

Abstract
INTRODUCTION
Skin metastases may impair the quality of life due to physical appearance, odour, and bleeding.
PRESENTATION OF CASE
A 70-year-old woman presented with two enlarging nodules (measuring 12 cm and 3 cm in diameter) consistent with metastatic breast cancer in the left subclavicular area. The larger tumour did not respond to initial cryosurgery. Therefore we added hyperthermia using a disposable body warmer. In addition, the cryosurgery technique was modified to freeze deeper tissue. The entire tumour was covered with dry cotton, to which liquid nitrogen was applied. Twenty weeks later, the tumour became nearly flat and the patient noted improved activity in her daily life.
DISCUSSION
Combination treatment with sufficient freezing is important for controlling the tumour, while hyperthermia may accelerate the antitumor effects of cryosurgery.
CONCLUTION
This treatment provides an alternative for unresectable breast cancer skin metastases resistant to chemotherapy and radiotherapy.
Keywords: Liquid nitrogen, Heating pad, Breast cancer
1. Introduction
Skin metastases from breast cancer are relatively common and sometimes impair quality of life. We report a patient whose breast cancer skin metastases were successfully attenuated using a combination of cryosurgery and hyperthermia. This method may be an option for unresectable breast cancer skin metastases resistant to chemotherapy and radiotherapy.
2. Presentation of case
A 70-year-old woman underwent mastectomy and axillary lymph node dissection for breast cancer. The histopathological findings were solid tubular carcinoma with metastases in two axillary lymph nodes. As adjuvant therapy, CEF (cyclophosphamide, 5-fluorouracil and epirubicin) with fadrozole was administered 4 times. Two years post-operatively, local metastases developed in the left subclavicular area. Chemotherapy (weekly paclitaxel, fadrozole and capecitabine) and radiotherapy (total 100 Gy) were attempted but the lesions continued to enlarge. On examination, two yellow, malodorous tumours were found in the left subclavicular area (Fig. 1A), measuring 12 cm and 3 cm in diameter, respectively. Reddish induration was noted in the peritumoral skin. Cryosurgery was commenced, with liquid nitrogen applied once per week for two months. A cotton swab soaked with liquid nitrogen was applied to the tumour until the surface was frozen. Cryosurgery was effective for the smaller tumour. The larger lesion continued to enlarge. A hyperthermia regimen was added after cryosurgery. A disposable body warmer was placed on the tumour immediately after cryosurgery allowing the lesion to be heated for 12 h. After 6 weeks, the surface of the tumour began to dissolve, yet volume reduction was not seen (Fig. 1B). In order to strengthen the freezing power of cryosurgery, the tumour was covered with dry cotton, to which liquid nitrogen was applied. It took about 5 min to freeze the entire tumour. The surface of the tumour became necrotic and it became possible to remove the necrotic tissue by forceps on a weekly basis. Only mild bleeding was seen with this procedure. Along with reduction of tumour size, the foul odour disappeared. Twenty weeks later, the tumour became nearly flat and the patient noted improved activity in her daily life (Fig. 1C).
Fig. 1.
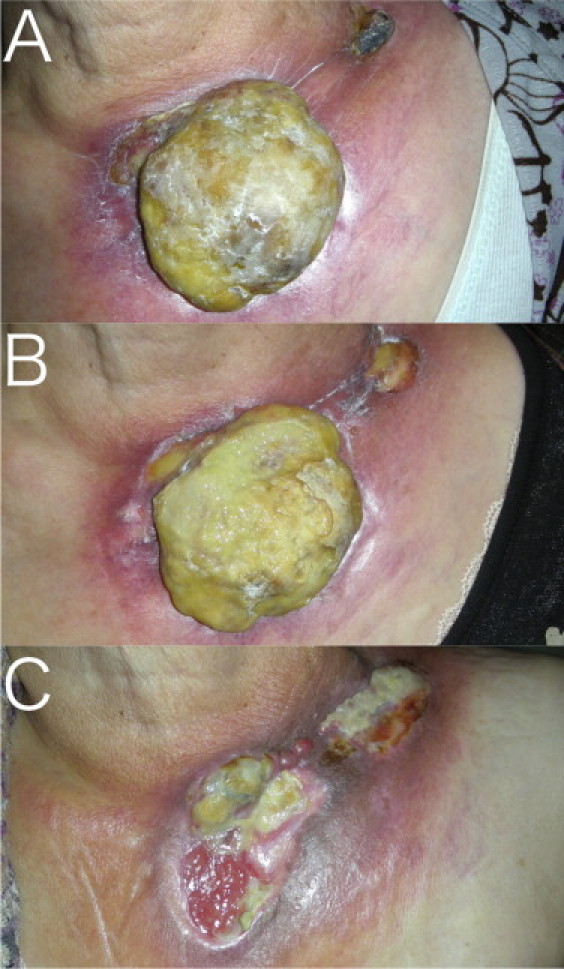
Skin metastasis from breast cancer was found on the left subclavicular area. (A) Before cryotherapy. The diameter of tumours was 12 cm and 3 cm, respectively. (B) Six weeks after cryotherapy and hyperthermic therapy with disposal-heating pad: the smaller tumour was nearly flat; the larger one was unchanged in size. (C) Twenty weeks later after improved cryotherapy and hyperthermic therapy: the tumour became flat.
3. Discussion
Breast cancer is the most common neoplasm to metastasize to the skin.1 Skin metastases impair activities of daily life due to physical appearance, odour and bleeding. In this case, we succeeded in controlling these symptoms through combined application of cryosurgery and hyperthermia, which resulted in a greatly improved quality of life. The biggest drawback to cryosurgery is pain. In this case, pain was initially mild when the tumour was large. As the tumour shrank, the pain increased, though it remained tolerable for the patient.
Cryosurgery is used to treat both benign and malignant lesions of the skin, inducing ice formation, extracellular osmolarity changes, and vasoconstriction that enhances cellular injury.2 Moreover, cryosurgery is thought to have immunological effects. In prior reports, combined cryo-heat therapy resulted in stimulation of a cytotoxic T-lymphocyte response, as well as attraction of immunocytes into tumour debris.3 In our case, freezing the tumour was a problem due to its size. At first, we simply applied a cotton swab soaked with liquid nitrogen but could freeze only the tumour surface. Therefore, we applied liquid nitrogen through the dry cotton that prolonged contact time and broadened the contact area. This method facilitated complete tumour freezing. In addition, hyperthermia is at times also used for cancer therapy, with the use of hyperthermia alone resulting in complete overall response rates of 13% in prior reports.4 A meta-analysis of five trials demonstrated the efficacy of hyperthermia as an adjunct to radiotherapy for treatment of recurrent breast cancer.5 We used a disposable body warmer in this case; this method might be the most practical way to induce hyperthermia in the clinical setting. This treatment might be effective by inducing necrosis on the surface of the skin (Fig. 1B), though hyperthermia itself may not have sufficient effect to cause tumour regression. Therefore, combination treatment with sufficient freezing is important for controlling the tumour, while hyperthermia may accelerate the anti-tumour effects of cryosurgery.
4. Conclusion
Combination cryosurgery with hyperthermia may be an alternative treatment for unresectable breast cancer skin metastases which fail to respond to chemotherapy and/or radiotherapy.
Conflicts of interest
None.
Funding
None.
Ethical approval
All the patients in our department are informed that their clinical cases may be published in anonymous format.
Author contributions
JH and KD treated the patient. JH and MF wrote the paper.
References
- 1.Krathen R.A., Orango I.F., Rosen T. Cutaneous metastasis: a meta-analysis of data. South Med J. 2003;96:164–167. doi: 10.1097/01.SMJ.0000053676.73249.E5. [DOI] [PubMed] [Google Scholar]
- 2.Dawber R. Cryosurgery: unapproved uses, dosages, or indications. Clin Dermatol. 2002;20:563–570. doi: 10.1016/s0738-081x(02)00265-1. [DOI] [PubMed] [Google Scholar]
- 3.Dong J., Liu P., Zhang A., Xu L.X. Immunological response induced by alternated cooling and heating of breast tumor. Conf Proc IEEE Eng Med Biol Soc. 2007;2007:1491–1494. doi: 10.1109/IEMBS.2007.4352583. [DOI] [PubMed] [Google Scholar]
- 4.Van der Zee J. Heating the patient: a promising approach? Ann Oncol. 2002;13:1173–1184. doi: 10.1093/annonc/mdf280. [DOI] [PubMed] [Google Scholar]
- 5.Vernon C.C., Hand J.W., Field S.B., Machin D., Whaley J.B., van der Zee J., et al. Radiotherapy with or without hyperthermia in the treatment of superficial localized breast cancer: results from five randomized controlled trials. International Collaborative Hyperthermia Group. Int J Radiat Oncol Biol Phys. 1996;35:731–744. doi: 10.1016/0360-3016(96)00154-x. [DOI] [PubMed] [Google Scholar]