

Introduction
Well-child care is a core service of primary care with the overall goal of promoting the physical health, cognitive growth, and emotional well-being of children. Leaders in child health care recommend that to achieve this goal, primary care physicians use a parent-centered approach, with a focus on the parent–child relationship in the context of family, culture, and community.1 To meet this goal in the family medicine residency program at the University of California, San Francisco Department of Family and Community Medicine, we are testing the use of Centering Parenting,2 a parent-centered group-care model for providing well-child care to address the needs of our socioeconomically disadvantaged patient population. Here we describe the use of this model and report on its evaluation.
Patients begin their experience in prenatal groups, then transition into parenting groups. This approach emphasizes the parent- and group-centered concepts developed in prenatal groups, specifically the integration of health assessment, education, and support. To integrate these concepts, Centering Parenting focuses on continuing positive support by valuing and building on successes within groups started during pregnancy. Relationships that develop in prenatal groups support peer-to-peer learning and trust, and they transition well into Centering Parenting, where parents continue to build on their collective knowledge about caring for their babies. The groups have an average size of four mother-baby pairs.
Methods
Since the pilot began in 2010, 3 parenting groups have been established, and they meet over the course of a year on an expanded schedule (including visits when members' babies are 2 weeks, 4 weeks, 6 weeks, 8 weeks, 3 months, 4 months, 6 months, 8 months, 10 months, and 12 months old for a total of 10 visits). Each group visit lasts for 2 hours, with an additional 1 hour required for premeeting planning and postmeeting reflection. Three residents in postgraduate year 2 or 3, chosen for specific groups on the basis of language concordance and schedule, are participating in the pilot program, one connected with each group. The residents attend a daylong, on-site training program led by instructors certified in the Centering Parenting model of facilitating group visits. Within our clinical setting, the coordinator is a faculty member trained in the facilitation techniques.
The faculty member and residents meet before the group does and plan the opening, content, and structure of the group. Various openings are used, including games and stress-reduction exercises. The content is based on relevancy to the group at that time. For example, the Edinburgh Postpartum Depression Scale is employed in the early infancy period, especially to discuss stress, support, and self-care for mothers. Early on, infant massage is taught as a means for bonding with and calming babies. As the babies get older, more time is devoted to doing developmental activities. The physicians do all of the examinations and individual portions with patients and assist in mothers' self-measurements (pressure and weight) and obtain measurements of the babies. After a brief check-in, parents pose questions to their group for discussion. All questions that come up in the private physician-parent encounter are discussed by the groups, and parents use their collective insight to educate one another. Any necessary individual care, such as placement of intrauterine devices or vaccination, is done after the groups meet. Also after the groups meet, the residents and faculty members participate in debriefing for self-reflection and continued teaching.
The physicians participating in the groups were surveyed regarding their experience of the program when the groups had completed their ten sessions. The items were presented as dichotomous yes/no choices.
Results
The results of the physician survey appear in Table 1. The physicians reported significant improvement in most areas of their skills and knowledge. As one of our residents said,
It has been one of my favorite experiences of residency. It is such a privilege to get to learn from our patients about the range of normal, and even more exciting, to see how empowered they feel teaching each other. I wish we all had the chance to have this experience as residents, and I really think it is the wave of the future in terms of how to best provide family-centered maternal and child health care in a primary care setting.
Table 1.
Evaluative results of physician surveys
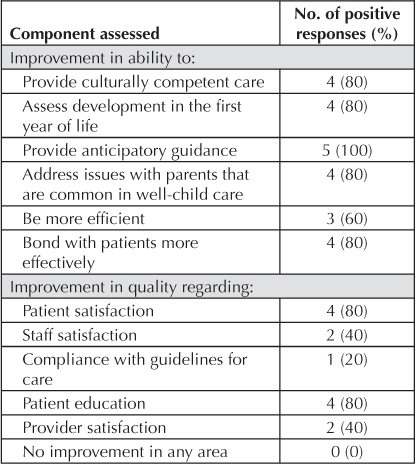
This sentiment was mirrored by the patients' reports of their experiences: In focus-group discussions, they universally said that the biggest group advantage was developing closer relationships with physicians and having the support of their peers. However, physicians' satisfaction levels and their perception of staff satisfaction levels were mixed, suggesting that the change in practice represented by the Centering Parenting program was perceived as challenging for both physicians and staff.
Discussion
In contrast to standard care, the Centering Parenting model allows residents to experience comparative development as well as interactions among a group of parents and children. We believe that the biggest advantage that this group exercise offers residents is the ability to see many babies at the same time longitudinally. They can see development in motion: the one-month-old baby compared with the three-month-old baby in the group; signs that the parents notice to determine readiness for solids; discussions about home safety for a child who has started crawling. These discussions and the availability of all of the babies at the same time, on an ongoing basis, provide education in child development that is clearer and longer-lasting than afforded by traditional well-child care. Also, because most residents do not have their own children, the group setting performs the important function of helping them to learn about child development in a much more organic way than the traditional care setting allows. Additionally, the expanded schedule of the group model allows for more time to learn and discuss development, both with parents and with residents.
… the biggest group advantage was developing closer relationships with physicians …
The extra time with patients provided by the group model forges a stronger bond between physician and parent. Patients are supported in their own context: their peers from the community. Group discussions engage patients, who share their culture and parenting practices with the rest of the group.
We believe that this model of teaching and providing well-child care is effective in promoting the overall health of children and their families. Beyond its early success, integrating this program into our residency program as a whole remains a challenge. We are currently planning the expansion of the pilot program for residents in postgraduate year 2 and 3.
Disclosure Statement
The author(s) have no conflicts of interest to disclose.
Acknowledgments
The author wishes to thank Peter Sommers, MD, for his support. Katharine O'Moore-Klopf, ELS, of KOK Edit provided editorial assistance.
References
- Schor EL. Rethinking well-child care. Pediatrics. 2004 Jul;114(1):210–6. doi: 10.1542/peds.114.1.210. [DOI] [PubMed] [Google Scholar]
- Centering Healthcare Institute [homepage on the Internet] Boston, MA: Centering Healthcare Institute, Inc; © 2009–11 [cited 2011 Sep 22]. Available from: www.centeringhealth-care.org. [Google Scholar]