

Abstract
Neuroergonomics provides a multidisciplinary translational approach that merges elements of neuroscience, human factors, cognitive psychology, and ergonomics to study brain structure and function in everyday environments. Driving safety, particularly that of older drivers with cognitive impairments, is a fruitful application domain for neuroergonomics. Driving makes demands on multiple cognitive processes that are often studied in isolation and so presents a useful challenge in generalizing findings from controlled laboratory tasks to predict safety outcomes. Neurology and the cognitive sciences help explain the mechanisms of cognitive breakdowns that undermine driving safety. Ergonomics complements this explanation with the tools for systematically exploring the various layers of complexity that define the activity of driving. A variety of tools, such as part task simulators, driving simulators, and instrumented vehicles provide a window into cognition in the natural settings needed to assess the generalizability of laboratory findings and can provide an array of potential interventions to increase safety.
Keywords: Older drivers, neuroergonomics
Overview of Neuroergonomics with Respect to Driving
Neuroergonomics is the study of brain and behavior at work (Parasuraman, 2003; Parasuraman & Rizzo, 2007). This multidisciplinary field merges the principles and practice of neuroscience and ergonomics to study brain structure and function in everyday environments. Whereas neuroscience and cognitive psychology have tended to focus on the neural structures and mental processes underlying cognition in controlled laboratory settings, ergonomics is more concerned with naturalistic behaviors. In each case, valuable information about how humans think and act in relation to the environment has been obtained. However, since cognition and behavior are often situational in context, laboratory findings particularly with regard to decision-making and related executive functions may fail to predict behavior in complex and dynamic tasks that people confront in their daily lives. Thus, cognition must be considered in relation to actions and artifacts in the environment. Humans and computers comprise “joint cognitive systems” that function in real-world settings. Consequently, neuroergonomics focuses on neural bases of perceptual and cognitive functions and actions in relation to actual technologies and settings, providing opportunities for translational research between neuroscience, human factors, ergonomics, medicine, engineering, computer science, and the social sciences.
Neuroergonomics can be applied to gain greater understanding of human behavior and performance in a wide range of settings at home, at work and travelling in between. A key representative area where neuroergonomics can be applied is the study of outcomes and safety measures in automobile driving. This paper takes a neuroergonomic approach in examining issues relating to older drivers who tend to be over-represented in fatal crashes on a per-mile basis (Evans, 2004). The proportion of fatal crashes for drivers aged 65 and over is expected to increase due to demographic shifts in the population, with some researchers suggesting a 155% increase by 2030 (Lyman, Ferguson, Braver, & Williams, 2002; McGwin, Owsley, & Ball, 1998). Increased crash risk for older drivers stems from age and disease-related declines in visual, cognitive and attentional impairments (Ball & Owsley, 1993b; Owsley, Ball, Sloane, Roenker, & Bruni, 1991; Preusser, Williams, Ferguson, Ulmer, & Weinstein, 1998).
Several age related declines have been reported in older drivers including diminished visual acuity and contrast sensitivity, diminished night vision, slower and less efficient eye-movements, increased sensitivity to glare, diminished divided attention capacity in complex or cluttered environments, reductions in the visual field of view, etc (see Ball, Vance, Edwards, & Wadley, 2004; Dewar, 2007; Preusser, et al., 1998). Such changes in visual and cognitive ability may diminish the ability of older drivers to extract and respond to information within the driving environment and may explain certain driving maneuver difficulties, such as detecting and understanding traffic control devices (e.g. failure to yield), driving at night, route navigation. In particular, this group of drivers has problems with complex traffic situations, including intersection navigation, making left-turns across traffic, merging into traffic, and making lane changes (McGwin & Brown, 1999; NHTSA, 2009; Preusser, et al., 1998; Zhang, Fraser, Lindsay, Clarke, & Mao, 1998)
In many cases, increased risk for older drivers is probably due to medical factors that accompany aging, rather than just age itself. Age related disorders include mild cognitive impairment, Alzheimer’s disease and associated disorders, stroke, cardiac disease, cancer, diabetes and other systemic disorders that affect brain and body chemistry and produce encephalopathy, a broad term subsuming any kind of cognitive impairment (Filley, 2004). Diabetes provides a prototypical opportunity for linking physiology and behavior in naturalistic settings. While diabetes may chronically affect multiple organ systems (e.g., vision, kidneys, peripheral nerves), a key effect relates to fluctuations of blood sugar causing hypoglycemia (low blood sugar) or hyperglycemia (high blood sugar). Hypoglycemia produces acute cognitive impairments affecting alertness, judgment and risk perception and is commonly caused by insulin, the mainstay of diabetes treatment. Strict control over glucose levels using insulin, intended to reduce chronic systemic complications of diabetes (outlined above) can increase the likelihood of hypoglycemic episodes. Unfortunately, some diabetics are unaware of their hypoglycemia and fail to take appropriate steps to treat the problem and to modulate their behavior to mitigate the risk posed by driving while impaired. A neuroergonomic approach offers the opportunity to link somatic states associated with hypoglycemia to meaningful real world outcomes such as driver errors. This approach can help inform the design and application of countermeasures, such as real-time auditory and haptic feedback to hypoglycemic drivers triggered by low glucose sensor readings from continuous glucose monitoring (CGM) devices (McGarraugh, 2010).
Another example in which the neuroergonomic approach linking behavior and physiology in operational settings can be helpful is in the case of excessive daytime sleepiness, which can be due to a variety of causes, including sleep disordered breathing associated with obstructive sleep apnea syndrome (OSA). OSA impairs visual vigilance (Tippin, Rizzo, Sparks, & Boyle, 2007) and causes microsleeps (few seconds long reduction in the background alpha [8–11Hz] brain rhythms in alert individuals that can be objectively determined by analyses of EEG data) and related changes in vehicle steering (Boyle, Tippin, Paul, & Rizzo, 2008).
It is possible to evaluate brain activity in driving-like tasks implemented in an fMRI scanner (cf Calhoun, McGinty, Pekar, Watson, & Pearlson, 2001; Calhoun, McGinty, Watson, & Pearlson, 2000; Graydon, et al., 2005). The metabolic changes in specific brain areas can be related to visuospatial and motor aspects of driving. Older individuals with neurodegenerative impairment have reduction in activity in posterior parietal and frontal regions (Peters, et al., 2009) that are activated during information processing related to the driving task, underscoring the potential utility of relating measures of brain metabolism with components of driving task performance in older drivers. The brain lesion method provides unique evidence that complements the findings from functional brain imaging and electrophysiological techniques. The lesion method shows which brain structures are necessary for a certain function (Rorden & Karnath, 2004). This method successfully addresses the nature of mental representations and the organization of brain processes (“psychoanatomy”) in animals and humans with brain lesions and is highly relevant to understanding the organization of cognition in drivers with lesions in different cerebral areas caused by various medical conditions (e.g. traumatic brain injury, stroke, tumors). For example, certain decrements might be predicted or expected given the examination of a MRI of a driver with frontal lobe damage such as that illustrated in Figure 1. Given that the frontal lobes have been implicated in attention and working memory, and knowing that these cognitive functions are important for executing complex tasks such as driving, it could be predicted that a patient sustaining extensive damage to the frontal lobe would show impaired driving performance. Identifying and evaluating drivers with various brain lesions offers a means to better understand the processes involved in driving.
Figure 1.
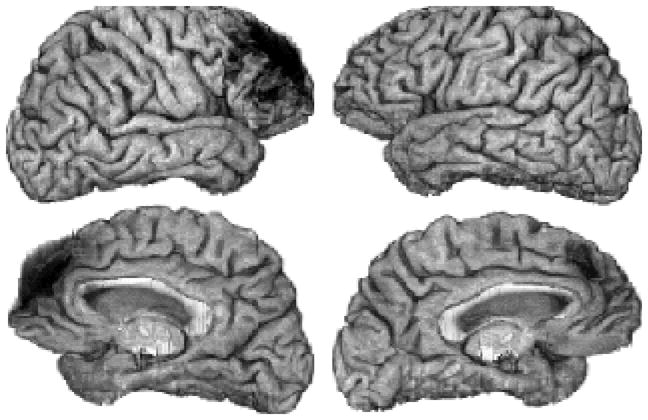
3D magnetic resonance imaging depicts the brain surface of a person with frontal lobe damage (dark areas) and executive dysfunction (which includes impairments of decision-making and implementations). The lateral and mesial surfaces of the right hemisphere are shown, respectively, in the upper and lower left. The left hemisphere surfaces are depicted in the right panels.
A number of tools effective for assessing the cognitive and neurological mechanisms of failure in populations known to have increased crash risk. Figure 2 provides a range of methods and tools for examining driver performance, ranging (left to right) from standardized neuropsychological tests which are capable of measuring levels of cognitive performance in health or disease but may be less sensitive to impairment in driving performance, to computer based tests that may use photographs or video of complex scenes (e.g., change blindness (CB) and hazard perception (HP) tasks), to various types of simulators (task focused, non-motion based, or motion based), to driving a car in controlled situations (on a test track, on a state road test, or on public roads), and naturalistic driving (in the driver’s own car, over extended time frames that follow no set protocol). Complex computer tasks such as the useful field of view (UFOV), CB and HP represent neuropsychological tasks that allow researchers to examine various levels of functioning. For example, CB tasks have been used to assess aspects of working memory and attention in drivers with brain disorders, neurodegenerative disease and to examine the effects of normal aging (Rizzo, et al., 2009; Summers, 2006). HP tasks represent a more global evaluation of aspects such as visual search, attention, and executive functioning that may help researchers understand how drivers identify hazards.
Figure 2.

Various methods used to evaluate driver performance. Trade-offs exist between experimental control and context or fidelity in studies of driving behavior.
As shown in Figure 2, there are tradeoffs in each approach in terms of experimental control and context/fidelity. Each tool has advantages and drawbacks and the method of choice depends on the question being asked. Some tools provide a greater degree of sensitivity and lend themselves better to a fine-grained assessment of cognitive function in at-risk individuals, whereas other tools more closely approximate how drivers might perform in real-world driving settings. As a result, multifaceted approaches to assessing driver performance, including paper and pencil neuropsychological tests, computer based tests of cognitive function, computer simulation, on-road and naturalistic data are likely to provide the clearest picture of driving fitness in at-risk populations (Bieliauskas, 2005; Uc & Rizzo, 2008). The tools outlined in the figure are derived from various disciplines and fit a translational research model as outlined by the National Institute of Health (NIH) roadmap. Translational research is often divided into Types 1, 2, 3, and 4, each being a step in the translation of a basic scientific discovery into a tool or practice that enhances human health. Type 1 refers to the application of new, laboratory-generated knowledge to an emerging method that can be tested using human subjects. Type 2 refines the results of these early human studies in ways that can be used in everyday practice, while Type 3 focuses on the effects of these practices on the community as a whole, helping to shape wider population health studies. Type 4 expresses the broadly circular nature of translational research, evaluating the final health outcomes of a discovery generated in a Type 1 study, providing feedback to the process as a whole.
Though seemingly comprised of discrete stages, translational research is ideally bidirectional in practice. For example, naturalistic driving data and crash statistics help identify at-risk populations that might not otherwise be apparent that can then be investigated with basic cognitive science paradigms in the laboratory. In addition, paper and pencil tests may point to cognitive errors that may undermine driving performance that can be further examined with increasing representative levels of driving context (ranging from CB tasks to HP tasks to interactive simulations with feedback to on-road evaluations) to both identify and understand at-risk populations. In this way, the researcher in basic science has increased awareness of the issues facing the systems designer, or in the case of the transportation researcher, in the translational model a deeper knowledge of the context of the driver. In translational research, feedback is essential, forming an iterative cycle of development that promotes ongoing exploration and advancement until a development goal is achieved, with the continuing possibility of that goal being improved upon. The broadened awareness resulting from multidisciplinary cooperation can reshape the thinking of all involved in the development process, allowing for faster and more effective system creation, or in the case of translational research, safety benefits for human beings. The subsequent sections of this paper outline translational approaches for examining older driver performance and identifying potential countermeasures for mitigating crash risk of at risk drivers.
Neurological Aspects Associated with Increased Crash Risk – Understanding the Mechanisms of Failure
At a basic level, paper and pencil neuropsychological tests can provide a window into the specific cognitive deficits present in individuals with increased crash risk. Such testing is typically sensitive to gross abnormalities and is often treated as the gold-standard for assessing cognitive deficits in the clinic. Neuropsychological tests evaluate a range of functions including (a) visual-construction ability (judgment of line orientation (JLO), complex figure test copy version (CFT-Copy), WAIS- III block design (BLOCKS), (b) memory: complex figure test recall version (CFT-Recall), Benton visual retention test (BVRT), Rey auditory verbal learning test (AVLT) and (c) executive functioning: trail-making test (TMT-B), controlled oral word association (COWA) (see Strauss, Sherman, & Spreen, 2006). A number of studies have shown relationships between performance of at-risk drivers on paper and pencil tests of cognitive function and driving behavior both in on-road driving (e.g., Dawson, Anderson, Uc, Dastrup, & Rizzo, 2009) and simulated driving (Rizzo, Reinach, McGehee, & Dawson, 1997; Szlyk, Myers, Zhang, Wetzel, & Shapiro, 2002).
Neuroergonomic approaches can help map neurocognitive deficits onto performance and behavior profiles in more complex tasks. For example, work from our laboratory has recently demonstrated that patients with Alzheimer’s disease (a neurodegenerative disorder caused by the destruction of brain cells and associated with progressive impairments in cognitive functions (notably memory) and related behavioral disturbances), show a wide range of deficits on paper and pencil tests of cognitive function, and performance on these tests can provide additional predictive value of driving performance beyond basic diagnosis alone (Dawson et al., 2009). Furthermore, neuropsychological testing has been shown to correlate with driving performance in healthy aging, with a number of studies showing the predictive value of neuropsychological test scores on driving behavior in advanced age (De Raedt & Ponjaert-Kristoffersen, 2000; Szlyk, et al., 2002).
Despite the ability of certain neuropsychological tests to accurately predict driving performance, many of these tests correlate only weakly, if at all, with driving performance, especially in drivers with relatively subtle cognitive deficits (Bieliauskas, 2005; Bieliauskas, Roper, Trobe, Green, & Lacy, 1998). One reason for this is that paper and pencil tests represent relatively simple tasks in which the observer is under little performance pressure – they are often self-paced and low in overall processing demands. Given the heavy processing demands inherent in complex tasks such as driving, it is not surprising that many standard neuropsychological tests in domains known to influence driving performance (e.g., attention, working memory) nonetheless fail to correlate with driving behavior. This issue has been addressed in recent years by the introduction of complex computer-based tests designed to more accurately represent the heavy cognitive demands present during driving (Ball & Owsley, 1993a, 1993b; Edwards, et al., 2005).
One of these computer-based tests, the useful-field of view (UFOV), focuses on measures of attention and processing speed and has been successful in identifying at-risk drivers based on crash records (Goode, et al., 1998; Myers, Ball, Kalina, Roth, & Goode, 2000; Roenker, Cissell, Ball, Wadley, & Edwards, 2003). The standard UFOV test (see Edwards, et al., 2005) has several subtests, which increase in difficulty and attentional processing demands. By increasing task demands relative to paper and pencil testing, this computer based test begins to replicate the intense cognitive processing demands of driving in a laboratory setting – observers must quickly deploy attention to multiple regions of interest in the environment, select specific relevant items (i.e., targets) in the environment, while suppressing other, irrelevant items (“noise”). As a result, the predictive validity of one version of the UFOV task is high and has demonstrated a sensitivity of 89% and specificity of 81% for predicting crash involvement (Ball & Owsley, 1993a; Edwards, et al., 2005) especially crashes due to failure to yield at intersections (Owsley, et al., 1991).
Studies using the UFOV task have demonstrated deficits in attention function in at-risk drivers: When faced with a task that strongly engages attention, at-risk drivers are less able to extract visual information from the environment efficiently. In the context of driving, where individuals must rapidly shift attention to multiple locations to monitor hazards or information of interest (e.g., a pedestrian entering the intersection to their left, the flow of traffic to their right, and navigational landmarks), such a deficit in attention can undermine driving performance and safety. While this task provides a useful measure for identifying at-risk drivers, mechanistically speaking it does little to pinpoint which aspects of attention function are central to driving. “Attention” is not a unitary construct, but refers to a collection of processes that allow an observer to shift the focus of processing in time and space, control the breadth of information processing, select relevant information, and suppress irrelevant information (see Knudsen, 2007; Posner & Cohen, 1984). Since each of these processes has been associated with different underlying neural systems (see Fan, McCandliss, Sommer, Raz, & Posner, 2002), it is possible that there are selective deficits in some, but not other subcomponents of attention in at-risk drivers, and these deficits may play out in different ways on the road.
Using attention deficits in otherwise healthy older adults as a starting point, we have recently attempted to assess what specific mechanisms are linked with attention functions responsible for impaired performance on the UFOV task (Cosman, Lees, Vecera, Lee, & Rizzo, Submitted). To this end, we employed well established computer-based cognitive science paradigms known to tap major subcomponents of attention. We classified 54 drivers aged 65–87 as either impaired or unimpaired based on their UFOV performance. Following classification, drivers performed a visual search task in which they must find a target item embedded in an array of distracters. The task measures the ability to voluntarily shift attention in space in the presence of distracting information. The drivers also performed an attentional cueing task which measures the efficiency of stimulus-driven attentional orienting and shifting in the absence of distracting information (Posner, Snyder, & Davidson, 1980). Since the UFOV task is multifaceted, and requires the ability of participants to rapidly shift attention between aspects of the stimulus array in both the presence and absence of visual noise, these tasks are well suited for elucidating the underlying impairments in basic attention function present in attention-impaired individuals.
Figure 3 summarizes our results. In the visual search task, attention-impaired and unimpaired drivers performed equally on an “easy” feature search task – in which the target differed from the distracter items with respect to a specific, salient feature causing the target to “pop out” from the distracter items. This indicates that both groups of drivers were able to orient attention reflexively to salient features of the environment when those features “capture” attention. However, UFOV-impaired drivers performed significantly slower than unimpaired drivers in a more difficult conjunction search task in which the target was very similar to distracter items. In this case, drivers must voluntarily shift attention from item to item in a more or less serial fashion. This result indicates a possible deficit in the ability of attention-impaired drivers to voluntarily shift attention in space. Data from the cueing task supported such an interpretation; both attention-impaired and unimpaired drivers showed normal, reflexive orienting to the exogenous cue, as evidenced by the facilitory effect of the valid cue on reaction times. However, as can be seen in Figure 3b, attention-impaired drivers were slower to disengage attention from an invalidly cued location when the target was presented at the opposite location. In the context of the results from the difficult conjunction search task, this slower disengagement of attention may have been responsible for their slower search – when forced to search serially in the difficult conjunction search task, shifting attention between each item in the array took longer and slowed their search for the target.
Figure 3.

(a) Data from the visual search task for both useful field of view (UFOV)-impaired and unimpaired drivers. UFOV-impaired drivers searched more slowly for a target item in the difficult conjunction search task. (b) Data from the Posner cueing task. Of note are the disproportionately long reaction times on invalid trials for UFOV-impaired drivers, reflecting a decrease in their ability to “disengage” attention from the invalidly cued location.
Taken together our results demonstrate that UFOV impairment, and most likely their associated driving impairments, arise in part from deficits in the ability of these individuals to shift attention. More specifically, these individuals show decrements in the ability to disengage attention from currently attended objects or locations. In the context of driving, such impairment could lead to a number of problems associated with unsafe driving; since a UFOV-impaired driver is less efficient at shifting attention within the driving environment, the driver is likely to attend to fewer objects, fail to shift attention to highly critical objects and may miss major events that demand action. Normal drivers may attempt to search the environment more exhaustively to avoid missing critical objects and events that require action, but these impaired drivers do not. Their behavior fits well with descriptions of cases in which impaired drivers “look at but don’t see” critical roadway events such as an incurring vehicle at an intersection (Rizzo, McGehee, Dawson, & Anderson, 2001).
This study shows that an at risk population of drivers defined in terms of clinical (UFOV) impairment and epidemiological risk has a fundamental neurocognitive impairment of attentional disengagement that has the potential to disrupt human performance in context rich tasks such as automobile driving. The role of these and related mechanisms can then be addressed in drivers by adding layers of the driving context using CB, HP paradigms, interactive simulation in virtual environments and naturalistic settings under varying degrees of experimental control.
Using a Driving Context to Understand the Errors Drivers Make in the Real World
As mentioned previously, older drivers are over-represented in intersection crashes (McGwin & Brown, 1999; NHTSA, 2009; Preusser, et al., 1998; Zhang, et al., 1998). These drivers are often involved in crashes that include a failure to yield the right of way, unseen objects, or a failure to heed stop signs: errors that might be indicative of perceptual problems, attentional failures, or recognition problems (McGwin & Brown, 1999). The CB phenomenon seems particularly relevant to such crashes. CB refers to an inability to detect large changes in a visual scene, often associated with a visual disruption, such as an eye-movement, blink, or film cut (McCarley, et al., 2004; O’Regan, Rensink, & Clark, 1999; Pringle, Irwin, Kramer, & Atchley, 2001; Rizzo, et al., 2009). An example CB image is presented in Figure 4a in which the driver is required to notice the vehicle on the far left disappearing over time. While different methods are employed to simulate visual disruption, often changes are made to a static image. Noticing scene changes requires attention and visual working memory so that visual information before and after the change occurs can be stored and compared (Pringle, Irwin, Kramer, & Atchley, 2001; Simons & Ambinder, 2005). The difficulty of such tasks often depends on eccentricity, meaningfulness, and salience of the changing object (Pringle, et al., 2001). Research suggests that older adults, especially those with neurological disorders, are slower and less accurate when performing CB tasks compared to younger adults (Caird, Edwards, Creaser, & Horrey, 2005; Pringle, et al., 2001; Rensink, 2002; Rizzo, et al., 2009)
Figure 4.

(a) Change blindness task used by Rizzo et al. (2009) and Lees et al. (2007). The changes occurred over time with the change element being modified to either appear, disappear, change color or change location. However, changes were made to a static image. In contrast, (b) Hazard perception task in which the driver is asked to view filmed traffic situations and indicate when a hazard appears. Both tasks represent closed feedback in that the driver cannot influence the environment, but the hazard perception task has a broader focus and considers the temporal aspect of driving.
The benefit of such tasks is that they can incorporate high levels of scene complexity representative of the scenes that confront drivers, and can contribute to a deeper understanding of crash involvement by older drivers. For example, Caird et al. (2005) examined decision-making accuracy at intersections in young, middle-aged, young-old and old-old drivers using a modified CB task. During the task, drivers viewed 36 intersection scenes and were asked whether it was safe to travel in a particular direction (straight, turn left, or turn right), what had motivated their decision, what changes had occurred to the scene, and their level of confidence in the decision they made. After being provided with a direction arrow, intersection scenes were previewed for either 5 or 8 s alternating between the original image, a mask, and an altered image. For catch trials there was no change made to the original scene. Older drivers (young-old drivers aged 65–73 and old-old drivers aged 74 and over) were less accurate – incorrectly indicated it was safe to go –compared to middle-aged and younger drivers. Visual acuity and contrast sensitivity, object size and contrast did not account for differences in performance. The authors further examined differences using logistic regression and by examining differences in performance qualitatively. Age was a significant predictor of decision accuracy in 10 of the 36 intersections. Overall older drivers had more difficulty making turn decisions when required to detect pedestrian events and traffic sign changes, and the authors noted that older drivers may have been overly reliant on traffic control devices when making decisions about whether they could proceed.
Rizzo et al. (2009) examined CB performance as a function of age and found that as age increased the hit rate decreased, reaction times increased and sensitivity (d′) decreased. Examining CB across the various age groups, the study found that CB performance decrements became accelerated at certain ages; 54 years for hit rate and 68 years for both RT and d′. In addition, comparisons between older adults with and without Alzheimer’s disease suggest that declines in overall cognitive function (attention, short-term visual memory, and executive function tasks) correlated with worse CB performance. The results of these studies suggest that older drivers with and without neurocognitive disease may be less able to perceive visual changes. Such degradations in performance likely transfer to driving situations where drivers need to identify and respond to changes in their every day environment in order to avoid being involved in an accident.
In a follow-up study the authors examined the underlying features of two attention related tasks, CB and UFOV, in relation to commonly used vision and cognitive test batteries, and driving performance measures assessed using a simulator and an instrumented vehicle that measured real world driver behavior (Lees, Sparks, Lee, & Rizzo, 2007). Driving performance was evaluated using simulated driving events (a police car located on the side of the road and a vehicle that ran a stop sign) and during an on-road drive where drivers were asked to perform a route following task and a landmark and traffic sign identification task (see Uc, Rizzo, & Anderson, 2005; Uc, Rizzo, Anderson, Shi, & Dawson, 2004). Seventeen elderly individuals participated in the study, eight with early AD (74 – 81 years, M = 77.5) and nine without (64 – 73 years, M = 68.3). As shown in Table 1, three factors (attention and decision-making, detection and evaluation, and identification and intervention) were identified using a factor analysis that accounted for 57% of the variation across measures. While UFOV correlated with CB hit rate (R2=-.668, p<.01) and CB detection time (R2=.578, p=.015), the two tasks loaded on different factors.
Table 1.
Factor analysis of cognitive/visual tests, and driving performance measures
| Factor 1: Attention and Decision-Making (33%) | Factor 2: Hazard Detection and Evaluation (13%) | Factor 3: Identification and Intervention (12%) | |
|---|---|---|---|
| Attention | UFOV2 (.657) | CB2 -Response time (.756), z-score (−.649) | |
| Decision Making | COWA3 (−.449) TMT-B 3 (.804) RFT1: times lost (.716) wrong turns (.704), |
||
| Memory | BVRT3 (.624) AVLT 3 (−.543) |
||
| Visuoconstruction Ability | JLO (−.713) CFT-Recall3 (−.566) CFT-Copy3 (−.372) BLOCKS3 (−.870) |
||
| Vision | Visual acuity3 (.520) Contrast sensitivity3 (−.529) |
||
| Response Selection | RFT1 - at-fault errors (.826) LIT1 - at-fault errors (.667) Police Car1 – responded (.522) |
Crash at intersection1 (.604) Police car reaction time1 (−.626) |
|
| Identification | LIT task performance2-critical signs (.818), restaurants (.710) |
Driving Task;
CB/UFOV;
Visual/cognitive task
The findings suggest that UFOV relates to attention and decision-making, and CB relates to hazard detection and evaluation. These different underlying dimensions may account for the differing correlations of UFOV and CB with driving performance in the simulator and on the road. Specifically, UFOV demonstrated a general relationship to driving and correlated with a number of on-road performance measures. In contrast, the association between CB and driving seems to largely depend upon the specific images incorporated by the task and types of changes being detected. For example, the ability to correctly detect the appearance of a stop sign correlated with multiple on-road performance measures. The results suggest that CB and UFOV tasks may relate to different cognitive processes and different aspects of driving. Refined CB tasks may be particularly beneficial in understanding older driver failures and may complement information gained through other tasks.
HP tasks are another useful tool that might help identify at-risk drivers and help understand what broad mechanisms relate to driver safety. HP, the ability to recognize and anticipate hazardous roadway situations, is a critical driving related skill and correlates with accident involvement and driver experience (Horswill & McKenna, 2004; McKenna & Crick, 1994; Pelz & Krupat, 1974; Quimby & Watts, 1981). During HP tasks drivers are asked to watch filmed traffic clips and identify as quickly and accurately when they observe a potential hazard. As such, these types of tasks not only have high levels of visual realism but also a temporal component (see Figure 4b). In addition, these tasks offer increased experimental control because all drivers receive the same set of stimuli. Pelz and Krupat (1974) found that drivers without crashes or convictions responded 0.5 s faster compared to drivers with a crash history and 1.2 s faster than drivers with violations. Horswill and McKenna (2004) found drivers with more crashes had worse HP scores. Other researchers have found that novice drivers are less accurate and slower in perceiving hazards in filmed traffic situations compared to experienced drivers (Horswill & McKenna, 2004; McKenna & Crick, 1994). While the majority of studies examining HP ability have focused on inexperienced and young drivers, there is evidence that HP declines with age in drivers aged 65 and older (Horswill, et al., 2008). For example, in line with the age related trajectory of decline in CB associated with age (Rizzo et al., 2009) one cross-age study found that the ability to perceive hazards peaked at age 55 and then subsequently declined (Quimby & Watts, 1981). A recent study found that older drivers with diminished contrast sensitivity, larger reductions in the UFOV and slower simple reaction time performed worse when identifying and responding to filmed roadway hazards (Horswill, et al., 2008). In line with these findings, another study found that older drivers aged 75–84 were significantly slower in identifying hazards compared to both middle-aged drivers and older drivers aged 65–74 (Horswill, et al., 2009). Contrast sensitivity, simple reaction time measures, and UFOV were found to account for the difference between the different age groups.
The benefit of such tasks is that they offer the ability to incorporate the visual complexity representative of everyday driving not used in neuropsychological or computerized tasks and still allow high levels of experimental control that are not possible with on-road driving tasks or naturalistic data collection. Such tasks may be particularly useful in identifying at-risk older drivers. In addition, several studies have shown that exposing drivers to hazards or providing training regimes can improve HP ability in novice drivers (Fisher, Pollatsek, & Pradhan, 2006; Grayson & Sexton, 2002; McKenna & Crick, 1994; McKenna, Horswill, & Alexander, 2006). Such training might also benefit older drivers when refined appropriately.
Using a Car as a Diagnostic Device to Understand Driver Errors and Track Behavior
CB, HP, and interactive simulation can be used to make detailed measurements of performance and behavior in healthy and impaired drivers as well as to design and evaluate technology and displays to improve driver performance and safety. However, drivers may behave differently in the real world than might be expected based on their self-report of driving behavior, paper and pencil tests, or computerized tasks administered in the clinical laboratory (Reger, et al., 2004; Rizzo, Robinson, & Neale, 2007). Therefore, studies performed in operational settings can be of great value and quantitative recordings of drivers operating their own instrumented vehicles (IVs) over time in the real world can provide the gold standard of driver performance (Dingus, et al., 2006; Neale, Dingus, Klauer, Sudweeks, & Goodman, 2005).
IVs permit quantitative assessments of driver performance in the field, in a real car, under actual road conditions, and are not subject to the same type of human observer biases as standard road tests. Such tools allow researchers to examine objective indices of driving performance in normal and potentially unfit drivers (Uc, et al., 2004) and to assess the safety and usability of prototype automotive technologies evaluated in earlier stages using virtual environments and “off road” tasks. One ethical issue for use of IVs in research is ensuring privacy protections for drivers who agree to be studied, especially those who may be considered at greater risk and who therefore face greater scrutiny by licensing authorities. Another issue concerns how illegal driving behaviors or other activities are reported. Research involving IVs normally has a protocol for dealing with such events that is specified prior to enrollment in the study through an informed consent document.
Vehicle kinematic profiles in common roadway scenarios may provide specific evidence of driving safety problems in older drivers with age and disease-related declines in visual, cognitive, and attentional impairments that relate to overall driving safety and cognitive abilities. Several studies have documented an increased crash risk of older drivers at intersections, particularly those with a stop sign (McGwin & Brown, 1999; NHTSA, 2009; Preusser, et al., 1998; Zhang, et al., 1998). For example, one study reported that 700,000 police-reported crashes occur at stop signs every year (Retting, Weinstein, & Solomon, 2003). This is particularly problematic given the severity of such crashes. In one study, 70% of the crashes investigated that occurred at intersections with a two-way stop sign were attributed to stop sign violations (Retting, Weinstein, & Solomon, 2003). In cases where the driver had reported coming to a stop prior to entering the intersection 44% of drivers indicated they failed to notice the other vehicle.
Bao and Boyle (2008, 2009) evaluated driver performance in young, middle-aged and older drivers at two rural expressway intersections. Drivers were asked to maneuver straight across the intersection, make a left turn, and make a right turn at high and low crash intersections. Older and younger drivers demonstrated different braking profiles when compared to middle-aged drivers (Bao & Boyle, 2008). Compared to middle-aged drivers, younger and older drivers were less likely to come to a complete stop before entering an intersection, took more time to initiate a braking response, and took less time to reach maximum braking. Interestingly, drivers were less likely to come to a complete stop when turning left or right compared to when travelling across the intersection. In a follow-up, the authors examined visual scanning behavior of these drivers while performing different driving maneuvers at the two intersections (Bao & Boyle, 2009). Overall, the results of the study suggest that compared to middle-aged and younger drivers, older drivers spent a smaller proportion of time scanning to the left and right when approaching an intersection, when approaching a median, and when exiting an intersection. Older drivers also spent less time checking their rear-view mirrors suggesting that they limit their visual sampling to certain areas.
These problems are magnified in older drivers with neurodegenerative impairments such as Alzheimer’s disease (AD). Drivers with AD may have difficulty identifying traffic signs and landmarks and commit more at-fault safety errors compared to older drivers without AD (Dawson, et al., 2009; Rizzo, et al., 2004; Uc, et al., 2005; Uc, et al., 2004). Recently we evaluated if drivers with and without AD demonstrate different driving behavior when approaching stop signs during an on-road drive in an instrumented vehicle. Performance was evaluated at a four-way stop sign that required drivers to go straight and at a t-intersection where drivers made a right turn. 34 drivers with probable AD (ages 51–89, M = 74.3) and 158 neurologically normal drivers without AD (ages 52–74, M = 64.6) participated. Performance measures included (a) speed when stop sign first visible, (b) time when accelerator released, (c) time when brake released, (d) total brake duration (total time the brake was applied when approaching the stop sign), (e) transition time from brake to accelerator after full stop (see Figure 5), (f) number of brake pumps (times the brake was applied then released), (g) maximum brake position, and (h) number of head turns after stop.
Figure 5.

Demonstration of measures derived to determine driver response to stop sign over time.
The results suggest that the four-way stop and the t-intersection imposed different demands on drivers. Older drivers with and without AD had somewhat different braking profiles that varied according to the intersection. At the four-way stop drivers with AD had faster approach speeds (p = 0.071). Such differences might be due to the inability of drivers with AD to recognize the need to slow down. For example, one study found that compared to older drivers without AD, older drivers with AD had more difficulty recognizing traffic signs (Brashear, et al., 1998). While performance was dependent upon the sign, the study found that while 98% of normal drivers correctly identified a stop sign only 76% of drivers with AD were able to do so. At the t-intersection, drivers with AD also applied more brake pumps (p = 0.082) which may suggest an inability to identify how to modulate braking in relation to the upcoming stop sign. Drivers with AD made more head turns when deciding to enter the intersection at the four-way stop (p = 0.072) and took longer to reaccelerate after stopping at the t-intersection (p = 0.093). Such differences in performance may reflect increased search time and go/no-go decision making in these at-risk drivers with cognitive impairment. Overall, these field studies suggest behaviors that might contribute to intersection crashes involving older drivers with and without neurological impairment (Bao & Boyle, 2008, 2009) and provide rationale for developing and designing particular countermeasures.
Along these lines, research suggests that older drivers with attention impairments may be more willing to attempt crossing a road under unsafe conditions compared to older drivers without impairments (Pietras, Shi, Lee, & Rizzo, 2006). Pietras et al. (2006) examined traffic entry behavior in older drivers with and without UFOV impairments. Drivers were asked to make judgments from a stationary vehicle about the last possible moment they could safely cross a road in the presence of an oncoming vehicle. In addition, they were asked to cross the roadway when no traffic was present. Speed and distance of oncoming vehicles were obtained using Light Detection And Ranging (LIDAR). The study found that older drivers with attention impairments accepted shorter time-to-contact values, took longer to cross the road, and had shorter safety margins compared to older drivers without impairments. UFOV scores negatively correlated with the three safety measures, suggesting that larger UFOV impairments are associated with more risky intersection-crossing behavior. Using a Monte-Carlo simulation, the study found that such differences in traffic-entry decisions increased the risk of a crash for impaired drivers by 6.9 times compared to unimpaired drivers when the approaching vehicle failed to brake and 17.0 times compared to unimpaired drivers when the approaching vehicle were to compensate for the situation.
Multiple studies have used instrumented vehicles in traffic safety research (e.g. Bao & Boyle, 2008, 2009; Dingus, et al., 1997; Rizzo, et al., 2004; Uc, et al., 2005; Uc, et al., 2004). In most cases an experimenter is present, and drivers who are aware of being observed are liable to drive in an overly cautious and unnatural manner. Because total data collection times are often less than an hour and crashes and serious safety errors are relatively uncommon, no study until recently has captured pre-crash or crash data for a police-reported crash. Internal networks of modern vehicles allow continuous detailed information from the driver’s own car over extended time frames (Rizzo, Jermeland, & Severson, 2002). Modern vehicles report variables relevant to speed, emissions controls, and vehicle performance, and some vehicles allow more detailed reporting options via the vehicle’s on-board diagnostics (OBD) port. Lane-tracking video can be processed to assess lane-keeping behavior. Radar systems in the vehicle can gather information on the proximity, following distance, and lane-merging behavior of the driver and other neighboring vehicles on the road (Pietras, et al., 2006). Global positioning systems (GPS) can show where and when a driver drives, takes risks, and commits errors. Cell phone use can be tracked without recording conversations to assess potential driver distraction and risk acceptance (i.e., choosing to be distracted). Wireless systems can check the instrumentation and send performance data to remote locations.
These developments can provide direct, real-time information on driver strategy, vehicle use, upkeep, drive lengths, route choices, and decisions to drive during inclement weather and high traffic. A person driving his or her own instrumented vehicle is exposed to the usual risk of the road environment without the psychological pressure that may be present when a driving evaluator is in the car. Road test conditions can vary depending on the weather, daylight, traffic, and driving course. This is an important advantage for naturalistic testing: Repeated observations in varying real-life settings provide rich information regarding driver risk acceptance, safety countermeasures, and adaptive behaviors.
Such information provides unique insights on the ranging relationships between low-frequency/high-severity driving errors and high-frequency/low-severity driver errors. Such “brain-in-the-wild” relationships (Rizzo, et al., 2007) were explored in detail in a study of naturalistic driving performance and safety errors in 100 normal individuals, driving 100 total driver years (Dingus, et al., 2006; Neale, et al., 2005). All enrolled drivers allowed installation of an instrumentation package into their own vehicle (78 cars) or drove a new model-year IV provided for their own use. Data collection provided almost 43,000 hours of actual driving data, over 2,000,000 vehicle miles. There were 69 crashes, 761 near crashes, and 8295 other incidents (including 5568 driver errors) for which data could be completely reduced (Klauer, Dingus, Neale, Sudweeks, & Ramsey, 2006). Crash severity varied, with 75% being mild impacts, such as when tires strike curbs or other obstacles.
Using such data collection procedures with at-risk drivers is likely to provide an abundance of knowledge and to provide the context of errors or lapses that result in crashes. Such data can also verify the assumptions of theoretical models and the results of laboratory studies regarding the role of variables such as how much time it takes drivers to react (Gabler & Hinch, 2009). As shown in Figure 6, event recorders allow vehicle data to be collected when severe steering or braking triggers such systems. The driver in this example had cognitive deficits that were documented in detail with neurocognitive testing and in virtual environment. By analyzing the quantitative data in context, researchers can better understand the factors surrounding a crash. For example, if a driver crashes with a vehicle while making a left turn, such data would allow researchers to see if the driver came to a stop, whether they looked to determine if it was safe to proceed, etc.
Figure 6.

An inattentive older driver of our instrumented vehicle (NIRVANA) approaches a lead vehicle (top panels) at more than over 30 mph (25 knots) and brakes hard (peak in the upper right plot) to avoid a rear-end collision. There is a corresponding dip in speed, as shown by the electronic data from the vehicle(lower panel). The severity of the braking triggered a DriveCam system to record the video of the event.
Naturalistic data also provides a small window into the social and cultural influences that guide drivers. Although such factors are rarely the proximal causes of crashes they may well represent a critical contribution to driving safety. Driving culture has an enormous influence on the driving safety of the population through its influence on norms and acceptable bounds for behavior and expected responses in a broad range of situations. Culture influences safety critical behavior such as seatbelt use, driving under the influence of alcohol, and speeding. In the case of seatbelt use and drinking and driving changes in social norms have saved thousands of lives (Moeckli & Lee, 2006). Although part of the broader culture, it can be useful to consider older drivers as having a distinct culture and how this culture is shaped could have critical consequences. If age-related cognitive decline becomes a stigma in the culture of older drivers then people may be inclined to persist in driving even when they recognize it is not safe. Naturalistic data that can be placed in the social context of driving might be particularly valuable in identifying the factors that influence drivers to drive in situations where crashes are likely. Understanding how such distal causes contribute to driving safety may identify novel interventions that might otherwise be overlooked.
Developing Crash Countermeasures with Particular Driver Populations in Mind
Knowing which specific cognitive functions are impaired in specific populations of at-risk drivers becomes important when considering the development of countermeasures to remediate attention deficits in at-risk populations – to the extent that the basic, underlying cognitive and neurological mechanisms of the cognitive dysfunction are known, specific countermeasures may be ethically employed to mitigate these deficits (Larriviere, Williams, Rizzo, & Bonnie, 2009). For example, in knowing exactly which specific brain networks are involved in a deficit, along with the pharmacological properties underlying that network’s physiology, it may be possible to suggest specific pharmacological interventions that act to counter the deficit. By the same token, peripersonal environmental countermeasures such as in-vehicle warning systems can be designed to more effectively exploit knowledge of specific cognitive deficits in order to increase alert efficacy. Alongside neuropsychological tests and complex computer-based tests of cognitive function, more specific computer-based tests based on cognitive psychology paradigms can provide a greater degree of assessment specificity and sensitivity, resulting in the ability to tailor countermeasures to specific populations of individuals with specific deficits (Weaver et al., 2009). Finally, crash statistics, on-road assessments and naturalistic data can provide information regarding what crashes certain drivers are over-represented in, what breakdowns occur and possibly lead to crash involvement.
Such information can dictate what types of countermeasures would be most beneficial to certain populations. For example, given the review provided here, the data strongly suggest that older drivers with and without impairments would benefit from a variety of countermeasures aimed at helping with intersection approach and negotiation. Such countermeasures might warn them of upcoming traffic signals or help drivers identify hazards that might otherwise be missed (i.e. speech warning that the driver is approaching a stop sign, visual warning highlighting the upcoming sign or crossing traffic), measures that invoke drivers to engage in certain behavior (i.e., LEDs placed on the side mirrors, rear view mirror, and window pane that increase the drivers scanning of an intersection), or systems that increase safety margins and gap acceptance (i.e., using sonification to indicate gap size).
Recent work in our laboratory has focused on the development and implementation of such countermeasures in at-risk drivers, and we have begun to assess the basic cognitive operations that are impaired in different driver populations. By employing computer-based psychological tasks that are sensitive to the specific components of high-level cognitive functions such as attention, we can adapt our countermeasures to better fit the needs of different populations of at risk drivers. Since there are most likely very different neurological origins of impaired driving performance between different groups of at-risk drivers, and different cognitive manifestations of these deficits, such specificity will allow for more effective remediation of driving difficulties across a range of driving-impaired individuals. For example, information regarding basic attention function in a population of at-risk drivers can provide a starting point for the design of a system capable of remediating specific attention deficits in UFOV-impaired older drivers.
Alerting drivers to specific driving situations is a promising approach in increasing a driver’s situation awareness and enhancing driving safety. Our findings suggest that older drivers with attention impairments might benefit from salient, directional alerts that reflexively draw attention to critical locations in the driving environment to overcome these subjects’ subtle deficits in voluntary attentional shifting (Cosman, et al., Submitted). In another study, we examined the effectiveness of cross-modal alerting for orienting attention to external targets using a variation of Posner’s orienting of attention paradigm (Lees, et al., 2009). The findings suggest that older drivers with and without UFOV impairments benefited most when provided with auditory and auditory/haptic cues. These results correspond with other research that has examined the benefit of using multimodal cues in more complex settings (i.e., using a simulator) (Ho, Reed, & Spence, 2006, 2007; Kramer, Cassavaugh, Horrey, Becic, & Mayhugh, 2007; Spence & Ho, 2008).
Auditory warnings that convey a specific meaning in addition to reflexive directional orienting of attention might further enhance driving safety. In general, a sound is processed through the sensory transduction of sound waves that enter the ear, and additional transmission leads to signals that are passed on to the brain (Lehto & Buck, 2008). There are three primary mechanisms that work together to perceive and recognize sounds: First of all, the peripheral auditory system detects sound waves that are further processed by the receptors and transmitted to the central auditory unit via action potentials. There they are decoded into audible sounds. Cognitive processes at the third level allow for the sound to be modified into meaning (Chisolm, Willott, & Lister, 2003). These three stages involve different anatomical areas: the perceptual stage involves the outer, middle and inner ear, the intermediate or central auditory unit includes neural nuclei in the brainstem, midbrain and thalamus and the final stage is located in the auditory cortex and other processing areas in the brain (Munkong & Juang, 2008).
Sounds might be particularly effective as warning signals because of advantages on several of these auditory processing stages. On the perceptual level, sounds are likely to attract attention regardless of a person’s workload (Edworthy, 1994). Moreover, many sounds are omnidirectional, which increases their likelihood of being detected (Haas & Edworthy, 2006) when compared to visual warnings. On the cognitive level, auditory icons (caricatures of natural sounds based on everyday experiences) have proven to be intuitive and quickly understood (Barrass & Kramer, 1999; Lucas, 1994; Petocz, Keller, & Stevens, 2008). These types of warnings have the potential to reduce cognitive processing effort which can thereby speed responses (Belz, Robinson, & Casali, 1999). Several laboratory and simulator studies have found that such warnings can reduce response times to visual stimuli (McKeown & Isherwood, 2007). However, this general benefit of auditory icons as warning signals might not apply to certain populations, such as young soldiers who have sensorineural hearing loss due to exposure to repetitive blast percussions, or older drivers, who might have more difficulties in identifying such sounds and mapping them appropriately to relevant hazards in the visually complex roadway panorama, especially when time is a factor. In addition, the ability of the human ear to be most sensible for frequencies between 500–3000 Hz (Deatherage, 1972) might be decreased as age related sensory degradation is associated with the reduced ability of hearing high-pitched sounds (Chisolm, et al., 2003). This might be a problem for warning sounds with a high fundamental frequency which is generally supposed to lead to high ratings of urgency (Haas & Edworthy, 2006). For these reasons, the applicability of auditory as warning signals for older drivers needs to be further investigated.
In one study, we therefore evaluated how ten older drivers between the ages of 66 and 77 paired a set of auditory warnings with 12 roadway scenes (Figure 7). During the study each warning sound was played while the driver viewed each of the 12 scenes. This procedure was repeated for nine auditory icons and five distracter sounds that were not directly related to any of the driving situations (e.g. sneeze sound) and presentation was randomized across drivers. A variety of sounds were evaluated, some more specific to items in certain scenes (e.g. bike bell, footsteps, jackhammer) than others (e.g., siren, crash). For each driving scene, drivers had to decide if and how the sound related to the situation. When the driver indicated the sound was related they were also asked to specify the item they associated with the sound or what they might expect to happen based on the sound.
Figure 7.

Static traffic scenes presented, from left to right and top to bottom: a) curve, b) traffic light, c) bus, d) speed sign, e) oncoming car, f) stop sign, g) lead vehicle braking highway, h) bike, i) construction, j) merge, k) crosswalk, l) lead vehicle braking city.
A number of patterns emerge from the data in Table 2. First, specific warnings (e.g., bike bell 1, footsteps1, and jackhammer) were highly effective for conveying information about certain situations. For example, when “bike bell 1” was used, 8/10 people correctly indicated that the warning corresponded to the bike in the scene and from these answers the median rating of the match was 4 (1=weak match, 5=strong match). In addition, people rarely associated this warning with other types of situations, such as a vehicle, or sign. This suggests that these warning sounds have a high degree of specificity. Second, not all auditory warnings are the same, even when they are trying to convey the same message. The experiment used two different versions of a bike bell warning and of a footsteps warning. In both cases, one version dominated the other. For example, 9/10 people associated “footsteps 1” with the pedestrians in the crosswalk compared to 4/10 people making the association when “footsteps 2” was played. A similar trend occurred for the image with pedestrians by the bus stop, suggesting that “footsteps 1” better conveys the presence of pedestrians since a higher number of people associated this with the picture, even though the match was only rated to be slightly higher for this sound (median=3). Third, people generalized ambiguous warnings to a variety of situations (e.g., siren, the car horn and the screeching tires). Some of the general warnings used also had a high association with specific situations. For example, 7/10 people associated the car horn sound with the oncoming car situation and the rating for the match was fairly high (median=4). Fourth, some situations weren’t matched with any of the warning sounds by some drivers. This finding could have two implications: 1) there was no appropriate warning sound that was used in this study; 2) some people don’t think that these situations require a warning.
Table 2.
The absolute frequency with which a particular auditory icon was associated with a given situation and the median value of the match (1= weak match, 5=strong match). Empty cells represent cases where no response occurred, light grey cells correspond to specific warnings and dark grey cells correspond to more general warnings. Distracter sounds are excluded.
| Situation (Y)
| |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Warning (X) | Bike | Crosswalk | Bus | Construction | Lead vehicle braking highway | Lead vehicle braking city | Merge | Curve | Traffic light | Stop sign | Speed sign | Oncoming car | Row sum (X) |
| Bike bell 1 | 8 (4) | 1 (5) | 1 (5) | 1 (3) | 1 (5) | 4 (5) | 16 | ||||||
| Bike bell 2 | 3 (2) | 0.5 (2.5) | 1 (2) | 1 (1) | 6 | ||||||||
| Footsteps 1 | 4 (3.5) | 9 (3) | 7 (3) | 3 (3) | 1 (4) | 2 (2.5) | 26 | ||||||
| Footsteps 2 | 3 (3) | 4 (3) | 2 (2) | 1 (5) | 1 (4) | 11 | |||||||
| Jackhammer | 1 (2) | 2 (3) | 9 (3) | 1 (1) | 2 (2) | 1 (4) | 1 (1) | 1 (2) | 18 | ||||
| Screeching tires | 1 (1) | 5 (2) | 4 (3.5) | 4 (3.5) | 2 (2.5) | 2 (3.5) | 2 (3.5) | 6 (3) | 5 (3) | 2 (3) | 3 (4) | 36 | |
| Crash | 2 (2) | 2 (3) | 2 (2.5) | 1 (3) | 1 (3) | 2 (3) | 2 (2.5) | 12 | |||||
| Siren | 3 (4) | 2 (5) | 4 (4.5) | 3 (4) | 3 (4) | 4 (3) | 2 (4.5) | 4 (3) | 6 (4) | 4 (4.5) | 3 (4) | 3 (4) | 41 |
| Car horn | 6 (3) | 4 (3) | 3 (4) | 2 (3) | 3 (3) | 4 (2) | 1 (1) | 1 (1) | 2 (4.5) | 1 (2) | 7 (4) | 34 | |
|
| |||||||||||||
| Column sum (Y) | 31 | 27 | 23 | 20 | 10 | 15 | 3 | 10 | 18 | 13 | 10 | 20 | |
Overall, empirical findings from this and other studies suggest that the “screeching tires” sound may be most suitable for an imminent collision situation (Fricke & Thuering, 2009; Graham, 1999; Ho, et al., 2007; Ho, et al., 2004) as well as situations involving stop signs, traffic lights, and construction. Drivers appear to associate this sound with the general action of needing to slow down. This warning seems to be applicable for a wide variety of warnings and even valuable for special populations such as elderly drivers. Such interventions need to be evaluated with the full range of techniques described in this article; spanning physiologic recordings, controlled laboratory tasks, driving simulators, and ultimately an assessment of how such devices affect people during their everyday driving.
Conclusions
Neuroergonomics provides a multidisciplinary translational approach that merges elements of neuroscience, cognitive psychology, human factors and ergonomics to study brain structure and function in everyday environments. Applied to the salient example of automobile driving, such an approach aims to understand performance and safety using multiple sources of evidence and is likely to yield a deeper understanding of cognition in the natural settings. Driving makes demands on multiple cognitive processes that are often studied in isolation and so presents a useful challenge in generalizing findings from controlled laboratory tasks to predict safety outcomes. Neurology, neuroscience, and cognitive psychology can be used to explain and understand the mechanisms of cognitive breakdown that might be associated with a specific subset of drivers. However, a more complete picture of the actual impairments that such a driver would experience in the real-world might come from examining this person in controlled laboratory studies to determine the level of cognitive impairment or to determine that certain functioning has been affected. Expanding the scope of investigation even further to interactive simulation or naturalistic data collection the researcher might further document the errors that the driver makes and to determine how well the driver can compensate given his or her impairment. Moving from the controlled laboratory tasks to simulators and ultimately naturalistic driving situations engages an increasingly board range of influences. In driving cultural and social influences might play a role that is as important as neurological influences. While this paper used a neuroergonomics approach to examine older drivers, such an approach is useful for investigating a variety of populations in a various environmental settings.
Acknowledgments
This research was sponsored by grants AG017177 and AG15071 and AG026027 from the National Institute of Aging, Washington, D.C.
Contributor Information
Monica N. Lees, University of Iowa, Iowa City
Joshua D. Cosman, University of Iowa, Iowa City
John D. Lee, University of Iowa, Iowa City
Matthew Rizzo, University of Iowa, Iowa City.
Nicola Fricke, Transportation Active Safety Institute, Indianapolis.
References
- Ball K, Owsley C. Identifying correlates of accident involvement for the older driver. Human Factors. 1993a;33(5):583–595. doi: 10.1177/001872089103300509. [DOI] [PubMed] [Google Scholar]
- Ball K, Owsley C. The useful field of view test: A new technique for evaluating age-related declines in visual function. Journal of the American Optometric Association. 1993b;64:71–79. [PubMed] [Google Scholar]
- Ball K, Vance DE, Edwards JD, Wadley VG. The aging brain. In: Rizzo M, Eslinger PJ, editors. Principles and Practice of Behavioral Neurology and Neuropsychology. Philadelphia, PA: Saunders; 2004. pp. 795–809. [Google Scholar]
- Bao S, Boyle LN. Driver Performance at Two-Way Stop-Controlled Intersections on Divided Highways. Transportation Research Record: Journal of the Transportation Research Board. 2008;2069:26–32. [Google Scholar]
- Bao S, Boyle LN. Age-related differences in visual scanning at median-divided highway intersections in rural areas. Accident Analysis & Prevention. 2009;41:146–152. doi: 10.1016/j.aap.2008.10.007. [DOI] [PubMed] [Google Scholar]
- Barrass S, Kramer G. Using sonification. Multimedia Systems. 1999;7(1):23–31. [Google Scholar]
- Belz SM, Robinson GS, Casali JG. A new class of auditory warning signals for complex systems: Auditory icons. Human Factors. 1999;41(4):608–618. doi: 10.1518/001872099779656734. [DOI] [PubMed] [Google Scholar]
- Bieliauskas LA. Neuropsychological assessment of geriatric driving competence. Brain Injury. 2005;19:221–226. doi: 10.1080/02699050400017213. [DOI] [PubMed] [Google Scholar]
- Bieliauskas LA, Roper BR, Trobe J, Green P, Lacy M. Cognitive measures, driving safety, and Alzheimer’s disease. Clinical Neuropsychologist. 1998;12:206–212. [Google Scholar]
- Boyle LN, Tippin J, Paul A, Rizzo M. Driver Performance in the Moments Surrounding a Microsleep. Transportation Research Part F, Traffic Psychology and Behavior. 2008;11(2):126–136. doi: 10.1016/j.trf.2007.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brashear A, Unverzagt FW, Kuhn ER, Glazier BS, Farlow MR, Perkins AJ, et al. Impaired traffic sign recognition in drivers with dementia. American Journal of Alzheimer’s Disease and other Dementias. 1998;13(131):131–137. [Google Scholar]
- Calhoun V, McGinty V, Pekar J, Watson T, Pearlson G. Investigation of Marinol (THC) Effects upon fMRI Activation During Active and Passive Driving Using Independent Component Analysis and SPM. NeuroImage. 2001;13(6):S388. [Google Scholar]
- Calhoun V, McGinty V, Watson T, Pearlson G. Insights Into Functional Connectivity During A Driving Simulation Before And After Effects Of Marinol Intoxication On FMRI Activation And Cognitive Performance. Paper presented at the ACNP; Puerto Rico. 2000. [Google Scholar]
- Chisolm T, Willott J, Lister J. The aging auditory system: anatomic and physiologic changes and implications for rehabilitation. International Journal of Audiology. 2003;42(2):S3–2SI0. [PubMed] [Google Scholar]
- Cosman JD, Lees MN, Vecera SP, Lee JD, Rizzo M. Inefficient attentional shifting drives age-related impairments in the useful field of view Submitted. [Google Scholar]
- Dawson J, Anderson SW, Uc EY, Dastrup E, Rizzo M. Predictors of driving safety in early Alzheimer disease. Neurology. 2009;72:521–527. doi: 10.1212/01.wnl.0000341931.35870.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Raedt R, Ponjaert-Kristoffersen I. The relationship between cognitive/neuropsychological factors and car driving performance in older adults. Journal of the American Geriatrics Society. 2000;48:1664–1668. doi: 10.1111/j.1532-5415.2000.tb03880.x. [DOI] [PubMed] [Google Scholar]
- Deatherage BH. Auditory and other sensory forms of information presentation. In: Cott HPV, Kincade RG, editors. Human engineering guide to equipment design. Washington, DC: U.S. Government Printing Office; 1972. [Google Scholar]
- Dewar RE. Age differences - Drivers old and young. In: Dewar RE, Olson PL, editors. Human Factors in Traffic Safety. 2. Tucson, AZ: Laywers and Judges Publishing Company, Inc; 2007. pp. 143–158. [Google Scholar]
- Dingus T, Hulse M, Mollenhauer MA, Fleishman RN, McGehee DV, Manakkal N. Effects of age, system experience, and navigation technique on driving with an advanced traveler information system. Human Factors. 1997;39(2):177–199. doi: 10.1518/001872097778543804. [DOI] [PubMed] [Google Scholar]
- Dingus T, Klauer SG, Neale VL, Petersen A, Lee SE, Sudweeks J, et al. The 100-Car Naturalistic Driving Study, Phase II – Results of the 100-Car Field Experiment (No. DOT HS 810 593) Blacksburg, Virginia: Virginia Tech Transportation Institute; 2006. [Google Scholar]
- Edwards JD, Vance DE, Wadley VG, Cissell GM, Roenker DL, Ball K. Reliability and validity of useful field of view test scores as administered by a personal computer. Journal of Clinical and Experimental Neuropsychology. 2005;27:529–543. doi: 10.1080/13803390490515432. [DOI] [PubMed] [Google Scholar]
- Edworthy J. The design and implementation of nonverbal auditory warnings. Applied Ergnomics. 1994;25(4):202–210. doi: 10.1016/0003-6870(94)90001-9. [DOI] [PubMed] [Google Scholar]
- Evans L. Traffic Safety. Bloomfield Hills, Michigan: Science Serving Society; 2004. [Google Scholar]
- Fan J, McCandliss BD, Sommer T, Raz A, Posner MI. Testing the efficiency and independence of attentional networks. Journal of Cognitive Neuroscience. 2002;40:340–347. doi: 10.1162/089892902317361886. [DOI] [PubMed] [Google Scholar]
- Filley CM. Encephalopathies. In: Rizzo M, Eslinger PJ, editors. Principles and Practice of Behavioral Neurology and Neuropsychology. Philadelphia, PA: Saunders; 2004. pp. 635–653. [Google Scholar]
- Fricke N, Thuering M. Complementary audio-visual collision warnings. Paper presented at the Human Factors and Ergonomics Society 53rd Annual Meeting; San Antonio. 2009. [Google Scholar]
- Gabler HC, Hinch J. Feasibility of using event data recorders to characterize the pre-crash behavior of drivers in rear-end collisions. Paper presented at the Twenty-first International Conference on Enhanced Safety of Vehicles; Stuttgart, Germany. 2009. [Google Scholar]
- Graham R. Use of auditory icons as emergency warnings: evaluation within a vehicle collision avoidance application. Ergonomics. 1999;42(9):1233–1248. doi: 10.1080/001401399185108. [DOI] [PubMed] [Google Scholar]
- Graydon FX, Young RA, Benton MD, Genik RJ, II, Posse S, Hsieh L, et al. Visual Event Detection During Simulated Driving: Identifying the Neural Correlates with Functional Neuroimaging. Transportation Research Part F: Traffic and Transport Psychology. 2005;7:271–286. [Google Scholar]
- Haas E, Edworthy J. An introduction to auditory warnings and alarms. In: Wogalter MS, editor. Handbook of Warnings. Mahwah: Lawrence Erlbaum Associates; 2006. pp. 189–198. [Google Scholar]
- Ho C, Reed N, Spence C. Assessing the effectiveness of “intuitive” vibrotactile warning signals in preventing front-to-rear-end collisions in a driving simulator. Accident Analysis & Prevention. 2006;38:988–996. doi: 10.1016/j.aap.2006.04.002. [DOI] [PubMed] [Google Scholar]
- Ho C, Reed N, Spence C. Multi-sensory in-car warning signals for collision avoidance. Human Factors. 2007;49:1107–1114. doi: 10.1518/001872007X249965. [DOI] [PubMed] [Google Scholar]
- Horswill MS, Marrington SA, McCullough CM, Wood J, Pachana NA, McWilliam J, et al. Older drivers’ hazard perception ability. Journal of Gerontology: Psychological Sciences. 2008;63:212–218. doi: 10.1093/geronb/63.4.p212. [DOI] [PubMed] [Google Scholar]
- Horswill MS, McKenna FP. Drivers’ hazard perception ability: Situation awareness on the road. In: Banbury S, Tremblay S, editors. A Cognitive Approach to Situation Awareness. Aldershot, UK: Ashgate; 2004. pp. 155–175. [Google Scholar]
- Horswill MS, Pachana NA, Wood J, Marrington SA, McWilliam J, McCullough CM. A comparison of the hazard perception ability of matched groups of healthy drivers aged 35 to 55, 65 to 74, and 75 to 84 years. Journal of International Neuropsychological Society. 2009;15:799–802. doi: 10.1017/S1355617709990312. [DOI] [PubMed] [Google Scholar]
- Keller PE, Stevens C. Meaning from environmental sounds: Types of signal-referent relations and their effect on recognizing auditory icons. Journal of Experimental Psychology: Applied. 2004;10(1):3–12. doi: 10.1037/1076-898X.10.1.3. [DOI] [PubMed] [Google Scholar]
- Klauer SG, Dingus TA, Neale VL, Sudweeks JD, Ramsey DJ. The Impact of Driver Inattention on Near-Crash/Crash Risk: An Analysis Using the 100-Car Naturalistic Driving Study Data (No. DOT HS 810 594) Washington, DC: National Highway Traffic Safety Administration; 2006. [Google Scholar]
- Knudsen EI. Fundamental components of attention. Annual Review of Neuroscience. 2007;30:57–78. doi: 10.1146/annurev.neuro.30.051606.094256. [DOI] [PubMed] [Google Scholar]
- Kramer AF, Cassavaugh N, Horrey WJ, Becic E, Mayhugh JL. Influence of age and proximity warning devices on collision avoidance in simulated driving. Human Factors. 2007;49(5):935–949. doi: 10.1518/001872007X230271. [DOI] [PubMed] [Google Scholar]
- Larriviere JD, Williams MA, Rizzo M, Bonnie J. Responding to requests from adult patients for neuroenhancements. Neurology. 2009;73:1406–1412. doi: 10.1212/WNL.0b013e3181beecfe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lees MN, Cosman JD, Lee JD, Vecera S, Jang M, Dawson JD, et al. Cross-modal alerts for orienting of attention in attention impaired drivers. Paper presented at the 17th World Congress on Ergonomics; Beijing, China. 2009. [Google Scholar]
- Lees MN, Sparks JD, Lee JD, Rizzo M. Change blindness, attention, and driving performance. Paper presented at the Proceedings of the International Driving Symposium on Human Factors in Driving Assessment, Training, and Vehicle Design; Portland, Oregon. 2007. [Google Scholar]
- Lehto MR, Buck JR. Introduction to human factors and ergonomics for engineers. New York: Lawrence Erlbaum Associates; 2008. [Google Scholar]
- Lucas PA. An evaluation of the communicative ability of auditory icons and earcons. Paper presented at the Second International Conference on Auditory Display ICAD ‘94; Santa Fe, New Mexico. 1994. [Google Scholar]
- Lyman S, Ferguson SA, Braver ER, Williams AF. Older driver involvements in police reported crashes and fatal crashes: trends and projections. Injury Prevention. 2002;8:116–120. doi: 10.1136/ip.8.2.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGarraugh G. Alarm characterization for continuous glucose monitors used as adjuncts to self-monitoring of blood glucose. Journal of Diabetes Science and Technology. 2010;4:41–48. doi: 10.1177/193229681000400106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGwin G, Brown DB. Characteristics of traffic crashes among young, middle- aged, and older drivers. Accident Analysis and Prevention. 1999;31(3):181–198. doi: 10.1016/s0001-4575(98)00061-x. [DOI] [PubMed] [Google Scholar]
- McGwin G, Owsley C, Ball K. Identifying crash involvement among older drivers: Agreement between self-report and state records. Accident Analysis and Prevention. 1998;30(6):781–791. doi: 10.1016/s0001-4575(98)00031-1. [DOI] [PubMed] [Google Scholar]
- McKenna FP, Crick J. Hazard perception in drivers: A methodology for testing and training (No. Contractor Report 313) Crowthorne, Berkshire: Transportation Research Laboratory: Department of Transport; 1994. [Google Scholar]
- McKeown D, Isherwood S. Mapping candidate within-vehicle auditory displays to their referents. Human Factors. 2007;49(4):417–428. doi: 10.1518/001872007X200067. [DOI] [PubMed] [Google Scholar]
- Moeckli J, Lee JD. The making of driving cultures. In: Kissinger JP, editor. Improving traffic safety culture in the United States: The journey forward. Washington, DC: AAA Foundation for Traffic Safety; 2006. pp. 59–76. [Google Scholar]
- Munkong R, Juang BH. Auditory perception and cognition. IEEE Signal Processing Magazine. 2008:98–117. [Google Scholar]
- Neale VL, Dingus TA, Klauer SG, Sudweeks J, Goodman MJ. An overview of the 100-car naturalistic study and findings. Paper presented at the International Technical Conference on Enhanced Safety of Vehicles.2005. [Google Scholar]
- NHTSA. Traffic safety facts: Traffic tech- technology transfer series (No. 380) Washington: National Highway Traffic Safety Administration; 2009. [Google Scholar]
- Owsley C, Ball K, Sloane ME, Roenker DL, Bruni JR. Visual/cognitive correlates of vehicle accidents in older drivers. Psychology and Aging. 1991;6:403–415. doi: 10.1037//0882-7974.6.3.403. [DOI] [PubMed] [Google Scholar]
- Parasuraman R. Neuroergonomics: Research and practice. Theoretical Issues in Ergonomics Science. 2003;5:5–20. [Google Scholar]
- Parasuraman R, Rizzo M. Neuroergonomics: the brain at work. New York: Oxford University Press; 2007. [Google Scholar]
- Peters F, Collette F, Degueldre C, Sterpenich V, Majerus S, Salmon E. The neural correlates of verbal short-term memory in Alzheimer’s disease: a fMRI study. Brain. 2009;132:1833–1846. doi: 10.1093/brain/awp075. [DOI] [PubMed] [Google Scholar]
- Petocz A, Keller PE, Stevens C. Auditory warnings, signal-referent relations and natural indicators: Re-thinking theory and application. Journal of Experimental Psychology: Applied. 2008;14:165–178. doi: 10.1037/1076-898X.14.2.165. [DOI] [PubMed] [Google Scholar]
- Pietras TA, Shi Q, Lee JD, Rizzo M. Traffic-entry behavior and crash risk for older drivers with impairment of selective attention. Perceptual and Motor Skills. 2006;102:632–644. doi: 10.2466/pms.102.3.632-644. [DOI] [PubMed] [Google Scholar]
- Posner MI, Cohen Y, editors. Components of visual orienting. 10. Hillsdale, NJ: Erlbaum; 1984. [Google Scholar]
- Posner MI, Snyder CR, Davidson BJ. Attention and the detection of signals. Journal of Experimental Psychology. 1980;109(2):160–174. [PubMed] [Google Scholar]
- Preusser DF, Williams AF, Ferguson SA, Ulmer RG, Weinstein HB. Fatal crash risk for older drivers at intersections. Accident Analysis and Prevention. 1998;30(2):151–159. doi: 10.1016/s0001-4575(97)00090-0. [DOI] [PubMed] [Google Scholar]
- Pringle HL, Irwin DE, Kramer AF, Atchley P. The role of attentional breadth in perceptual change detection. Psychological Bulletin and Review. 2001;8:89–95. doi: 10.3758/bf03196143. [DOI] [PubMed] [Google Scholar]
- Quimby AR, Watts GR. Human Factors and Driving Performance. Crowthorne: Transport and Road Research Laboratory; 1981. [Google Scholar]
- Reger MA, Welsh RK, Watson GS, Cholerton B, Baker LD, Craft S. The Relationship Between Neuropsychological Functioning and Driving Ability in Dementia: A Meta-Analysis. Neuropsychology. 2004;18:85–93. doi: 10.1037/0894-4105.18.1.85. [DOI] [PubMed] [Google Scholar]
- Retting RA, Weinstein HB, Solomon MG. Analysis of motor-vehicle crashes at stop signs in four U.S. cities. Journal of Safety Research. 2003;34:485–489. doi: 10.1016/j.jsr.2003.05.001. [DOI] [PubMed] [Google Scholar]
- Rizzo M, Jermeland J, Severson J. Instrumented Vehicles and Driving Simulators. Gerontechnology. 2002;1(4):291– 296. [Google Scholar]
- Rizzo M, Reinach S, McGehee D, Dawson J. Simulated car crashes and crash predictors in drivers with Alzheimer disease. Archives of Neurology. 1997;54:545–551. doi: 10.1001/archneur.1997.00550170027011. [DOI] [PubMed] [Google Scholar]
- Rizzo M, Robinson S, Neale V. The Brain in the Wild. In: Parasuraman R, Rizzo M, editors. Neuroergonomics: the brain at work. New York: Oxford University Press; 2007. pp. 113–128. [Google Scholar]
- Rizzo M, Sparks J, McEvoy S, Viamonte S, Kellison I, Vecera SP. Change blindness, aging and cognition. Journal of Clinical and Experimental Neuropsychology. 2009;31:245–256. doi: 10.1080/13803390802279668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rizzo M, Stierman L, Skaar N, Dawson JD, Anderson SW, Vecera SP. Effects of a controlled auditory-verbal distraction task on older driver vehicle control. Transportation Research Record. 2004;1865:1–6. [Google Scholar]
- Rorden C, Karnath H. Using human brain lesions to infer function: a relic from a past era in the fMRI age? Nature Reviews Neuroscience. 2004;5:813–819. doi: 10.1038/nrn1521. [DOI] [PubMed] [Google Scholar]
- Simons DJ, Ambinder MS. Change Blindness: Theory and Consequences. Current Directions in Psychological Science. 2005;14(1):44–48. [Google Scholar]
- Spence C, Ho C. Multisensory interface design for drivers: past, present and future. Ergonomics. 2008;51:65–70. doi: 10.1080/00140130701802759. [DOI] [PubMed] [Google Scholar]
- Strauss E, Sherman E, Spreen O. A compendium of neurpsychological tests. 3. New York: Oxford University Press; 2006. [Google Scholar]
- Summers MJ. Increased inattentional blindness in severe traumatic brain injury: evidence for reduced distractibility. Brain Injury. 2006;20(1):51–60. doi: 10.1080/02699050500309742. [DOI] [PubMed] [Google Scholar]
- Szlyk JP, Myers L, Zhang YX, Wetzel L, Shapiro R. Development and assessment of a neuropsychological battery to aid in predicting driving performance. Journal of Rehabilitation Research and Development. 2002;39:483–495. [PubMed] [Google Scholar]
- Tippin J, Rizzo M, Sparks JD, Boyle LN. Reduced Useful Field of View in Drivers with Obstructive Sleep Apnea Syndrome (OSAS) Sleep. 2007;30(Suppl):A187. [Google Scholar]
- Uc EY, Rizzo M. Driving and neurodegenerative diseases. Current Neurology and Neuroscience Reports. 2008;8:377–383. doi: 10.1007/s11910-008-0059-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uc EY, Rizzo M, Anderson SW. Driver landmark and traffic sign identification in early Alzheimer’s disease. Journal of Neurology, Neurosurgery and Psychiatry. 2005;76:764. doi: 10.1136/jnnp.2004.049338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uc EY, Rizzo M, Anderson SW, Shi Q, Dawson JD. Driver route-following and safety errors in early Alzheimer disease. Neurology. 2004;63(5):832–837. doi: 10.1212/01.wnl.0000139301.01177.35. [DOI] [PubMed] [Google Scholar]
- Zhang J, Fraser J, Lindsay J, Clarke K, Mao Y. Age-specific patterns of factors related to fatal motor vehicle traffic crashes: focus on young and elderly drivers. Public Health. 1998;112:289–295. doi: 10.1038/sj.ph.1900485. [DOI] [PubMed] [Google Scholar]