

Abstract
Introduction
It is well known that obesity is a risk factor for sleep-disordered breathing (SDB). However, whether SDB predicts increase in BMI is not well defined. Data from the Sleep Heart Health Study (SHHS) were analyzed to determine whether SDB predicts longitudinal increase in BMI, adjusted for confounding factors.
Methods
A full-montage unattended home polysomnogram (PSG) and body anthropometric measurements were obtained approximately five years apart in 3001 participants. Apnea-hypopnea index (AHI) was categorized using clinical thresholds: < 5 (normal), ≥ 5 to <15 (mild sleep apnea), and ≥ 15 (moderate to severe sleep apnea). Linear regression was used to examine the association between the three AHI groups and increased BMI. The model included age, gender, race, baseline BMI, and change in AHI as covariates.
Results
Mean (SD) age was 62.2 years (10.14), 55.2% were female and 76.1% were Caucasian. Five-year increase in BMI was modest with a mean (SD) change of 0.53 (2.62) kg/m2 (p=0.071). A multivariate regression model showed that subjects with a baseline AHI between 5–15 had a mean increase in BMI of 0.22 kg/m2 (p=0.055) and those with baseline AHI ≥ 15 had a BMI increase of 0.51 kg/m2 (p<0.001) compared to those with baseline AHI of <5.
Conclusion
Our findings suggest that there is a positive association between severity of SDB and subsequent increased BMI over approximately 5 years. This observation may help explain why persons with SDB have difficulty losing weight.
Keywords: Sleep Apnea, Weight Gain, Obesity
Introduction
There is overwhelming epidemiological and clinical data indicating that obesity is a risk factor for sleep disordered breathing (SDB).1–8 The association between obesity and SDB is substantial, with high body mass index (BMI) contributing to moderate to severe SDB in 58% of affected persons.9 The effect of obesity is greater in men than women1,10–12 although it decreases with increasing age.6,7 In addition, weight loss has been demonstrated to decrease the severity of SDB.10,13,14 Longitudinal data from population studies including the Sleep Heart Health Study (SHHS),10 the Wisconsin Sleep Cohort,15 and the Cleveland Family Study6 have initially focused on the impact of increased weight on SDB severity. However, examination of the opposite causal pathway has yet to be prospectively addressed.
Anecdotally, patients with SDB appear to have more difficulty losing weight than obese patients without SDB. They also report marked weight gain prior to confirmation of their diagnosis. Two small studies support these empiric observations.5,16 Given this limited information on the impact of SDB on BMI, data from SHHS was analyzed to examine the impact of SDB on BMI after controlling for change in AHI and severity of SDB.
Methods
Study Design and Population
The SHHS is a multi-center, community-based prospective cohort study of the natural history and cardiovascular consequences of SDB. Details of the study design, sampling, and procedures have been reported.17 Briefly, between November 1995 and January 1998 participants were recruited from several ongoing prospective cohort studies--the Framingham Offspring and Omni Studies, the Atherosclerosis Risk in Communities Study, the Cardiovascular Health Study, the Strong Heart Study, and the cohort studies of respiratory disease in Tucson and of hypertension in New York. Participants were eligible if they were ≥ 40 years of age and were not being treated for sleep apnea with positive pressure therapy, an oral appliance, oxygen, or a tracheostomy. Habitual snorers < 65 years were over sampled to increase the prevalence of obstructive sleep apnea. Subjects were required to provide written consent and the protocol was approved by the institutional review boards of each of the eight investigative sites.
Data Collection
A total of 6,441 subjects completed the baseline polysomnogram (PSG), and 4,586 consented to have a second evaluation approximately five years later. This analysis focuses on the 3,040 participants who had PSG and BMI data at both time points. Data from all 215 participants who had a follow-up PSG from the New York center were excluded because they did not meet quality standards for the follow-up examination. The remaining participants died, were too ill to participate, refused to participate, were lost to follow-up or had incomplete covariate data such as weight. This latter group had a higher percentage of Whites (85%) compared with the study group (75.5%) (p-value <0.001). There also were statistically significant differences in baseline BMI, baseline AHI, and age between the study group compared with the excluded group, however, these differences were very small and were not clinically significant. There was no gender difference between the two groups.
Weight was measured on the night of the PSG examination with the participant in light clothes on a calibrated portable scale. Height was obtained at the baseline home visit if not already measured within ± 3 months of the parent study. BMI was calculated as weight in kilograms divided by the square of height in meters. Baseline height was used for baseline and follow-up BMI calculations. Age, sex, and ethnicity were self-reported.
The PSG was conducted using a portable monitor (PS-2 System; Compumedics Limited, Abbotsford, Victoria, Australia), using methods previously described.18 Apnea was present if there was an absence or near absence of airflow or thoracoabdominal movement (at least < 25% of baseline) for > 10 seconds. Hypopnea was defined as a decrease in the amplitude of the airflow or thoracoabdominal movement below 70% of baseline for > 10 seconds. The apnea-hypopnea index (AHI) was calculated as the number of apnea and hypopnea events, each associated with at least a 4% decrease in oxygen saturation, divided by total sleep time in hours.
Statistical Analyses
The primary endpoint in this analysis was change in BMI determined as BMI at follow-up minus the baseline value. AHI was categorized using clinical cutoffs: < 5 (normal), ≥ 5 to <15 (mild sleep apnea), and ≤ 15 (moderate to severe sleep apnea). Delta AHI was computed as the difference between follow-up AHI and baseline AHI. Race was categorized into “White” and “Other” because of the small number of non-White participants. Chi square tests were used to assess differences in proportions and analysis of variance (ANOVA) was employed to assess differences in means. A linear regression model was used to examine the association between AHI category at follow-up and change in BMI. The model was adjusted for age, gender, race, baseline BMI, and change in AHI. An interaction term of gender by AHI group was also tested and not found to be statistically significant and thus removed from the final model. A p-value of <0.05 was used for all analyses to determine statistical significance. All analyses were conducted using SPSS 15.0 (SPSS Inc, Chicago, IL).
Results
Participant characteristics are provided in Table 1.
Table 1.
Characteristics of participants of the Sleep Heart Health Study cohort with complete baseline and follow-up polysomnography and weight measurements as a function of sleep apnea severity.
| BASELINE AHI | |||||
|---|---|---|---|---|---|
|
|
|||||
| All Subjects N = 3040 | AHI < 5 events/hr N = 1657 | AHI ≥ 5 to <15 events/hr N = 893 | AHI: ≥ 15 events/hr N = 490 | p-value* | |
|
| |||||
| Sex, % | |||||
| Women | 55.13% | 64.94% | 47.14% | 36.53% | <0.001 |
| Men | 44.87% | 35.06% | 52.86% | 63.47% | |
|
| |||||
| Race, % | |||||
| White | 75.53% | 76.64% | 74.36% | 73.88% | 0.286 |
| Other | 24.47% | 23.36% | 25.64% | 26.12% | |
|
| |||||
| Baseline Age, mean (SD) | 62.05 (10.18) | 60.71 (10.36) | 63.53 (9.87) | 63.89 (9.45) | <0.001 |
|
| |||||
| Baseline BMI kg/m2, mean (SD) | 28.74 (5.27) | 27.23 (4.51) | 29.90 (5.24) | 31.73 (5.86) | <0.001 |
|
| |||||
| Follow-up BMI kg/m2 | 29.27 (5.51) | 27.86 (4.84) | 30.33 (5.41) | 32.10 (6.25) | <0.001 |
|
| |||||
| BMI kg/m2 change, mean (SD) | 0.53 (2.61) | 0.63 (2.54) | 0.43 (2.48) | 0.37 (3.05) | 0.064 |
|
| |||||
| AHI change, mean (SD) | 2.68 (10.58) | 3.28 (6.48) | 3.82 (10.94) | −1.40 (17.76) | <0.001 |
p-value for chi-square for sex and race, and One Way Analysis of Variance for baseline age, baseline BMI, follow-up BMI, change of BMI, and change of AHI.
As expected, women were over-represented in the baseline AHI < 5 group (64.9%) and men were over-represented in the AHI ≥ 15 group (63.5%) (p<0.001). Baseline BMI increased as baseline AHI severity increased. Overall unadjusted five-year increase in BMI was modest with a mean (SD) BMI change of 0.53 (2.61) kg/m2. The unadjusted five-year increase in BMI was 0.63 (2.54) kg/m2 for those with baseline AHI < 5, 0.43 (2.48) kg/m2 among those with AHI ≥ 5 to < 15 and 0.37 (3.05) kg/m2 for the AHI group ≥ 15. These values were not statistically different from each other.
A multivariate regression model was constructed predicting five-year change in BMI by baseline AHI category adjusted for age, gender, race, baseline BMI, and AHI change (Table 2).
Table 2.
Adjusted β coefficients of BMI change according to AHI and continuous variables in the Sleep Heart Health Study*.
| β Coefficient | 95% CI | P-value | |
|---|---|---|---|
| AHI ≥ 15.0 | 0.508 | 0.226 – 0.790 | <0.001 |
| AHI < 5.0 – 14.9 | 0.213 | (−0.004) – 0.430 | 0.055 |
| Baseline Age | −0.050 | (−0.059) – (−0.041) | <0.001 |
| Baseline BMI | −0.094 | (−0.112) – (−0.075) | <0.001 |
| AHI change | 0.027 | 0.019 – 0.036 | <0.001 |
| Sex (female) | 0.183 | (−0.004) – 0.370 | 0.055 |
| Race (other) | −0.161 | (−0.377) – 0.0543 | 0.142 |
White is the reference category for race, Male is the reference category for sex, AHI < 5 is the reference category for AHI group.
Compared to baseline AHI group of < 5, those with AHI between ≥ 5 to < 15 had a mean adjusted increase in BMI of 0.21 that approached statistical significance (p=0.055). However, those with AHI ≥ 15 had a statistically significant adjusted BMI increase of 0.51 (p<0.001). Younger age, lower baseline BMI and greater AHI change also were associated with a larger BMI increase. There was a trend for women to have a greater increase in BMI, but no effect of race was observed. However, the model only accounted for 7% of the total variance. Adjusted means by baseline AHI group are displayed graphically in Figure 1.
Figure 1.
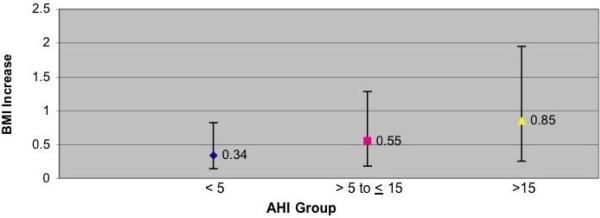
Estimated Adjusted Means of BMI increase according to AHI in the Sleep Heart Health Study. Data are adjusted for baseline age (continuous), race (categorical), gender (categorical), baseline BMI (continuous), change in AHI (continuous). Covariates fixed at: baseline BMI = 28.7, baseline age 62.1, change in RDI = 2.7. Bars represent 95% confidence intervals.
Discussion
Our findings indicate that there is a positive association between severity of SDB and five-year increase in BMI. The finding was demonstrated after controlling for key covariates including age, gender, race, baseline BMI, and AHI change. This observation may help explain the difficulty patients with SDB have in trying to lose weight. Two previous small studies have demonstrated a positive association between newly diagnosed SDB and weight gain. A retrospective study by Phillips et al. compared one-year weight histories of 53 men and women patients who were recently diagnosed with SDB with 24 control subjects matched for gender, age, BMI and percent body fat.5 Subjects in that study were somewhat younger than the SHHS cohort with an age difference of approximately 10 years. The SDB among subjects in the previous study tended to be moderate to severe with mean ± SEM AHI 33 ± 5 /h for men and 37 ± 10 /h for women. Mean ± SEM of BMI at time of diagnosis was somewhat higher than in the SHHS with 35 ± 1 kg/m2 for men and 44 ± 2 kg/m2 for women. Men and women patients with SDB had reported a recent weight gain of 7.4 ± 1.5 kg compared with a weight loss of 0.5 ± 1.7 kg (p=0.001) in obese controls without SDB. However, given the design of this study it is not possible to determine whether weight gain contributed to the onset of SDB or was a result of SDB. The study was also limited by reliance on self-report of weight gain history.
Another study by Traviss et al. prospectively evaluated 49 obese patients with newly diagnosed SDB.16 Mean ± SD of AHI at diagnosis was severe at 45 ± 27 /h. BMI at diagnosis was elevated at 36.5 ± 6.2 kg/m2. Of the 49 subjects, 43 could estimate the duration of their symptoms with 84% reporting weight gain since becoming symptomatic. Weight gain was relatively large, with a reported 17 ± 15 kg over 5.3 ± 4.8 years. However, this study was limited by the lack of a control group and reliance on self-report of weight history. These two small studies, in addition to our findings, suggest that there is an association between SDB and increased BMI.
Interestingly, unadjusted BMI change in our study was quite modest and not statistically different as a function of SDB severity. However, BMI change over time is a complex phenomenon influenced by several variables. A large (29,799 subjects) prospective study examining 5-year change in weight in a multi-ethnic cohort of men and women explored several of these relationships.19 In that study, younger men and to a greater degree, younger women were at greater risk for weight gain compared to older adults. This is consistent with our initial findings. In addition, there was a trend for women in the higher baseline BMI categories of `overweight' (BMI >25– 30 kg/m2) and `obese' (BMI >30 kg/m2) in the aforementioned cohort to gain more weight than men in the higher baseline BMI categories. In order to more precisely examine the effect of AHI on weight change, we controlled for these confounders in our final multivariate model thus resulting in the finding of an increase in BMI as a function of SDB severity in this study.
Several mechanisms could explain why SDB contributes to increased BMI. First, persons with SDB may have a reduction in the quantity and quality of their sleep. Recent data indicate that insufficient sleep may be a risk factor for obesity.20 Experimental sleep restriction increases ghrelin and reduces leptin production favoring appetite enhancement,21 a finding that also has been observed in a large population cohort.22 Second, those with SDB may eat a diet that favors weight gain. In support of this hypothesis, sleep restriction has been shown to increase craving for calorie dense food with high carbohydrate content. The Apnea Positive Pressure Long-Term Efficacy Study (APPLES) demonstrated that those with severe SDB consumed a diet higher in cholesterol, protein, total fat and total saturated fatty acids, even after adjusting for BMI, age, and daytime sleepiness.23 Third, a cardinal symptom of SDB is excessive daytime sleepiness. Thus, it is possible that persons with SDB engage in less physical activity because they are too fatigued to exercise. Data from APPLES indicate that recreational physical activity is less in those with SDB. However, this finding appears to be principally explained by concomitant obesity.
Weight loss frequently results in an improvement and sometimes resolution in SDB. This is most evident in those who undergo bariatric surgical procedures.24,25 Persons with SDB are frequently counseled to treat their SDB by losing weight through diet and exercise,26 an approach that is usually unsuccessful.25 Failure to primarily address SDB in conjunction with a weight reduction program may diminish the latter's success. However, evidence to date indicates that treatment of SDB does not consistently result in weight loss. In a sample of clinical patients with SDB, treatment with CPAP did not result in weight loss. Moreover, in female patients, there was actually an increase in weight.27 In addition, consistent weight reduction was not observed in a small number of patients with severe OSA who underwent tracheostomy.28 Thus, it appears that weight gain engendered by the presence of OSA is not easily reversed despite therapy. Prospective studies will be required to determine whether primary treatment for OSA enhances weight loss programs in those with OSA.
Although this analysis demonstrated a positive association of severity of SDB on five-year increase in BMI, there are several caveats that deserve consideration. The BMI of participants tended to be lower than that seen in clinical SDB populations and a relatively small number of subjects had large changes in BMI. As previously noted, the mean BMI increase was, at best, quite modest. When converted for illustrative purposes to weight using an average height of 167 cm of the participants, those with an AHI between ≥ 5 to < 15 had a mean adjusted increase in BMI of 0.21 kg/m2 equal to 0.59 kg or 1.30 lbs. Similarly, those with AHI ≥ 15 had an adjusted BMI increase of 0.51 kg/m2 equal to 1.42 kg or 3.13 lbs. Thus, the magnitude of the changes we observed may not be applicable to clinical populations where patients with SDB may have a higher BMI. In addition, it is not known when the participants developed SDB, thus definitive inference of causality cannot be made. However, following a large undiagnosed cohort over an extended period of time to determine incidence of SDB onset and subsequent change in weight would be exceedingly difficult and costly. Additionally, the model only accounted for a small amount of the total variance in five-year BMI increase, suggesting that there are likely other unmeasured variables influencing the amount of BMI increase over time in this cohort. Finally, while not statistically significant, the unadjusted mean change in BMI was slightly less in the high RDI group in comparison to the lower RDI groups. This observation underscores the biological complexity of the interactions among weight change, SDB, age, gender and other factors.
In conclusion, our findings suggest that although weight gain is a risk factor for developing or worsening SDB, SDB may, in a reciprocal fashion, lead to increased weight gain. This may help explain why patients with SDB find it difficult to lose weight.
Acknowledgements
This work was supported by National Heart, Lung and Blood Institute cooperative agreements U01HL53940 (University of Washington), U01HL53941 (Boston University), U01HL53938 (University of Arizona), U01HL53916 (University of California, Davis), U01HL53934 (University of Minnesota), U01HL53931 (New York University), U01HL53937 and U01HL64360 (Johns Hopkins University), U01HL63463 (Case Western Reserve University), and U01HL63429 (Missouri Breaks Research).
Sleep Heart Health Study (SHHS) acknowledges the Atherosclerosis Risk in Communities Study (ARIC), the Cardiovascular Health Study (CHS), the Framingham Heart Study (FHS), the Cornell/Mt. Sinai Worksite and Hypertension Studies, the Strong Heart Study (SHS), the Tucson Epidemiologic Study of Airways Obstructive Diseases (TES) and the Tucson Health and Environment Study (H&E) for allowing their cohort members to be part of the SHHS and for permitting data acquired by them to be used in the study. SHHS is particularly grateful to the members of these cohorts who agreed to participate in SHHS as well. SHHS further recognizes all of the investigators and staff who have contributed to its success. A list of SHHS investigators, staff and their participating institutions is available on the SHHS website, www.jhucct.com/shhs. The opinions expressed in the paper are those of the author(s) and do not necessarily reflect the views of the Indian Health Service.
Abbreviation List
- PSG
polysomnogram
- SDB
sleep disordered breathing
- AHI
apnea hypopnea index
- SHHS
Sleep Heart Health Study
- BMI
body mass index
- SD
standard deviation
- SEM
standard error of the mean
- ANOVA
analysis of variance
Footnotes
These data have been presented in part at the Annual Meeting of the Associated Professional Sleep Societies, June 11, 2009, Seattle, WA.
Conflict of Interest Statement: None of the authors have conflicts of interest pertinent to the subject matter of this manuscript.
References
- 1.Bixler EO, Vgontzas AN, Lin HM, Ten Have T, Rein J, Vela-Bueno A, et al. Prevalence of sleep-disordered breathing in women: Effects of gender. Am J Respir Crit Care Med. 2001;163:608–13. doi: 10.1164/ajrccm.163.3.9911064. [DOI] [PubMed] [Google Scholar]
- 2.Bixler EO, Vgontzas AN, Ten Have T, Tyson K, Kales A. Effects of age on sleep apnea in men: I. prevalence and severity. Am J Respir Crit Care Med. 1998;157:144–8. doi: 10.1164/ajrccm.157.1.9706079. [DOI] [PubMed] [Google Scholar]
- 3.Carmelli D, Swan GE, Bliwise DL. Relationship of 30-year changes in obesity to sleep-disordered breathing in the western collaborative group study. Obes Res. 2000;8:632–7. doi: 10.1038/oby.2000.81. [DOI] [PubMed] [Google Scholar]
- 4.Duran J, Esnaola S, Rubio R, Iztueta A. Obstructive sleep apnea-hypopnea and related clinical features in a population-based sample of subjects aged 30 to 70 yr. Am J Respir Crit Care Med. 2001;163:685–9. doi: 10.1164/ajrccm.163.3.2005065. [DOI] [PubMed] [Google Scholar]
- 5.Phillips BG, Hisel TM, Kato M, Pesek CA, Dyken ME, Narkiewicz K, et al. Recent weight gain in patients with newly diagnosed obstructive sleep apnea. J Hypertens. 1999;17:1297–300. doi: 10.1097/00004872-199917090-00009. [DOI] [PubMed] [Google Scholar]
- 6.Tishler PV, Larkin EK, Schluchter MD, Redline S. Incidence of sleep-disordered breathing in an urban adult population: The relative importance of risk factors in the development of sleep-disordered breathing. JAMA. 2003;289:2230–7. doi: 10.1001/jama.289.17.2230. [DOI] [PubMed] [Google Scholar]
- 7.Young T, Shahar E, Nieto FJ, Redline S, Newman AB, Gottlieb DJ, et al. Predictors of sleep-disordered breathing in community-dwelling adults: The sleep heart health study. Arch Intern Med. 2002;162:893–900. doi: 10.1001/archinte.162.8.893. [DOI] [PubMed] [Google Scholar]
- 8.Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5. doi: 10.1056/NEJM199304293281704. [DOI] [PubMed] [Google Scholar]
- 9.Young T, Peppard PE, Taheri S. Excess weight and sleep-disordered breathing. J Appl Physiol. 2005;99:1592–9. doi: 10.1152/japplphysiol.00587.2005. [DOI] [PubMed] [Google Scholar]
- 10.Newman AB, Foster G, Givelber R, Nieto FJ, Redline S, Young T. Progression and regression of sleep-disordered breathing with changes in weight: The sleep heart health study. Arch Intern Med. 2005;165:2408–13. doi: 10.1001/archinte.165.20.2408. [DOI] [PubMed] [Google Scholar]
- 11.Ip MS, Lam B, Tang LC, Lauder IJ, Ip TY, Lam WK. A community study of sleep-disordered breathing in middle-aged chinese women in hong kong: Prevalence and gender differences. Chest. 2004;125:127–34. doi: 10.1378/chest.125.1.127. [DOI] [PubMed] [Google Scholar]
- 12.Millman RP, Carlisle CC, McGarvey ST, Eveloff SE, Levinson PD. Body fat distribution and sleep apnea severity in women. Chest. 1995;107:362–6. doi: 10.1378/chest.107.2.362. [DOI] [PubMed] [Google Scholar]
- 13.Barvaux VA, Aubert G, Rodenstein DO. Weight loss as a treatment for obstructive sleep apnoea. Sleep Med Rev. 2000;4:435–52. doi: 10.1053/smrv.2000.0114. [DOI] [PubMed] [Google Scholar]
- 14.Grunstein RR, Stenlof K, Hedner JA, Peltonen M, Karason K, Sjostrom L. Two year reduction in sleep apnea symptoms and associated diabetes incidence after weight loss in severe obesity. Sleep. 2007;30:703–10. doi: 10.1093/sleep/30.6.703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Peppard PE, Young T, Palta M, Dempsey J, Skatrud J. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA. 2000;284:3015–21. doi: 10.1001/jama.284.23.3015. [DOI] [PubMed] [Google Scholar]
- 16.Traviss KA, Barr SI, Fleming JA, Ryan CF. Lifestyle-related weight gain in obese men with newly diagnosed obstructive sleep apnea. J Am Diet Assoc. 2002;102:703–6. doi: 10.1016/s0002-8223(02)90160-4. [DOI] [PubMed] [Google Scholar]
- 17.Quan SF, Howard BV, Iber C, Kiley JP, Nieto FJ, O'Connor GT, et al. The sleep heart health study: Design, rationale, and methods. Sleep. 1997;20:1077–85. [PubMed] [Google Scholar]
- 18.Redline S, Sanders MH, Lind BK, Quan SF, Iber C, Gottlieb DJ, et al. Methods for obtaining and analyzing unattended polysomnography data for a multicenter study. sleep heart health research group. Sleep. 1998;21:759–67. [PubMed] [Google Scholar]
- 19.Ball K, Crawford D, Ireland P, Hodge A. Patterns and demographic predictors of 5-year weight change in a multi-ethnic cohort of men and women in australia. Public Health Nutr. 2003;6:269–81. doi: 10.1079/PHN2002431. [DOI] [PubMed] [Google Scholar]
- 20.Chaput JP, Despres JP, Bouchard C, Tremblay A. The association between sleep duration and weight gain in adults: A 6-year prospective study from the Quebec Family Study. Sleep. 2008;31:517–23. doi: 10.1093/sleep/31.4.517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Spiegel K, Tasali E, Penev P, Van Cauter E. Brief communication: Sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann Intern Med. 2004;141:846–50. doi: 10.7326/0003-4819-141-11-200412070-00008. [DOI] [PubMed] [Google Scholar]
- 22.Taheri S, Lin L, Austin D, Young T, Mignot E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004;1:e62. doi: 10.1371/journal.pmed.0010062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Vasquez MM, Goodwin JL, Drescher AA, Smith TW, Quan SF. Associations of dietary intake and physical activity with sleep disordered breathing in the apnea positive pressure long-term efficacy study (APPLES) J Clin Sleep Med. 2008;4:411–8. [PMC free article] [PubMed] [Google Scholar]
- 24.Rasheid S, Banasiak M, Gallagher SF, Lipska A, Kaba S, Ventimiglia D, et al. Gastric bypass is an effective treatment for obstructive sleep apnea in patients with clinically significant obesity. Obes Surg. 2003;13:58–61. doi: 10.1381/096089203321136593. [DOI] [PubMed] [Google Scholar]
- 25.Fritscher LG, Canani S, Mottin CC, Fritscher CC, Berleze D, Chapman K, et al. Bariatric surgery in the treatment of obstructive sleep apnea in morbidly obese patients. Respiration. 2007;74:647–52. doi: 10.1159/000107736. [DOI] [PubMed] [Google Scholar]
- 26.Veasey SC, Guilleminault C, Strohl KP, Sanders MH, Ballard RD, Magalang UJ. Medical therapy for obstructive sleep apnea: A review by the medical therapy for obstructive sleep apnea task force of the standards of practice committee of the american academy of sleep medicine. Sleep. 2006;29:1036–44. doi: 10.1093/sleep/29.8.1036. [DOI] [PubMed] [Google Scholar]
- 27.Redenius R, Murphy C, O'Neill E, Al-Hamwi M, Zallek SN. Does CPAP lead to change in BMI? J Clin Sleep Med. 2008;4:205–9. [PMC free article] [PubMed] [Google Scholar]
- 28.Haapaniemi JJ, Laurikainen EA, Halme P, Antila J. Long-term results of tracheostomy for severe obstructive sleep apnea syndrome. ORL J Otorhinolaryngol Relat Spec. 2001;63:131–6. doi: 10.1159/000055728. [DOI] [PubMed] [Google Scholar]