

Abstract
Background:
Sexual function and activity in old age have been inadequately studied world over. It is important to know that aging processes are not confined to persons beyond the age of 60 years; many changes in elderly have their antecedents in the middle age.
Aims:
This study sought to determine the patterns of sexual activity and function in individuals over 50 years of age. It also sought to discuss barriers such as chronic illness that may interfere with sexual function.
Materials and Methods:
We conducted a study of subjects above the age of 50 years in various outpatient departments (OPDs) of a teaching municipal hospital in Mumbai, by interviewing 60 individuals who attended the OPDs, after taking their informed consent. Socio-demographic and other information on their sexual function and activities were obtained. Data was analyzed using statistical package for social sciences v15.
Results:
72% individuals below 60 were sexually active, while only 57% above 60 were active. Others had become completely abstinent at some time in their lives. Statistical analysis revealed significant gender, health and educational status based differences in the sample.
Conclusion:
Our study showed significant presence of sexual desire, activity and function even after the age of 50 years; a decline by the age of 60 and above was a finding that reflected more in women. Chronic illness did affect sexual function and desire.
Keywords: Elderly, illness, sexual activity, sexual desire, sexual function, sexuality
INTRODUCTION
Although recognized as a fundamental driving force, human sexuality is frequently misunderstood and particularly in the elders, neglected.[1] Human beings are actually never too old to enjoy a happy and healthy sex life. Despite this, many people, young and old alike, are astounded at the idea of people remaining sexually active in their sixties and beyond. It is frequently assumed that elder persons lose their sexual desires or that they are physically unable to perform. For the elders, the ability to remain sexually active is a major concern in their lives. Fear about the loss of sexual prowess in older males is common. Older women also express sexual desire, but may fear their interest is undignified and disgraceful. Some elder persons may even freely accept their interests in sex, but their children or grandchildren may disapprove, making them feel guilty. The elder often view sexuality as an expression of passion, affection, admiration, and loyalty, a renewal of romance, a general affirmation of life, especially the expression of joy and a continuing opportunity for growth and experience. In addition, sexual activity is a means for the elder to affirm physical functioning, to maintain a strong sense of identity and establish self-confidence, and to prevent anxiety. It remains a mode of pure physical pleasure as well. However, not all elder persons have positive attitudes about sexuality. Like all persons, elders may experience sexual dysfunction due to boredom, fear, fatigue, grief, or other factors (e.g., intrinsically low sexual desire, physical disability). Sexuality in the elder is particularly affected by problems that are common in this age group, for example, depression, medical disorders, or incapacitation or death of a partner.[2]
Aging is characterized by physiological, pathological, behavioral, and psychosocial changes that can all affect sexual functioning, and it is difficult to disentangle their individual effects. Clinicians tend to ignore this aspect of the lives of elders, who themselves can find sexual problems very difficult to talk about. In psychiatric interview of elders, sexual history and details are often omitted. Human sexuality and particularly sexuality in the elderly is an area that requires more attention in psychiatric training.[3] A marked increase in life expectancy over the past century has meant that individuals over the age of 65 years form an increasingly large proportion of our population. Yet, very little attention has been paid until recently to the treatment of sexual dysfunction in older adults. Older individuals are generally erroneously viewed as asexual people who have lost both their interest in sex and their capacity for sexual behavior.[4]
MATERIALS AND METHODS
The study was a cross-sectional, single interview study that was approved by the Institutional Review Board. We interviewed 60 consecutive elder individuals (30 men and 30 women) above the age of 50 years from the Geriatric, Hypertension, Rheumatology and Diabetes outpatient departments (OPDs) of a tertiary hospital in Mumbai after obtaining their informed consent. Individuals with any previously diagnosed psychiatric disorders or dementia or HIV-positive individuals were excluded from the study. Subjects were briefed about the study and were interviewed to answer a self-prepared questionnaire probing into various areas of sexuality. Data was pooled and statistical analysis was done using statistical package for social sciences (v15); chi-square test was applied wherever necessary.
RESULTS
The population characteristics were as follows:
Individuals in the age group between 50 and 60 years comprised 41.7% of our study population (group I), while the rest (58.3%) consisted of those aged 60 years and above (group II). Around 88.3% had their spouses alive at the time of the interview; 83.3% were staying with their spouses, 53.3% were working and 76.8% were educated, ranging from primary level to postgraduate level.
36.7% subjects did not have any diagnosed major illness. 18.3% were hypertensive, 15% were diabetic, 10% had arthritis, and 8.3% had experienced an episode of stroke in the past, while 11.7% were patients with diagnosed cardiac illness. Of those who were ill (63.3%), approximately 28.3% had an illness of more than 5 years duration.
The findings in different areas of sexuality in the subjects were as follows:
Factors affecting sexual desire and sexuality
The term sexuality for this study meant the sexual experiences and expressions of subjects’ in-totality, and included their sexual function, fantasy, orientation, behavior, and various other aspects. As high as 70% subjects perceived that their age negatively affected their sexuality (P=0.05; likelihood ratio=0.02). In every decade of life after 50, more number of subjects said that their age had affected their sexual desires “very much”; almost 42.9% subjects in group II attributed age to be responsible for their diminishing desires compared to 28% in group I [Figure 1]. Subjects in group I attributed their reduced sexual desires to loss of partner as a significant factor (24%).
Figure 1.
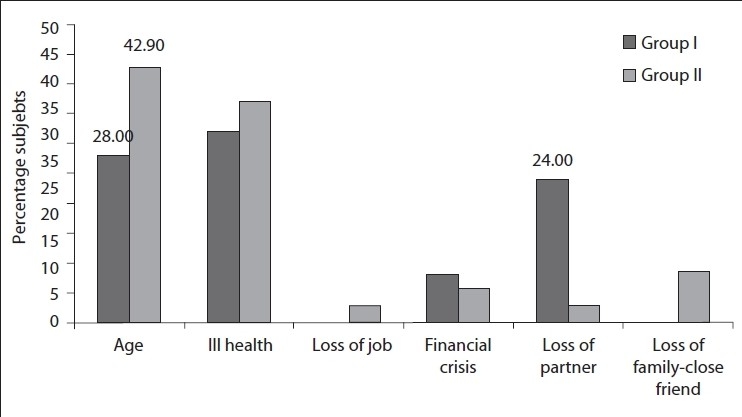
Factors affecting sexual desire
Approximately 43% women reported that their sexuality was affected by increasing age, while 56.7% men reported their sexuality being affected by their deteriorating health [Table 1]. It was interesting to know that 20% of women subjects were affected sexually due to loss of partner or other family member as compared to 3.3% men. These findings were statistically significant (P=0.008).
Table 1.
Gender and factors affecting sexual desire

A greater number of women subjects at all age groups in our sample reported “very much” decrease in their sexual desire (66.7%). Although this was not statistically significant (P=0.3), such change in sexual desires and behavior over the life cycle is normal.[5]
A greater number of nonworking elderly subjects (75%) showed “very much” decrease in their sexual desires, as compared to the working subjects (37.5%), which was statistically significant (P=0.004), thus proving the fact that an active and working lifestyle may help to keep one sexually active for a longer time. Presence of any illness caused “very much” or “quite a lot” reduction (89.5%) in the sexual desires in all subjects (not significant).
Sexual interest, activity and function
About 52% subjects in group I still wanted to experience sexual intercourse or in other words were interested in sexual activity at least once per week or daily; however, only 40% actually experienced it in the past 1 year at that frequency. A similar pattern was also seen in group II, wherein 25.7% individuals were still interested in continuing their sexual activity, while only 14.3% were actually experiencing it at least once per week or daily. However, this pattern was not found in “once per month” frequency for either groups. 72% subjects in group I were still sexually active, as compared to only 57.1% in group II [Figure 2]. In total, 83.4% men in our sample were still sexually active after the age of 50.
Figure 2.
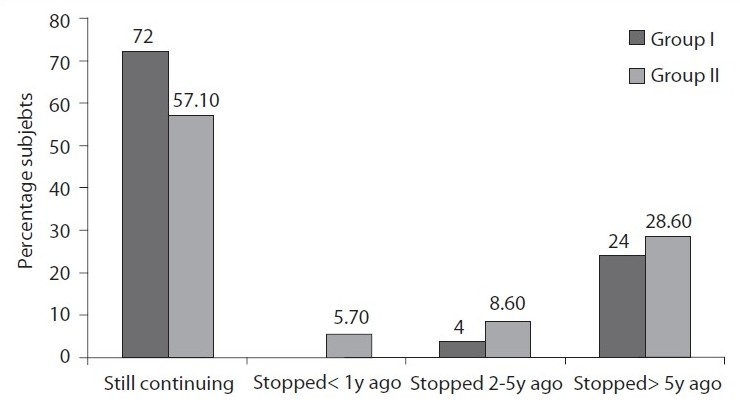
Sexual activity
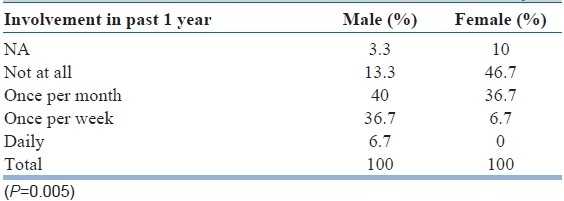
Across both groups I and II, women in our sample showed less interest in non-sexual activities like holding hands, kissing, hugging [Table 2] (P=0.03), and also masturbating or sexual activity [Table 3]. While only 43.4% women reported some interest in non-coital activity, almost double, that is, 83.3% men in both the groups, showed this interest. Similarly, they engaged less in such activities [Tables 4 and 5]. This was found to be statistically significant. While 43.4% women in our study were still sexually active, older men of almost double that number (83.4%) were sexually active, which was significant (P=0.005). Thus, it was seen that men, even in old age, were more interested and participating in both non-coital as well as coital activities with their spouse [Tables 2–5].
Table 2.
Gender and interest in non-sexual activity

Table 3.
Gender and interest in sexual activity
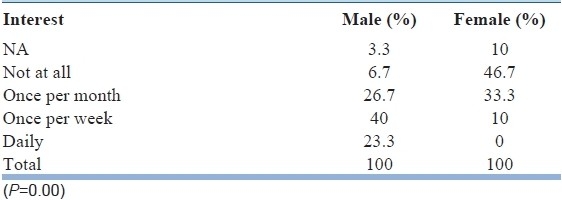
Table 4.
Gender and involvement in non-sexual activity

Table 5.
Gender and involvement in sexual activity
Above 50 years, more women (56.6%) had stopped sexual activity at some time due to varied reasons than men (16.6%) (P=0.012). Thirty percent women in our study reported loss of sexual interest in self as the cause of stopping their activity, as compared to 6.7% men who reported a loss of interest to be the cause. This was also reflected the other way round. Of the men who had stopped sexual activity, 3.3% attributed it to the loss of partner's interest in sex. Women, on the other hand, did not report anything like this. Overall, we found sexual activity in elder men to be more than in elder women. As pointed out earlier, men reported sexual inactivity because of lack of desire, ill health, or erectile dysfunction in their old age, whereas women reported sexual inactivity due to loss of partner.
Almost 100% individuals of group II agreed that they took significantly (P=0.002) more time for sexual arousal compared to before. Age also affected the erection obtained. Overall, 31.4% men above the age of 50 reported erection stiffness “just sufficient for intercourse”. Around 28.7% men in group II reported poor quality of erection for intercourse as compared to 8% men in group I (P=0.04). Poor quality of erection was defined as insufficient erection for intercourse. Erection was assessed by asking the subjects about frequency of sexually stimulated erections, morning erections and spontaneous erections, and the stiffness of erection was compared to erections in the youth. Twenty-six percent subjects with illness reported some or the other form of erectile dysfunction as compared to only 9% of healthy subjects. Men in group II (45.7%) also perceived a significant decrease in the amount of ejaculatory volume (P=0.04) as compared to those in group I; however, this change did not distress most of the subjects in the study.
All women in our study reported a difference in vaginal lubrication as compared to that in young age. Twenty percent women in group I reported poor quality of lubrication, as opposed to 40% women from group II who reported poor quality of lubrication, insufficient for intercourse (P=0.4).
We asked the subjects to compare their current sexual capacity with their capacity 1 year after their marriage. Sex now was worse than before for 75% of them (76% for women, 73% for men). Subjects with any illness (84%) reported greater worsening of sexual pleasure as compared to those without illness (59%) (P=0.07; likelihood=0.05). Although this was not statistically significant (P=0.06), more number of subjects in group II (83%) reported worse orgasm at this age than when they were young (likelihood ratio=0.04). Similarly, subjects with illness reported higher reduction (81%) in the intensity of orgasm as compared to those who were healthy (54%) (P=0.07; likelihood=0.05). A larger percentage (71.4%) of subjects in group II did not get distressed by this decrease in orgasmic intensity. This difference in perception of orgasm with age was statistically significant (P=0.04). Working subjects with no illness adjusted best and expected this age-related change in orgasmic intensity (P=0.03). On the other hand, people who were not working or people with illness were less adjusted to this change. Both these findings were statistically significant.
Approximately 78% subjects reported no sexual dreams of any type. Of the other 22% who reported dreams, majority had dreams at a frequency of around 3–4 times/month, irrespective of gender. It was interesting that one of these women, who reported very frequent sexual dreams, was in fact separated from her husband and dreamt of having intercourse with him frequently. Thirty percent men reported having dreams of a sexual nature as opposed to 13.3% women above the age of 50.
96.7% subjects in our sample did not masturbate at all. There was no gender difference noted. Only 6.6% men above the age of 50 masturbated.
All study subjects were asked about their preferred role in sex (i.e. active or passive). We found a significant difference (P=0.00) in this; almost all men preferred to be active partners while all women preferred to be passive partners.
Love and intimacy
Around 48% subjects in our study did not perceive any change in the areas of love and intimacy in their relationship over the years, while these areas had improved in 25% of the subjects’ lives and worsened for 13.3% of them. The subjects were asked how much role, sex had played in their relationships over the years. Only 26.7% subjects in our study thought that sex had played 100% role in their marital relationship over the years, while 41.7% felt it had only played 50% role. A small percentage (13.3%) felt that sex was only a minor role player in their relationships. Educated elderly subjects attributed a greater role played by sex in their relationship with their spouses (P=0.002; likelihood ratio=0.004).
DISCUSSION
This study was done in a sample of 60 individuals above the age of 50 years, and three broad areas related to sexuality in the elder were studied, including factors affecting sexual desire, sexual activity and function, and love and intimacy.
The results of this study leave little doubt that intact sexual function is common among elder people, even among those above 60 years (group II). But definitely there was a declining course of sexual functions including a decrease in sexual desire with increasing age, with a steep course in group II. This finding is similar to that of Pfeiffer et al.[6] Subjects in group I being young, did not expect loss of partner at their age, and so this was the main factor worrying them for their decreasing sexual desires as opposed to those in group II, who did not attribute loss of partner as an important factor in affecting their sexual desires as this was something that was more common in their age group and something which they may have been ready for.
Changes brought on by age can often make a person's sex life more difficult,[7] but there is still an internal drive or need for sexual fulfilment. Continuation of sexual activity for elder persons in many societies indicates that cultural factors may be key determinants in their sexual behavior.[8] Our society has generally been viewed as restricting the sexuality of older adults. Although many old people experience sexual difficulties, traditionally they have presented for treatment relatively infrequently, being more prepared to live with the problem than younger adults.[9,10] However, this picture seems to be changing recently with an increase in the number of elder persons seeking treatment for sexual difficulties,[11] even in the Indian setup.
Deacon et al.[12] suggest that a decline in sexual activity for men is less likely to be due to the lack of a partner, while in women it is more likely to be due to this reason and that too at any age. George and Weiler[13] similarly reported illness and deteriorating health as the major reason for reduced sexual desires and activity in men in their study, while women reported loss of partner as the major factor. Loss of partner is both commoner and more of a handicap for women in that they survive longer than men and tend to be younger than their husbands.[14] The greater decrease in sexual desire in women at all age groups in our study may reflect the influence of socio-cultural factors in determining the libido of elderly women.[8]
There are many causes for women's sexual problems, especially in old age, including shame and guilt, sexual abuse, interpersonal conflicts, depression and religious and cultural prohibitions.[15] Some women use changes at midlife as a reason to stop being sexual. Earlier unhappy and unsatisfying sexual experiences may lead some women to find relief in their loss of sexual feelings and capacities at midlife and encourage them to hide behind the belief that they are “too old for sex”.[16] Older adults experience sexual problems and concerns which are not that different from those of young people; however, biological and psychological factors may need to be looked at more closely with an aging population.[17]
Even though it was not studied in detail, illness did have a negative effect on sexual desires in our subjects. The incidence of sexual dysfunction and decreased sexual desires increases in old age, but it is possible that this is primarily related to the increased rate of health problems, rather than old age per se.[18] However, it is not right to assume that physical changes associated with advancing age reduce the opportunity to enjoy sex.[12]
Numerous endocrine, vascular and neurological disorders may interfere with sexual function, just as many forms of medications and surgeries. These health factors are more prevalent in older people, and hence it is perhaps not surprising to find an increase in biologically caused sexual problems in the elderly.[18] Deacon et al.[12] indicate that the pathological factors that affect sexual function include cardiovascular disease, diabetes mellitus, dementia, arthritis, and surgery. They also indicate that pharmacological factors play a role in sexual problems.[12,16,19] There is a possibility that some of these issues might have interfered with sexual functioning in our subjects. We need to put it across to the elderly individuals that some illnesses and disabilities require that the couple experiment with new positions for intercourse or they could experiment with “outercourse”[20] which refers to the non-sexual activities like kissing, hugging, caressing, etc.
Although the subjects in our study maintained a definite interest in sexual activity, their activity itself had declined substantially for both the groups. This concept has been called the ‘interest-activity gap’, wherein older adults have an interest in maintaining their sexual activity; however, the sexual activity per se decreases.[2,6,21]
A larger percentage of men (83.4%) were maintaining their sexual activity even after the age of 50 years. All others had stopped their sexual activity at some time or the other. This was slightly more than that reported by Helgason et al.[22] and Antonovsky et al.[23] wherein approximately 71% men in their sample were having sexual intercourse after the age of 50.
The interest as well as involvement in both sexual and non-sexual activities was reported to be significantly less by women in our study, which reflected the findings of Lindau et al.[24] who reported that women were less likely than men at all ages to report sexual activity. Men in our sample were more interested as well as involved in both these activities, as was seen by Pfeiffer et al.[2] In an earlier Indian study, Sanger et al.[25] had reported a rate of 63.2% non-coital activity in their sample of 120 elderly men. Changes in sexual expression and preferred sexual activity may be common with advancing age,[26] and one can see a shift from sexual activity to non-sexual petting and caressing or touching.
Even when it comes to sexual activity, the time taken for sexual arousal is increased. The bio-physiological changes in old age predispose to increased time for arousal that has been well reported in literature.[27] The quality of erection was poor in men of group II. It is seen that after the age of 35 or 40 years, most men may have erectile difficulties and may need direct penile stimulation to get an erection.[19] In a study by Helgason et al.[22] on men aged 50–80 years, 68% men reported erection stiffness just sufficient for intercourse, which was reported by only 31.4% men in our study. Men in group II who reported a significant decrease in ejaculatory volume did not get distressed by it. It is known that changes occurring in the sexual physiology of an aging male can affect both erectile function and ejaculation. These changes need not have any functional impact on the subjective enjoyment of the sexual encounter. However, knowledge that these changes are not dysfunctional and assistance with the adjustment of sexual practices may be crucial in preventing dysfunction in them.[12]
Corresponding to this finding, women in our study reported decreased vaginal lubrication which pointed to an important age-related change in the physiology in women,[28] that may be responsible for painful intercourse, if the vaginal walls become excessively thin.[18]
As would be expected, the quality of sex had worsened for most of our subjects, and more so for those with any of the chronic illness. Chronic illness can have profound negative effects on relationship and sexual satisfaction of both patients and their partners.[29] This could be due to impaired sexual fulfilment as a result of anxiety, loss of self-esteem, grief and depression associated with chronic illnesses.[30] Orgasms were similarly of poor quality for more subjects in group II and those with illness as compared to those in group I or the healthy subjects. In old age, orgasms may be less intense than in the youth, which is an expected physiological change. Sexual and orgasmic dysfunction may often be related more to chronic illness than to aging alone,[31] which is why chronically ill individuals perceive greater deterioration in sexual and orgasmic quality at any age. As the subjects grew older (group II), they did not get distressed by the decrease in orgasmic intensity since they knew it was inevitable and had adjusted to it accepting the physiological changes.
On similar lines, very less percentage of men in our sample masturbated, which was contrary to the findings of Bergstrom-Walan and Nielsen,[32] where 51% men between the ages 60 and 80 reported masturbation at least once a month, but then that was a Western sample. A number of myths present at that age group could have been the main reason behind it,[33] one of which was that masturbation “ruins” a person for partner sex. Masturbation is a natural supplementary activity within a relationship,[19] but was very less practised in our sample of individuals (3.4%). Even today, many people do not treat masturbation as a normal and enjoyable activity.[19]
In a sexual encounter, the subjects in our sample stuck to the conventional sexual roles, with men preferring to perform as active partners and women as passive. In most sexual encounters, there has to be one active (masculine) and one passive (feminine) partner.[27] Men and women tend to conform to their gender roles and behave as active or passive in their sexual encounters, which probably continues in old age.
The areas of love and intimacy remained same as they were in their youth for a large percentage of our subjects. Cultural factors probably reflect in the solidarity of relationships till old age.[8] In men, whether or not erectile capacity is retained, the decision to continue intimacy is often socio-cultural.[8] The quality and frequency of intimacy and intercourse may decline with age; however, satisfaction with sexuality may not be affected.[34]
It was the educated subjects who attributed a greater importance to sex in their relationship with their spouses, which shows that education does play a vital role in sexuality and intimacy. Knowledge of sexuality and its importance may perhaps enhance its role in an educated individual's relationship. This finding definitely opens up new areas in research on the role of education in sexual attitudes. Pfeiffer and Davis[35] had pointed out that educational level is an important predictor of sexual interest, frequency and enjoyment for women.
Agism, or the acceptance by us and society at large that old age is associated with loss and decline, is all the more marked in the field of sexuality. Our study on sexual desire, sexual interest, activity and function, and love and intimacy in the Indian elderly people was an eye opener even for us.
Limitations
The sample size of the study was very small. We had used an interviewer-based questionnaire that was not self-administered which might have been more forthcoming. The effect of illness like diabetes, hypertension and their medications and its impact on sexual functioning of the subject was not a part of the study.
CONCLUSION
To conclude, our study found that overall sexual activity showed a declining course with increasing age but still continued in individuals above 50 years of age. The increasing ‘interest-activity gap’ was very well demonstrated in our study in both group I (50–60 years) and group II (>60 years) subjects. Significant gender differences were found in that women were less interested and also less involved in both coital as well as non-coital activities. A better sexual function was seen with an active and working lifestyle in old age in our sample. The study showed significant reduction in the following parameters with increasing age: Quality of erection, ejaculate volume, vaginal lubrication, orgasmic pleasure and overall sexual functioning. However, the subjects did not seem to be distressed with these changes. Further, presence of co-morbid illness worsened sexual function and sexual activity.
Both sexes reported a significant increase in the time required for sexual arousal. The reasons for stopping sexual activity differed significantly in case of either gender, with loss of a partner in women and deteriorating health in men being the most important ones. Love and intimacy stayed the same for majority of our subjects.
These findings warrant considering sexual function in clinical decision making and the design of clinical trials in elder men and women. It also opens doors to a new area for research into geriatric sexuality, much of which lies neglected till now.
Footnotes
This paper won Bombay Psychiatric Society Silver Jubilee National Award at the 60th Annual National Conference of Indian Psychiatric Society, in Kolkata on 4th January 2008.
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Walker BL. Sexuality and the elderly: A research guide. Annotated ed. Westport, CT: Greenwood Press; 1997. [Google Scholar]
- 2.Pfeiffer E, Verwoerdt A, Davis GC. Sexual behavior in middle life. Am J Psychiatry. 1972;128:1262–7. doi: 10.1176/ajp.128.10.1262. [DOI] [PubMed] [Google Scholar]
- 3.Bouman WP, Arcelus J. Are psychiatrists guilty of “ageism” when it comes to taking a sexual history? Int J Geriatr Psychiatry. 2001;16:27–31. doi: 10.1002/1099-1166(200101)16:1<27::aid-gps267>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 4.Tien-Hyatt JL. Self-perceptions of aging across cultures: Myth or reality? Int J Aging Hum Dev. 1986-1987;24:129–48. doi: 10.2190/mcf9-22dm-8hpa-p3f4. [DOI] [PubMed] [Google Scholar]
- 5.Garnets LD, Peplau LA. A new paradigm for women's sexual orientation: Implications for therapy. In: Kaschak E, Tiefer L, editors. A new view of women's sexual problems. Binghamton, NY: Haworth Press; 2001. pp. 111–22. [Google Scholar]
- 6.Pfeiffer E, Verwoerdt A, Wang HS. The natural history of sexual behavior in a biologically advantaged group of aged individuals. J Gerontol. 1969;24:193–8. doi: 10.1093/geronj/24.2.193. [DOI] [PubMed] [Google Scholar]
- 7.Rasilainen R. 7 Myths about senior sex. Reader's Digest. 2007;48:47–52. [Google Scholar]
- 8.Winn RL, Newton N. Sexuality in aging: A study of 106 cultures. Arch Sex Behav. 1982;11:283–98. doi: 10.1007/BF01541590. [DOI] [PubMed] [Google Scholar]
- 9.Baikie E. Sexuality in the elderly. In: Hanley I, Hodge J, editors. Psychological approaches to the care of the elderly. Illustrated ed. London: Croom Helm; 1984. pp. 237–254. [Google Scholar]
- 10.Wise TN. Sexual problems in the aged and incapacitated. In: Meyer JK, Schmidt CW, Wise TN, editors. Clinical management of sexual disorders. Baltimore: Williams and Wilkins; 1983. [Google Scholar]
- 11.Renshaw DC. Sexuality in old age, illness and disability. In: Wheatley D, editor. Psychopharmacology and sexual disorders. Oxford: Oxford University Press; 1983. pp. 88–100. [Google Scholar]
- 12.Deacon S, Minichiello V, Plummer D. Sexuality and older people: Revisiting the assumptions. Educ Gerontol. 1995;21:497–513. [Google Scholar]
- 13.George LK, Weiler SJ. Sexuality in middle and late life. The effects of age, cohort, and gender. Arch Gen Psychiatry. 1981;38:919–23. doi: 10.1001/archpsyc.1981.01780330077008. [DOI] [PubMed] [Google Scholar]
- 14.Bouman WP. Sexuality in later life. In: Jacoby R, Oppenheimer C, Dening T, editors. Oxford textbook of old age psychiatry. illustrated ed. New York: Oxford University Press; 2008. p. 693. [Google Scholar]
- 15.Leiblum S. The role of the sex therapist in female sexual dysfunction. New York: University School of Medicine Conference; 2002. Dec 7, [Google Scholar]
- 16.Levine SB. Sexuality in mid-life. 1st ed. New York: Plenum Press; 1998. p. 91. [Google Scholar]
- 17.Leiblum SR, Segraves RT. Sex therapy with aging adults. In: Leiblum SR, Rosen RC, editors. Principles and practice of sex therapy. New York: Guilford Press; 1989. pp. 352–81. [Google Scholar]
- 18.Spence SH. Psychosexual dysfunction in the elderly. Behav Change. 1992;9:55–64. [Google Scholar]
- 19.Butler RN, Lewis MI. The new love and sex after 60. 3rd ed. New York: Ballantine Books; 2002. [Google Scholar]
- 20.Klein M, Robbins R. Let me count the ways: Discovering great sex without intercourse. New York: Tarcher; 1999. [Google Scholar]
- 21.Long BC, Phipps WJ. Adult nursing: A nursing process approach. Illustrated ed. London: Elsevier Health Sciences; 1995. p. 746. [Google Scholar]
- 22.Helgason AR, Adolfsson J, Dickman P, Arver S, Fredrikson M, Göthberg M, et al. Sexual desire, erection, orgasm and ejaculatory functions and their importance to elderly Swedish men: A population-based study. Age Ageing. 1996;25:285–91. doi: 10.1093/ageing/25.4.285. [DOI] [PubMed] [Google Scholar]
- 23.Antonovsky H, Sadowsky M, Maoz B. Sexual activity of aging men and women: An Israeli study. Behav Health Aging. 1990;3:151–61. [Google Scholar]
- 24.Lindau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357:762–74. doi: 10.1056/NEJMoa067423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sanger KS, Singh PK, Prakash J, Singh A, Chaudhury S, Sharma DK, et al. Aging and sexuality- A study of sexual behaviour of elderly males. Ind Psychiatry J. 2007;16:42–4. [Google Scholar]
- 26.Starr BD, Weiner MB. Report on sex and sexuality in the mature years. London: W. H. Allen / Virgin Books; 1981. [Google Scholar]
- 27.Haeberle EJ. The sex atlas. New popular reference edition. New York: The Continuum Publishing Company; 1983. [Last accessed on 2010 November 24]. Available from: http://www2.rz.hu-berlin.de/sexology/GESUND/ARCHIV/ATLAS_EN/atlas.htm . [Google Scholar]
- 28.Barbach LG. The pause: Positive approaches to perimenopause and menopause. Revised edition. New York: Plume; 2000. [Google Scholar]
- 29.Parish KL. Sexuality and haemophilia: Connections across the life-span. Haemophilia. 2002;8:353–9. doi: 10.1046/j.1365-2516.2002.00647.x. [DOI] [PubMed] [Google Scholar]
- 30.Jensen SB. Sexual relationships in couples with a diabetic partner. J Sex Marital Ther. 1985;11:259–70. doi: 10.1080/00926238508405452. [DOI] [PubMed] [Google Scholar]
- 31.Mulligan T, Retchin SM, Chinchilli VM, Bettinger CB. The role of aging and chronic disease in sexual dysfunction. J Am Geriatr Soc. 1988;36:520–4. doi: 10.1111/j.1532-5415.1988.tb04022.x. [DOI] [PubMed] [Google Scholar]
- 32.Bergstrom-Walan MB, Nielsen HH. The sexual expression among 60-80 years old men and women; A sample from Stockholm, Sweden. J Sex Res. 1990;2:289–95. [Google Scholar]
- 33.Schover LR, Jensen SJ. Sexuality and chronic illness: A comprehensive approach. illustrated ed. New York: Guilford Press; 1988. [Google Scholar]
- 34.Bretschneider JG, McCoy NL. Sexual interest and behaviour in healthy 80- to 102-year-olds. Arch Sex Behav. 1988;17:109–29. doi: 10.1007/BF01542662. [DOI] [PubMed] [Google Scholar]
- 35.Pfeiffer E, Davis GC. Determinants of sexual behavior in middle and old age. J Am Geriatr Soc. 1972;20:151–8. doi: 10.1111/j.1532-5415.1972.tb00789.x. [DOI] [PubMed] [Google Scholar]