and intermittent presumptive treatment (IPT) among pregnant women. However, malaria still continues to be a major public health problem accounting for about 30–50% of all outpatient consultations and 35% of hospital admissions in the country [5]. Several studies conducted in malaria-endemic areas of Africa regarding knowledge, attitudes, and practices toward malaria control measures among pregnant women indicate that malaria is perceived as a serious illness, and knowledge of malaria risks during pregnancy is relatively high [6–10]. A number of studies also reveal that misconceptions concerning malaria still exist and that practices for the control of malaria have been unsatisfactory [11, 12]. This study was conducted to assess the level of knowledge and misconception about malaria among pregnant women in a post conflict internally displaced persons' (IDP) camps in Gulu.
2. Methods
The study was conducted in IDP camps of Gulu district. Gulu district has two counties (Aswa and Omoro) and a municipality. The district is part of the region which was affected, by the two decades of arm conflict. The populations were forced into concentration camps with little social and health services and therefore lived in appalling conditions. From July 2007 to June 2008, Gulu had 31 IDP camps [13] with a total of 10,888 pregnancies [14]. A cross-sectional study was conducted in 20 randomly selected IDP camps. A camp constituted a cluster. Ten (10) IDP camps were randomly selected in each county. The numbers of pregnant women interviewed per IDP camp were determined using proportion to size cluster sampling method. We determine the centre of each IDP camp first and then the starting household. Consecutive sampling method was used by moving to the next nearest household. A total of 769 pregnant women were interviewed. Inclusion criteria were pregnant women who gave self-report of carrying pregnancy. Being residents of the 20 selected camps. Being present on the interview date and giving a written informed consent to participate in the study. The exclusion criteria were being seriously sick or in labour. The study was approved by the Faculty of Medicine Research and Ethic Committee, Makerere University which granted permission to study pregnant women less than 18 years as emancipated minors.
A semistructured questionnaire was administered by trained research assistants who were fluent in the local language (Acholi). The questionnaire was translated into Acholi with the help of an expert linguistic and back-translated into English and pretested in municipality before administering to the study population. Data was collected on sociodemographic characteristics and knowledge on malaria. Data was entered into Epidata version 3.1 cleaned, edited, coded, and exported to STATA 11 for analysis. Continuous variables were summarised using means and categorical variables were displayed into tables and charts for general description (Figure 1).
Figure 1.
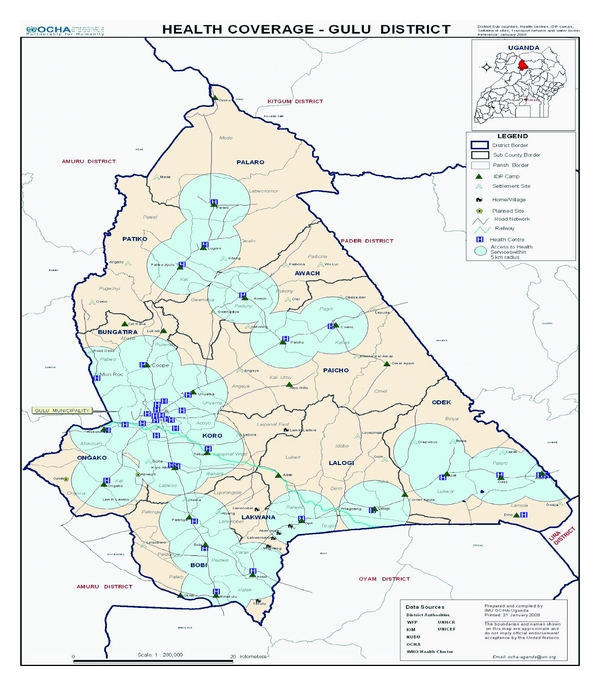
Map of Gulu District showing Health Units and IDP Camps. Permission was granted from UNOCHA Gulu office to use the map for the research purpose only.
3. Results
769 pregnant women were interviewed with age ranging from 14 to 45 years with a mean age of 25.3 years and standard deviation (SD) of 6.2. The modal age of respondents was in the bracket of 20–24 (29%) years and those 35 years and above constituted 10%. Of the 769 respondents, 26% had not got formal education while 70% had primary education level and only two (2) had tertiary education. Most pregnant women were cohabiting (62%) followed by married pregnant women (30%). Most respondents were Para 3 or more. Detailed socio-demographic characteristics are presented in Table 1.
Table 1.
Socio-demographic characteristics of respondents.
| Variable | Frequencies | Percentage |
|---|---|---|
| n | (%) | |
| Age | ||
| 14–19 | 152 | 20 |
| 20–24 | 225 | 29 |
| 25–29 | 190 | 25 |
| 30–34 | 124 | 16 |
| 35–45 | 075 | 10 |
| Education levels | ||
| Not educated | 200 | 26 |
| Primary | 540 | 70 |
| Secondary | 027 | 04 |
| Tertiary | 002 | 00 |
| Marital status | ||
| Married | 233 | 30 |
| Single | 057 | 07 |
| Cohabiting | 477 | 62 |
| Divorce | 001 | 00 |
| Widow | 001 | 00 |
| Parity | ||
| Para 0 | 127 | 17 |
| Para 1-2 | 232 | 30 |
| Para ≥3 | 410 | 53 |
Also, of the 769 respondents, 85% have ever heard about malaria and 47% of these people heard about malaria for the first time from the health centre (Table 2). Knowledge about malaria signs and symptoms were fairly distributed with 146 (20%) of the respondents citing feeling cold, 141 (19%) fever, 66 (9%) mentioned they did not know any of the signs or symptoms of malaria. Other signs and symptoms of malaria mentioned are presented in Table 2.
Table 2.
Awareness about malaria signs and symptoms.
| Variables | Frequency | Percentage |
|---|---|---|
| n | % | |
| Have ever heard about Malaria | ||
| Yes | 648 | 85 |
| No | 116 | 15 |
| Sources of information about malaria | ||
| Cannot recall | 022 | 03 |
| From community | 100 | 15 |
| Radio | 230 | 36 |
| Health centre | 296 | 46 |
| Malaria Signs and Symptoms mentioned | ||
| Diarrhoea | 013 | 02 |
| Others | 026 | 04 |
| Dizziness | 028 | 04 |
| Malaise | 038 | 05 |
| Jaundice | 057 | 08 |
| I do not know | 066 | 09 |
| Vomiting | 109 | 15 |
| Headache | 109 | 15 |
| Fever | 141 | 19 |
| Chill | 146 | 20 |
Also, 571 (80%) of the respondent attributed malaria to be transmitted by mosquito bites, 15 mentioned cold weather, 53 mentioned dirt, 35 said not sleeping under net, and 5% did not know (Table 3). 683 of the respondents mentioned that malaria was caused by mosquito, 3 respondents said that malaria was caused by playing in the rain, 28 respondents said that cold food was the cause of malaria, 19 respondents said that cold weather, 6 said eating mango, and 10 respondents said they did not know the cause of malaria (Table 3).
Table 3.
Malaria knowledge among pregnant women.
| Variables | Frequencies | Percentage |
|---|---|---|
| n | % | |
| Mode of transmission | ||
| Cold weather | 015 | 02 |
| When you do not sleep under net | 035 | 05 |
| I do not know | 039 | 05 |
| From dirt | 053 | 07 |
| Mosquito bites | 571 | 80 |
| Perceive causes of malaria | ||
| Playing in rain | 003 | 00 |
| Eating sour things | 006 | 01 |
| Do not know | 010 | 01 |
| Cold weather | 019 | 03 |
| Cold food | 028 | 04 |
| Mosquito | 683 | 91 |
| Malaria consequences during pregnancy | ||
| Give birth to a low weight baby | 016 | 02 |
| Causes death | 018 | 03 |
| Foetal death | 019 | 03 |
| Premature delivery | 026 | 04 |
| Transmitted across placenta to the foetus | 030 | 04 |
| Causes anaemia | 235 | 34 |
| Causes abortion | 348 | 50 |
| Groups at risk of Malaria | ||
| People living with HIV/AIDS | 012 | 02 |
| Do not know | 086 | 12 |
| Children under 5 Years | 287 | 40 |
| Pregnant women | 331 | 46 |
Abortion was cited by 50% of the respondents as a consequence of malaria during pregnancy followed by jaundice at 34%. Giving birth to a low weight baby was the least mentioned by 16 (2%). When asked about groups at risk of malaria, 331 (46%) indicated that pregnant women were at risk for malaria while 287 (40%) said it was children less than five years and 86 (12%) of the pregnant women could not mention any group at risk of malaria. Table 3 summarises malaria knowledge among pregnant women.
The age of respondent was found not to be correlated with malaria knowledge and was not significantly associated with malaria knowledge. However, education level had a weak positively correlated with knowledge of perceive cause of malaria (ϱ = 0.129, P value = 0.0004) and was found to be significantly associated with the knowledge of the perceived cause of malaria (Table 4).
Table 4.
Respondent's knowledge of malaria cause by educations level (n).
| Variable | Education level | |||
|---|---|---|---|---|
| causes of malaria | Not educated | Primary | Secondary | Tertiary |
| Playing in rain | 002 | 001 | 000 | 000 |
| Eating sour things | 002 | 004 | 000 | 000 |
| Do not know | 007 | 003 | 000 | 000 |
| Cold weather | 006 | 012 | 001 | 000 |
| Cold food | 013 | 013 | 002 | 000 |
| Mosquito | 157 | 501 | 023 | 002 |
| Total number (n) | 187 | 534 | 026 | 002 |
Chi-Square (χ2) = 25.12.
P value = 0.011.
4. Discussion
Our study shows that in the post conflict IDP camps of Gulu district, pregnant women have not demonstrated a better understanding of the cause of malaria as observed by other studies done elsewhere [15–17]. Majority of respondents reported to have ever heard about malaria with the main source of information being from health centres followed by radio. However, those who indicated that they heard from within the community were the least while 3% of the pregnant women could not recall the source. However, a great percentage of the pregnant women indicated that they had not heard about malaria. In contrast, a study done in Tanzania shows that almost all the respondents have never heard about malaria [18].
Also, a high percentage of the respondents were knowledgeable about mosquitoes as a cause of malaria/fever. Indeed, in the local dialect the word two lyeto means fever caused by mosquitoes. This is a misconception about the cause of malaria because mosquito is a vector. This misconception was mentioned by majority across educational status and was found to be weakly correlated with educational level. However, when a chi-square test was performed, it was found to be statistically significant. Other study done in Ethiopia indicates that educational status was not significantly associated with basic awareness about the cause of malaria [19]. While mosquito was implicated as a cause of malaria, the aetiologic agent of malaria was not mentioned as people usually incriminate mosquitoes as the causative agents of malaria [20–22]. Other causes of malaria mentioned by pregnant women were cold food, playing in rain, cold weather, and eating mango. A study done in Kampala by Njama et al. indicated that 90% of the caregivers knew that mosquitoes cause malaria although they equally indicated other perceived causes such as drinking unboiled water and respiratory illnesses [23]. Another study done in Uganda shows that malaria is believed to be caused by poor diet and exposure to bad environmental conditions [24]. While in Ghana, it has been reported that malaria is presumed to be caused as a result of excessive heat and eating oily or starchy food [25, 26]. In Guatemala, malaria is thought to be caused by exposure to cold or wet conditions, weakness or poor general health, poor eating habits, and problems related to hygiene [27]. Also, a study from coastal Kenya found that most mothers did not know the association between mosquitoes and malaria [28]. Misconceptions about malaria still exist among pregnant women in this study. Therefore, there is need for awareness creation among pregnant women to know that mosquito is a vector for malaria parasite that causes malaria so that all these misconceptions are addressed. People's perceptions and understandings about the perceived cause and transmission of malaria have strong implications on the preventive measures such as the current scale-up ITNs implementation [24, 25]. Therefore, public health education interventions should always be designed to cover the existing knowledge and should be implemented for a sufficient length of time for it to be effective [29].
Majority of the pregnant women knew that mosquito bite was the mode of malaria transmission. This demonstrated high level of knowledge on malaria transmission compared with findings from other malaria endemic countries [30, 31]. However, this study also revealed evidence of knowledge gaps about malaria transmission by some pregnant women who reported that malaria is transmitted through cold weather, from dirt, when you do not sleep under net and others had no clue on the mode of malaria transmission. It is evident therefore that misconception about malaria transmission still exist in endemic country like Uganda as shown by the results of this study. Results from other studies done in Africa have shown that malaria is misconceived to be transmitted through drinking contaminated/unboiled water, staying in the sun and working in rain [12, 32, 33].
This study has demonstrated that pregnant women had a good knowledge about malaria signs and symptoms. The most commonly mentioned symptom was feeling cold, followed by fever, headache, vomiting, and jaundice. This high level of awareness of the clinical features of malaria might be due to increased access to mass media, health education by health workers, and the village health team in the community. Other studies done elsewhere also shows similar results that participants had good knowledge on malaria signs and symptoms [30, 32].
A half of the respondent cited abortion as the consequences of malaria infection during pregnancy. Other consequences of malaria infection during pregnancy mentioned by respondents were anaemia, transmission across to the foetus, premature delivery of babies, foetal death, death of the pregnant woman, and giving birth to a low weight baby. Other study done in Nigeria indicates that knowledge of the consequences of malaria during pregnancy was poor among pregnant women [34]. This study has shown that pregnant women knew at least one of the consequences of malaria infection during pregnancy. This knowledge is good for setting up appropriate malaria prevention strategy among pregnant women since they are aware of malaria danger during pregnancy. Other study has indicated that the increased risk posed to pregnant women by malaria was almost universally recognized, but the knowledge of the health impact of malaria to the health of the foetus was very low [35].
Also, most of the pregnant women had knowledge of group of people who are perceived to be at risk for malaria. Among these groups mentioned were pregnant women, children under five years, and people living with HIV/AIDS. However, some of the respondent could not tell people who were at risk for malaria. The lack of knowledge by majority of pregnant women that they were at increase risk for malaria calls for more sensitisation in the community so that awareness is increased among pregnant women about malaria infection during pregnancy.
5. Conclusion and Recommendation
This study indicates that pregnant women in the post conflict IDP camps in Gulu district were aware about malaria transmission, signs, symptoms, and consequences of malaria during pregnancy. However, misconception about the cause of malaria still exists and thus, there is need for more public health education about the cause of malaria among pregnant women to minimise misconceptions about the cause of malaria. Also, there is need for more awareness creation so that malaria signs and symptoms are well understood by pregnant women to promote early treatment for malaria as well as preventive and control efforts in the community.
Conflict of Interests
The authors declare that they have no competing interests.
Authors' Contribution
J. Henry participated in the conception, design and implementation of the study, statistical analysis, interpretation, and drafting of the paper. D. L. Kitara participated in study design, interpretation, and drafting of the paper. C. G. Orach participated in study conception, design, statistical analysis, interpretation, and drafting of the paper. All authors read and approved the final paper.
Acknowledgments
The authors would like to express their gratitude to the Belgian Technical Cooperation in Uganda for the scholarship given to the author. We specially thank the pregnant women for accepting to participate in this study. Special thanks go to Makerere University, Faculty of Medicine Research and Ethics Committee for the ethical clearance and Gulu District Local Government for giving permission to conduct the study.
References
- 1.Bassey BE, Asor JE, Useh MF. Profile of malaria in pregnant women attending antenatal clinics in rural community in Nigeria. The Open Parasitology Journal. 2007;1:1–6. [Google Scholar]
- 2.Adefioye OA, Adeyeba OA, Hassan WO, Oyeniran OA. Prevalence of malaria parasite infection among pregnant women in Osogbo, Southwest, Nigeria. American-Eurasian Journal of Scientific Research. 2007;2(1):43–45. [Google Scholar]
- 3.Kimani EW, Vulule JM, Kuria IW, Mugisha F. Use of insecticide-treated clothes for personal protection against malaria: a community trial. Malaria Journal. 2006;5, article 63 doi: 10.1186/1475-2875-5-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.WHO. Tech. Rep. AFR/MAL/04/01. Geneva, Switzerland: World Health Organization; 2004. A strategic framework for malaria prevention and control during pregnancy in the Africa Region. [Google Scholar]
- 5.Annual Health Sector Performance Report. Republic of Uganda: Ministry of Health; 2008. [Google Scholar]
- 6.Mbonye AK, Neema S, Magnussen P. Treatment-seeking practices for malaria in pregnancy among rural women in Mukono District, Uganda. Journal of Biosocial Science. 2006;38(2):221–237. doi: 10.1017/S0021932005007108. [DOI] [PubMed] [Google Scholar]
- 7.Schultz LJ, Steketee RW, Chitsulo L, Macheso A, Nyasulu Y, Ettling M. Malaria and childbearing women in Malawi: knowledge, attitudes and practices. Tropical Medicine and Parasitology. 1994;45(1):65–69. [PubMed] [Google Scholar]
- 8.Mubyazi G, Bloch P, Kamugisha M, Kitua A, Ijumba J. Intermittent preventive treatment of malaria during pregnancy: a qualitative study of knowledge, attitudes and practices of district health managers, antenatal care staff and pregnant women in Korogwe District, north-eastern Tanzania. Malaria Journal. 2005;4, article 31 doi: 10.1186/1475-2875-4-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mbonye AK, Neema S, Magnussen P. Preventing malaria in pregnancy: a study of perceptions and policy implications in Mukono district, Uganda. Health Policy and Planning. 2006;21(1):17–26. doi: 10.1093/heapol/czj002. [DOI] [PubMed] [Google Scholar]
- 10.Belay M, Deressa W. Use of insecticide treated nets by pregnant women and associated factors in a pre-dominantly rural population in northern Ethiopia. Tropical Medicine and International Health. 2008;13(10):1303–1313. doi: 10.1111/j.1365-3156.2008.02159.x. [DOI] [PubMed] [Google Scholar]
- 11.Hla-Shein T, Soe-Soe T, Ne-Win K. The level of knowledge, attitude and practice in relation to malaria in Oo-do village, Myanmar. Southeast Asian Journal of Tropical Medicine and Public Health. 1998;29(3):546–549. [PubMed] [Google Scholar]
- 12.Vundule C, Mharakurwa S. Knowledge, practices, and perceptions about malaria in rural communities of Zimbabwe: relevance to malaria control. Bulletin of the World Health Organization. 1996;74(1):55–60. [PMC free article] [PubMed] [Google Scholar]
- 13. United Nation High Commissioner for Refugee unpublished data from Gulu office, 2008.
- 14. Gulu District Health Directorate Work plan, unpublished data from Gulu district health officer record, 2009.
- 15.Ahmed SM, Haque R, Haque U, Hossain A. Knowledge on the transmission, prevention and treatment of malaria among two endemic populations of Bangladesh and their health-seeking behaviour. Malaria Journal. 2009;8(1, article 173) doi: 10.1186/1475-2875-8-173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mboera LEG, Mlozi MRS, Senkoro KP, et al. Malaria and Agriculture in Tanzania. Impact of Land Use and Agricultural Practices on Malaria in Mvomero District. Dar es Salaam, Tanzania: National Institute for Medical Research; 2007. [Google Scholar]
- 17.Hlongwana KW, Mabaso MLH, Kunene S, Govender D, Maharaj R. Community knowledge, attitudes and practices (KAP) on malaria in Swaziland: a country earmarked for malaria elimination. Malaria Journal. 2009;8(1, article 29) doi: 10.1186/1475-2875-8-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mazigo HD, Obasy E, Mauka W, et al. Knowledge, attitudes, and practices about malaria and its control in rural northwest Tanzania. Malaria Research and Treatment. 2010;2010:9 pages. doi: 10.4061/2010/794261. Article ID 794261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Legesse M, Deressa W. Community awareness about malaria, its treatment and mosquito vector in rural highlands of central Ethiopia. Ethiopian Journal of Health Development. 2009;23(1):40–47. [Google Scholar]
- 20.Govere J, Durrheim D, La Grange K, Mabuza A, Booman M. Community knowledge and perceptions about malaria and practices influencing malaria control in Mpumalanga Province, South Africa. South African Medical Journal. 2000;90(6):611–616. [PubMed] [Google Scholar]
- 21.Okrah J, Traoré C, Palé A, Sommerfeld J, Müller O. Community factors associated with malaria prevention by mosquito nets: an exploratory study in rural Burkina Faso. Tropical Medicine and International Health. 2002;7(3):240–248. doi: 10.1046/j.1365-3156.2002.00856.x. [DOI] [PubMed] [Google Scholar]
- 22.Karanja DMS, Alaii J, Abok K, et al. Knowledge and attitudes to malaria control and acceptability of permethrin impregnated sisal curtains. East African Medical Journal. 1999;76(1):42–46. [PubMed] [Google Scholar]
- 23.Njama D, Dorsey G, Guwatudde D, et al. Urban malaria: primary caregivers’ knowledge, attitudes, practices and predictors of malaria incidence in a cohort of Ugandan children. Tropical Medicine and International Health. 2003;8(8):685–692. doi: 10.1046/j.1365-3156.2003.01060.x. [DOI] [PubMed] [Google Scholar]
- 24.Nuwaha F. People’s perception of malaria in Mbarara, Uganda. Tropical Medicine and International Health. 2002;7(5):462–470. doi: 10.1046/j.1365-3156.2002.00877.x. [DOI] [PubMed] [Google Scholar]
- 25.Ahorlu CK, Dunyo SK, Afari EA, Koram KA, Nkrumah FK. Malaria-related beliefs and behaviour in southern Ghana: implications for treatment, prevention and control. Tropical Medicine and International Health. 1997;2(5):488–499. [PubMed] [Google Scholar]
- 26.Agyepong IA, Manderson L. The diagnosis and management of fever at household level in the Greater Accra Region, Ghana. Acta Tropica. 1994;58(3-4):317–330. doi: 10.1016/0001-706x(94)90025-6. [DOI] [PubMed] [Google Scholar]
- 27.Klein RE, Weller SC, Zeissig R, Richards FO, Ruebush TK., II Knowledge, beliefs, and practices in relation to malaria transmission and vector control in Guatemala. American Journal of Tropical Medicine and Hygiene. 1995;52(5):383–388. doi: 10.4269/ajtmh.1995.52.383. [DOI] [PubMed] [Google Scholar]
- 28.Mwenesi H, Harpham T, Snow RW. Child malaria treatment practices among mothers in Kenya. Social Science and Medicine. 1995;40(9):1271–1277. doi: 10.1016/0277-9536(94)00250-w. [DOI] [PubMed] [Google Scholar]
- 29.Kroeger A, Meyer R, Mancheno M, Gonzalez M. Health education for community-based malaria control: an intervention study in Ecuador, Colombia and Nicaragua. Tropical Medicine and International Health. 1996;1(6):836–846. doi: 10.1111/j.1365-3156.1996.tb00119.x. [DOI] [PubMed] [Google Scholar]
- 30.Habtai H, Ghebremeskel T, Mihreteab S, Mufunda J, Ghebremichael A. Knowledge, attitudes and practices (KAP) about malaria among people visiting referral hospitals of Eritrea in 2008. Journal of Eritrean Medical Association. 2009;4(1):42–46. [Google Scholar]
- 31.Opiyo P, Mukabana WR, Kiche I, Mathenge E, Killeen GF, Fillinger U. An exploratory study of community factors relevant for participatory malaria control on Rusinga Island, western Kenya. Malaria Journal. 2007;6, article 48 doi: 10.1186/1475-2875-6-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kinung’Hi SM, Mashauri F, Mwanga JR, et al. Knowledge, attitudes and practices about malaria among communities: comparing epidemic and non-epidemic prone communities of Muleba district, North-western Tanzania. BMC Public Health. 2010;10, article 395 doi: 10.1186/1471-2458-10-395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Idowu OA, Mafiana CF, Luwoye IJ, Adehanloye O. Perceptions and home management practices of malaria in some rural communities in Abeokuta, Nigeria. Travel Medicine and Infectious Disease. 2008;6(4):210–214. doi: 10.1016/j.tmaid.2007.10.007. [DOI] [PubMed] [Google Scholar]
- 34.Enato EFO, Okhamafe AO, Okpere EE. A survey of knowledge, attitude and practice of malaria management among pregnant women from two health care facilities in Nigeria. Acta Obstetricia et Gynecologica Scandinavica. 2007;86(1):33–36. doi: 10.1080/00016340600984670. [DOI] [PubMed] [Google Scholar]
- 35.Nganda RY, Drakeley C, Reyburn H, Marchant T. Knowledge of malaria influences the use of insecticide treated nets but not intermittent presumptive treatment by pregnant women in Tanzania. Malaria Journal. 2004;3, article 42 doi: 10.1186/1475-2875-3-42. [DOI] [PMC free article] [PubMed] [Google Scholar]