

Abstract
One of the unique contributions of the current study is a glimpse into the process by which counselors decide to try new innovations in their clinical work. Data were collected from 421 counseling staff from 71 outpatient treatment programs in 4 US regions. Using hierarchical linear modeling, results reveal that the propensity to adopt workshop-based interventions is facilitated by two important mechanisms (1) an innovative organization with creative leadership and (2) change-oriented staff attributes (i.e., seeking professional growth, efficacy, adaptability, and influence on others). Innovative leaders and a climate receptive to change also bolster the development of these change-oriented attributes. One implication of these findings is the cascading effect of leaders’ support of innovative thinking and action resulting in employees strengthening their own adaptive skills and carrying this innovative thinking into individual adoption.
Keywords: Innovation adoption, leadership, organizational climate, staff attributes, multilevel modeling
1. Introduction
Organizations experiencing rapid changes and increasing demands require programming approaches that are open to change (Bass & Riggio, 2006). The substance abuse treatment field is faced with multiple challenges including inconsistent funding and an emphasis on demonstrating treatment effectiveness (McLellan, Carise, & Kleber, 2003). In response to these changing pressures, the National Institute on Drug Abuse (2006) has made dissemination of research products to facilitate the adoption and implementation of evidence-based interventions a priority. While all programs are encouraged to incorporate evidence-based interventions into treatment curriculums, some programs are better at innovation adoption than others (Real & Poole, 2005; Schoenwald & Henggeler, 2003).
The current study focuses on the initial adoption of innovations for treatment improvement among substance abuse treatment counselors. Specifically, this study examines organizational attributes that promote or impede what has been described in the technology transfer literature as the “decision to use what was taught in training” (Klein & Knight, 2005; Simpson, 2002). Counselors who self-report utilizing strategies learned through training tend to also be more open to the use of evidence-based practices (EBPs) and find such interventions to be generally appealing for treatment improvement (Saldana, Chapman, Henggeler, & Rowland, 2007). Because trial use of new innovations is considered a vital stage in the process of moving practices into routine care (e.g., Klein & Knight, 2005, Rogers, 2003), it is important to explore mechanisms involved in planning and initial adoption of innovations.
Processes involved in the planning and initial adoption of innovations are described in the TCU Program Change Model (Flynn & Simpson, 2009; Simpson & Flynn, 2007; see Figure 1). These begin with exposure to potential innovations in workshop-based training sessions. Following training, the next crucial step is adoption of the intervention, which involves a decision to try the intervention and action on the part of the counselor to begin trial use. The implementation stage expands adoption of the innovation to regular use. Innovations that successfully progress through these stages tend to become integrated into standard “practice,” bringing about improvements in client care.
Figure 1.
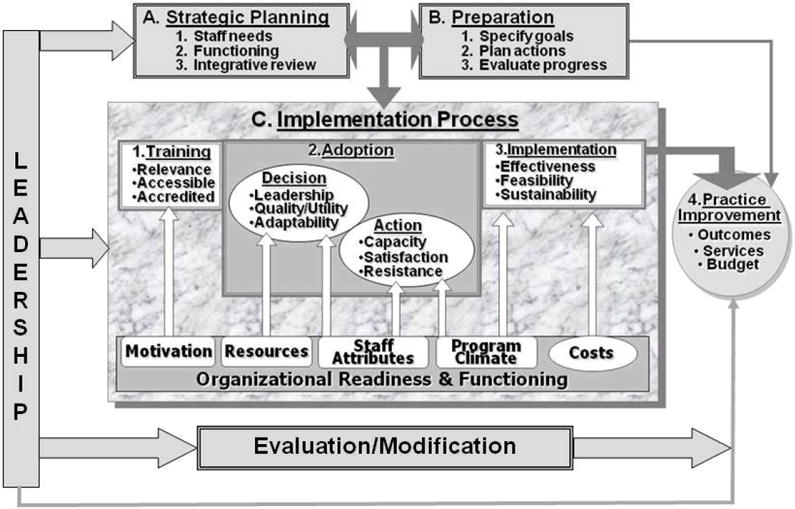
The TCU Program Change Model.
Permission granted from Original Sourceto reprint: Flynn, P. M., & Simpson, D. D. (2009).
Successful adoption of an innovation is heavily dependent upon program leadership, empowerment of staff members, and a climate that facilitates innovation (Flynn & Simpson, 2009; Simpson, 2002, 2009). As illustrated in Figure 1, a staff members’ decision to adopt a new innovation might be determined by a program leader, but it might also reflect the staff members’ individual decision to take action by trying the new innovation in their own clinical practices.
While leadership (Elenkov & Manev, 2009; Roman & Johnson, 2002), staff indicators of change (Farrell, Young, & Taxman, 2011; Joe, Broome, Simpson, & Rowan-Szal, 2007; Knudsen & Roman, 2004; Knudsen, Ducharme, Roman, & Link, 2005), and organizational climate (Fuller et al., 2007; Joe et al., 2007; Knudsen, Studts, Boyd, & Roman, 2010; Simpson, Joe, & Rowan-Szal, 2007) have independently been examined in relation to transferring research into practice, there is less known about how these mechanisms interact with each other to facilitate change.
The current study helps address this research gap by examining connections among several components of the TCU Program Change Model. Using advanced statistical techniques, specific hypotheses were examined, addressing how leadership influences innovation adoption through change-oriented staff attributes and exploring circumstances when leadership is more strongly related to change-orientation among staff members.
1.1. Staff attributes, leadership, and innovation adoption
Counselors’ perceptions of EBPs and willingness to try new innovations, especially those that impact the treatment process, are directly dependent upon individual attributes of counseling staff. For instance, having confidence in one’s counseling skills (i.e., work efficacy) builds persistence and initiation of behavior (Bandura, 1986) and can also develop heightened attitudes toward change (Schyns, 2004). Results from two studies suggest that staff attributes, as measured by the Organizational Readiness for Change (ORC) instrument, serve as indicators of how open a staff member is to change. Using a composite measure of staff attributes (e.g., adaptability, influence on others, professional growth, and work efficacy), Saldana et al. (2007) found that counselors reporting higher staff attributes are more open to using EBPs. Fuller et al. (2007) examined each staff attribute independently and found differential relationships depending on the specific attribute. Findings indicated that counselors who report more influence over others in their workplace and those that are adaptive to work demands also report more support for the use of manual based treatment innovations; whereas levels of confidence in one’s work and desire for professional growth were not related to attitude toward adoption of innovations. In consideration of these findings, the current study examines whether counselors that report change-oriented attributes (disaggregated as adaptability, influence on others, professional growth, and work efficacy) also report more trial use of new innovations introduced in workshops.
Hypothesis 1: Staff members that report more change-oriented attributes (i.e., adaptability, influence, growth, and efficacy) will also report more innovation adoption.
Leadership is also important in promoting change, particularly during times of insecurity (Conger & Kanungo, 1998; Donohue & Wong, 1994). For instance, employees report less cynicism toward organizational change when their leader is supportive of innovation (Bommer, Rich, & Rubin, 2005). Further, Aarons (2006) found that employees serving with leaders that support change report more acceptance of EBPs, openness to trying new interventions, and more perceptions of convergence between the current organizational practices and the EBP being considered for adoption. Based on these considerations, it is suggested that counselors employed in organizations where leaders facilitate organizational change will report more trial use of innovations introduced in workshops.
Hypothesis 2: Positive perceptions of leader practices will be associated with more innovation adoption.
Leader practices can also serve as one mechanism for promoting an open attitude to change among staff members. Leaders can help facilitate a change orientation by responding to staff members’ needs for achievement and professional growth, helping their staff to assert themselves, developing shared and aligned goals, and encouraging staff to become experts on the job. Such leader practices have been shown to strengthen followers’ confidence in their ability to successfully complete tasks (Bass, Avolio, Jung, & Berson, 2003) and may result in raising followers job efficacy (Schyns, 2004). Leaders that show concern for their staff members, lead by example, and encourage participatory decision making among staff, have also been shown to instill motivation among their staff to share their unique knowledge and ideas with others and actively participate in influencing other staff members in organizational decision making (Srivastava, Bartol, & Locke, 2006). Further, staff members in organizations with supportive leadership also report more opportunities for occupational training and development (Rowold & Laukamp, 2009). Based on these empirical findings, it is suggested that counselors employed in organizations where leaders facilitate organizational change will self-report more change-oriented staff attributes.
Hypothesis 3: Positive perceptions of leader practices will be associated with more change-oriented staff attributes.
Leaders that transform organizations by enabling staff members to more effectively deal with and respond to change, may cause a “cascading effect” across the hierarchical levels of the workplace, whereby leaders actions that promote change-orientation in staff members result in followers taking their own action to promote new initiatives(Avolio & Bass, 2004; Waldman & Yammarino, 1999). Thus a leader that models innovation not only stimulates receptivity for change in followers (Denton, Smith, Faust, & Holmboe, 2001), but also empowers staff to become change agents themselves. Leaders committed to the application of new techniques and to service improvement tend to instill a “capacity for evidence-based thinking” among their staff (Rosenberg, 2010). Therefore, while leader practices that transform organizations directly promote innovation, it is also possible that these same practices may indirectly result in innovation adoption through their influence on promoting change-oriented staff attributes. Reflecting this theoretical basis, it is hypothesized that leadership practices that transform organizations will promote trial use of new innovations by strengthening change-oriented attributes among staff.
Hypothesis 4: Change-oriented staff attributes will mediate the relationship between leader practices and innovation adoption, such that more positive perceptions of leader practices will be associated with more innovation adoption by increasing change-oriented staff attributes.
1.2. Organizational climate for change and innovation adoption
While positive leader behaviors can provide an impetus for staff attributes and actions, the influence that leaders have on outcomes can vary. Leaders and staff are inherently embedded within an organization, and therefore contextual characteristics such as perceptions of workplace practices and procedures influence individual decisions (McNulty, Oser, Johnson, Knudsen, & Roman, 2007), partially determining the impact that leadership has on an organization (Osborn, Hunt, & Jauch, 2002).
Counselors employed in high functioning drug treatment organizations – those that support open communication between management and staff and promote a certain level of freedom in getting tasks accomplished – are more likely to try new interventions received in training and to be satisfied with their use (Joe et al., 2007). While such organizational climates further the adoption of new innovations, which is important for promoting organizational improvement, programs within the treatment field vary significantly in the degree to which they exhibit innovative climates (Knight, Broome, Simpson, Edwards, & Flynn, 2007). If work groups vary significantly in the degree to which the climate supports change, then it would be anticipated that variations in climate might also influence how leader practices impact change-orientation among staff.
For instance, Wu, Neubert, and Yi (2007) examined organizational climate and found that group cohesion served as a moderator of leadership and cynicism toward change. Specifically, cohesive workgroups reported a stronger influence of leader practices on level of employee cynicism toward change. Simpson et al.(2007) also found that climate served as a “moderator” of the relationship between attitudes toward an innovation and trial use of the innovation. Regardless of how relevant and meaningful counselors’ viewed training materials, if the climate was not receptive to change, counselors had less motivation to try the new interventions in client care. Based on this theoretical and empirical framework, it is hypothesized that positive leader practices will be more influential in developing change-oriented attributes among staff in organizations with a climate for change.
Hypothesis 5: Organizational climate for change will moderate the relationship between leader practices and change-oriented staff attributes, such that the relationship between leader practices and change-oriented staff attributes will be stronger when there is a higher climate for change.
1.3. Methodological considerations
In addition to testing the specific hypotheses stated above, the current study offers several methodological advantages: (1) both program- and individual-level measures are examined and (2) multilevel modeling is used to account for variance associated with both program and individual measures simultaneously.
While it is essential that innovation adoption (i.e., outcome) and change-oriented staff attributes be assessed as individual perceptions, level of theory (theoretical consideration of constructs; Klein, Dansereau, & Hall, 1994) suggests that the measure of leadership and climate are best assessed as shared perceptions among counselors within the same program. In particular, individuals in a common group have similar perceptions of the values and guidance of their shared leader (Bliese, Halverson, & Schriesheim, 2002; Ehrhart, 2004; Gavin & Hofmann, 2002; Griffin & Mathieu, 1997) as well as corresponding views of common organizational practices and policies (James, 1982; Kozlowski & Hattrup, 1992). Therefore, individual staff ratings of leadership and climate are aggregated to serve as program means and are therefore assessed as Level-2 (group-level) predictors. The conceptual meaning takes into consideration individual staff attitudes about leadership and climate and aggregates the ratings into perceptions that staff hold of their leaders and organization as a whole. Conversely, individual ratings of change-oriented staff attributes and innovation adoption are assessed as Level-1 (individual-level) variables.
The current study inherently represents multilevel data, in that counselors are nested within a program and share a common leader. Research questions involving variability among respondents within naturally occurring groups require an analytical method that takes into account the multilevel structure of the data. The current study employed hierarchical linear modeling (HLM; Raudenbush & Bryk, 2002) that adopts a 2-level approach to evaluate the hypotheses.
Although HLM is similar to Ordinary Least Square (OLS) regression in parameter estimation (i.e., intercepts and slopes), HLM has two primary advantages over OLS regression, both dealing with the independence of the observations. First, OLS regression estimates one error term at the individual level of analysis, whereas HLM models estimate two error terms, (1) individual-level error and (2) group-level or residual error. Using OLS regression might provide a poor estimate of error variance when individuals within the same group score similarly with other members of their own group. Second, in OLS regression the degrees of freedom for group-level predictors are based on the number of individuals, whereas in HLM models the degrees of freedom are more appropriately based on the number of groups (see Gavin & Hofmann, 2002 for a conceptual and analytic overview of HLM models).
2. Method
2.1. Sample
As part of the Treatment Costs and Organizational Monitoring (TCOM) project, data were collected in 2004 from 92 Outpatient Drug-Free (ODF) treatment programs in 9 states: Florida, Idaho, Illinois, Louisiana, Ohio, Oregon, Texas, Washington, and Wisconsin. These data represent annual surveys of program structure, clinical staff, and clients. Programs were selected to reflect major types of ODF treatment for adults in several diverse geographic areas of the United States. Four Addiction Technology Transfer Centers (ATTCs; including the Southern Coast, Great Lakes, Gulf Coast, and Northwest Frontier) assisted with recruitment.
The study sample consists of 71 programs and 421 counseling staff that completed surveys on their treatment environment. Staff members from the remaining 21 of the 92 treatment programs were not considered in these analyses due to a low response rate with only one staff member completing the assessment. The group-level sample of 71 programs fulfills the suggestion that when using HLM – a minimum of 30 units be included in model estimation (Hofmann, 1997).
A majority of the programs (67%) were affiliated with a parent organization (i.e., shared financial responsibility with other programs); 37% of the programs were accredited by either the Joint Commission or the Commission on Accreditation of Rehabilitation Facilities (CARF); 72% were private-nonprofit with 18% private for profit and 10% public; and somewhat equally distributed in rural (25%), suburban (30%), and urban (45%) catchment areas. Case management was offered at 63% of the programs, 61% of the programs reported an increase in clients served from the previous year, and 39% reported a budget increase. On average, these programs served special populations which included 25% female clients, 30% clients referred from the criminal justice system, and 25% dual diagnosis (i.e., both mental health and substance abuse issues).
Counselors were predominately female (62%) and Caucasian(75%). Staff generally reported serving 3 or more years within the field of substance abuse treatment (75%) and 3 or more years within their current position (44%). The average age was 47 (SD = 11), and 42% of the staff reported a level of education at Master’s degree or higher. Typically, caseloads were diverse, with 21% having 10 or fewer clients, 47% having between 11 and 30, and 32% having more than 30 clients. A majority of the counselors (63%) were currently certified or licensed in the addiction field.
2.2. Procedure
Program directors and clinical staff were contacted and asked to complete a battery of organizational assessment forms. Program directors completed the Survey of Structure and Operations (SSO) addressing program information including program size, services offered, accreditation, affiliation with a parent organization, and proportion of special needs populations. Clinical staff members were asked to complete the staff versions of the Survey of Organizational Functioning (SOF), which includes the Organizational Readiness for Change (ORC; Lehman, Greener, & Simpson, 2002) instrument. All participation in the study was voluntary and the research protocols were approved by the university’s Institutional Review Board.
2.3. Measures
The current study utilizes four SOF primary measures, two that include multiple scales (staff attributes and climate) and two that are single scales (leadership and individual innovation adoption; Broome, Knight, Edwards & Flynn, 2009; Lehman et al., 2002). The rating scale for these items (with the exclusion of innovation adoption) ranged from 1 to 5 (1 = disagreestrongly and 5 = agreestrongly). Each item in the innovation adoption scale was rated using a similar 5-point Likert response format (1 = never, 2 = rarely, 3 = sometimes, 4 = a lot, 5 = almost always). All scale scores were recoded to range from 10 to 50.
2.3.1. Perceived program leadership
The leadership measure (Broome et al., 2009) is conceptually similar to constructs articulated by Bass, Avolio, and colleagues (Avolio, Bass, & Jung, 1999) and Podsakoff and colleagues (Podsakoff, MacKenzie, Moorman, & Fetter, 1990). Using a common stem referring to “My program director,” staff members were asked nine items about specific elements of their directors’ behavior. Items include “Leads by example,” “Encourages new ways of looking at how we do our jobs,” and “Provides well-defined performance goals and objectives”. The program leadership scale has shown good convergent validity with measures of job satisfaction and burnout and a reported coefficient alpha reliability of .90 (Broome et al., 2009).
2.3.2. Organizational climate for change
Organizational climate is represented by six scales (mission, cohesion, autonomy, communication, stress, and openness to change; Broome, Flynn, Knight, & Simpson, 2007). Mission includes “this program operates with clear goals and objectives” (5 items; coefficient alpha = .76). Cohesion among staff members includes “the staff here always work together as a team” (6 items; coefficient alpha = .82). Autonomy in decision-making includes “counselors here are given broad authority in treating their own clients” (5 items; coefficient alpha = .61). Open communication between staff and management includes “program staff are always kept well informed” (5 items; coefficient alpha = .79). Perceptions of stress includes “staff members often show signs of stress and strain” (4 items; coefficient alpha = .84). Openness to change includes “it is easy to change procedures here to meet new conditions” (5 items; coefficient alpha = .70). These six dimensions have been reported as highly intercorrelated (Greener, Joe, Simpson, Rowan-Szal, & Lehman, 2007; James & McIntyre, 1996) and were combined into a single, Organizational Climate Indexwith stress reverse coded (OCI; Greener et al., 2007). The OCI scale has shown good convergent validity with measures on attitudes toward adoption of evidence based practices (Saldana et al., 2007) and a reported coefficient alpha reliability of .87 (Broome et al., 2007).
2.3.3. Innovation adoption
As the primary dependent variable, innovation adoption consists of four items that address the counselors’ use of interventions from previous workshops, frequency of previous adoption, encouragement of other counselors to use ideas that the counselor has adopted, and responsiveness of the clients to newly adopted ideas and materials. The scale represents a general measure of adoption and is not linked to specific training opportunities or implementation initiatives. Items include, “In recent years, how often have you adopted (for regular use) new counseling interventions or techniques from a workshop?” and “When you attend workshops, how often do you try out the new interventions or techniques learned?” The innovation adoption scale has shown good convergent validity with measures on attitudes toward adoption of evidence based practices (Saldana et al., 2007) and a reported coefficient alpha reliability of .78 (Joe et al., 2007).
2.3.4. Change-oriented staff attributes
Four scales address staff attributes (i.e., growth, efficacy, influence, and adaptability). Each scale is analyzed independently and serves as a secondary dependent variable in the mediation analyses and as a primary dependent variable in the moderation analyses. Seeking professional growth includes items such as “keeping your counseling skills up-to-date is a priority for you” and “you regularly read professional journal articles or books on drug abuse treatment” (5 items; coefficient alpha = .78, Broome et al., 2007). Efficacy includes “you are effective and confident in doing your job” and “you have the skills needed to conduct effective group counseling” (5 items; coefficient alpha = .70, Broome et al., 2007). Influence on others includes “you often influence the decisions of other staff here” and “you are viewed as a leader by other staff here” (6 items; coefficient alpha = .80, Joe et al., 2007). Adaptability to a changing environment includes “you are willing to try new ideas even if some staff members are reluctant” and “you are able to adapt quickly when you have to shift focus” (4 items; coefficient alpha = .64, Joe et al., 2007). Measures of influence and adaptability have shown good convergent validity with opinions toward adoption of treatment manuals (Fuller et al., 2007).
2.3.5. Professional qualifications
Previous research has shown that professional qualifications, including years of experience within the treatment field, are related to innovation adoption and staff attributes (Saldana et al., 2007). Having a Master’s degree is related to higher ratings on the composite measure of staff attributes, while larger caseloads are associated with more innovation adoption. Reflecting these associations, the current study examined years in the treatment field (less than 1 year = 0, 1-3 years = 1, and more than 3 years = 2), education level (Master’s degree or higher), and caseload as potential covariates in analysis of innovation adoption and staff attributes. Including one or more covariates is a common method to increase the power in tests of effects (Kirk, 1998).
Caseload was measured using a categorical response format, where respondents selected the caseload size that most closely resembled their average client load. For the current analyses, these ranges are grouped into three categories: a ‘light’ caseload (10 or fewer clients), an ‘average’ caseload (11-30 clients), and a ‘heavy’ caseload (31 clients or more). Light caseload served as the reference category for analytic purposes. As an additional measure of counselor qualifications, certification within the treatment field was included as a covariate of innovation adoption and staff attributes. Years of experience, Master’s degree, caseload, and certification were obtained from the SOF instrument.
2.3.6. Program structure
Because attitudes toward innovation and change-oriented staff attributes are potentially connected with program structure, the current study includes two organizational measures (parent affiliation and accreditation) as covariates from the SSO. Parent organization affiliation was defined as belonging to a larger organization or agency of which the clinic or program is a part (with either shared or separate financial accounting practices). Accreditation by a national body (either Joint Commission or Commission on Accreditation of Rehabilitation Facilities (CARF)) was used to indicate ongoing quality assurance efforts. Fuller et al., (2007) reported that accredited programs were more likely to support adoption of medicated assisted treatment than non-accredited programs.
3. Results
3.1. Descriptive statistics and correlations
Means, standard deviations, intraclass correlation coefficients, internal reliabilities, and intercorrelations among the variables are reported in Table 1. All measures show high internal reliabilities, with alpha coefficients ranging between .67 and .92. The pattern of correlations provides initial support for the proposed relationships. Specifically, each staff attribute shows a statistically significant positive relationship with innovation adoption, leadership, and climate. Also, leadership relates positively to innovation adoption.
Table 1.
Descriptive Statistics and Intercorrelations among Study Variables
| M | SD | ICC | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Staff Levela | ||||||||||
| 1. IA | 33.29 | 7.15 | .15 | .81 | ||||||
| 2. GR | 35.70 | 7.12 | .17 | .35** | .74 | |||||
| 3. EF | 40.22 | 5.15 | .26 | .38** | .39** | .72 | ||||
| 4. AD | 37.78 | 5.58 | .06 | .33** | .37** | .49** | .67 | |||
| 5. IN | 35.75 | 6.66 | .10 | .44** | .37** | .32** | .28** | .81 | ||
| Program Levelb | ||||||||||
| 6. L | 37.92 | 4.05 | .21 | .21** | .37** | .18** | .14** | .21** | .92 | |
| 7. CL | 35.87 | 3.19 | .13 | .23** | .38** | .24** | .15** | .23* | .66** | .91 |
IA = Innovation Adoption, GR = Growth, EF = Efficacy, AD = Adaptability, IN = Influence, L = Leadership
CL = Climate, ICC = intraclass correlation
Note: The values on the diagonal shown in bold are the internal reliabilities.
N = 421
N = 71
p< .05;
p< .01
ICC values for both leadership (ICC = .21) and climate (ICC = .13) measures were high (> .10; Bliese, 2000; see Herold, Fedor, Caldwell, & Liu, 2008), indicating a significant influence of group membership on individual ratings and providing justification for modeling leadership and climate as Level-2 measures. The correlation coefficient between these two measures (r = .66) suggests that leadership and climate might be viewed by staff in a similiar manner. As anticipated the between-groups variance in the individual-level dependent variable (innovation adoption, ICC = .15) was high. Thus, there is evidence of group-level influences on the individual measure of innovation adoption. Likewise there is significant variance between programs in average ratings of 2 of the staff attributes. Whereas, professional growth and efficacy have high values (ICCs = .17 and .26 respectively), adaptability and influence have low ICC values (ICCs = .06 and .10 respectively), suggesting that there is relatively little variability between programs in individual ratings of adaptability and influence.
3.2. Test ofmediation effects
A series of two-level hierarchical linear models (HLM) were conducted using HLM 6.7 computer software (Raudenbush, Bryk, & Congdon, 2005). The strategy used in the current study to test mediation in HLM as suggested by Hofmann, Morgeson, and Gerras (2003) corresponds to the steps required to show mediation using standard regression (Baron & Kenny, 1986). Two direct effects were examined, (1) each staff attribute as it related to innovation adoption (Hypothesis 1; Models 1-4; see Table 2) and (2) leadership as it related to each staff attribute (Hypothesis 3; Models 6-9). One indirect effect was examined on leadership as it related to innovation adoption (Hypothesis 2; Model 5). Once the direct and indirect effects were considered(as the preconditions for mediation), Models 10-13 testing mediation were employed. A cross-level mediation effect (i.e., Level-1 predictor mediating a Level-2 predictor and a Level-1 outcome) is indicated when program level leadership is no longer significantly related to innovation adoption when simultaneously included in the model with a Level-1 staff attribute. When examining cross-level mediation effects (Hofmann & Gavin, 1998; Shanock & Eisenberger, 2006) it is advisable to grand-mean center the Level-1 predictors. Therefore, in the current study, Level-1 predictors were grand mean centered.
Table 2.
HLM Results for Test of Mediation
| Models | Coefficient (SE)
|
||||||
|---|---|---|---|---|---|---|---|
| Base Rate (γ00) | Leadership (γ01) | Staff Attribute (γ10) | Experience (γ20) | Master’s (γ30) | Certification (γ40) | Caseload (γ50) | |
| Hypothesis 1: Relationship of Staff | |||||||
| Attribute to Innovation Adoption | |||||||
| Model 1a: GR (γ10) | 33.46 (.39)** | -- | .34 (.05)** | 1.70 (.51)** | 2.12 (.64)** | .97 (.71) | 1.32 (.43)** |
| Model 2a: EF (γ10) | 33.30 (.39)** | -- | .41 (.08)** | 1.49 (.53)* | 1.45 (.66)* | 1.00 (.74) | 1.26 (.44)** |
| Model 3a: AD (γ10) | 33.40 (.40)** | -- | .40 (.09)** | 1.95 (.51)** | 2.05 (.65)** | 1.30 (.72) | 1.38 (.43)** |
| Model 4a: IN (γ10) | 33.18 (.40)** | -- | .40 (.05)** | 1.10 (.51)* | 1.82 (.65)** | .44 (.73) | 1.09 (.43)* |
| Hypothesis 2: Relationship of Leadership to Innovation Adoption | |||||||
| Model 5a | 33.32 (.43)** | .39 (.10)** | -- | 1.55 (.54)** | 2.28 (.68)** | 1.36 (.77) | 1.39 (.46)** |
| Hypothesis 3: Relationship of Leadership to Staff Attribute | |||||||
| Model 6: GR (Y) | 35.54 (.35)** | .65 (.09)** | -- | -- | -- | -- | -- |
| Model 7: EF (Y) | 40.40 (.36)** | .36 (.08)** | -- | -- | -- | -- | -- |
| Model 8: AD (Y) | 37.72 (.29)** | .25 (.07)* | -- | -- | -- | -- | -- |
| Model 9: IN (Y) | 35.9 (.37)** | .35 (.08)** | -- | -- | -- | -- | -- |
| Hypothesis 4: Mediation of Leadership-Innovation Adoption by Staff Attribute | |||||||
| Model 10a: GR (γ10) | 33.46 (.39)** | .14 (.09) | .32 (.06)** | 1.69 (.51)** | 2.12 (.64)** | 1.00 (.71) | 1.34 (.43)** |
| Model 11a: EF (γ10) | 33.29 (.38)** | .23 (.09)* | .38 (.08)** | 1.21 (.53)* | 1.48 (.66)* | 1.01 (.73) | 1.34 (.44)** |
| Model 12a: AD (γ10) | 33.35 (.39)** | .27 (.09)** | .39 (.06)** | 1.94 (.51)** | 2.01 (.64)** | 1.34 (.72) | 1.46 (.43)** |
| Model 13a: IN (γ10) | 33.20 (.39)** | .26 (.09)** | .37 (.05)** | 1.14 (.51)* | 1.77 (.64)** | .44 (.73) | 1.16 (.43)** |
GR = Growth, EF = Efficacy, AD = Adaptability, IN = Influence
Note: Y = outcome variable, γ00 = base rate of dependent measure
controlling for experience, Master’s degree, certification, and caseload
p< .05;
p< .01
Before examining the relationship between leadership, staff attributes and innovation adoption, the HLM analysis began with determining whether each measure of professional qualification served as a significant correlate of the primary independent variable (innovation adoption). Experience in the field, Master’s degree, certification, and caseload were each significantly related to innovation adoption and were subsequently included in all models predicting innovation adoption (Models 1-5, 10-13). With the exception of certification, each professional qualification was significantly related to innovation adoption in all models. Parent organization affiliation and program accreditation, as Level-2 measures, were not significantly related to innovation adoption and were therefore excluded from subsequent models with innovation adoption as the outcome variable.
Table 2 provides a summary of results from the hierarchical linear models used to test Hypotheses 1-4. Hypothesis 1 stated that staff members reporting more change-oriented attributes would also report more innovation adoption. HLM analyses revealed that all 4 staff attributes were related to innovation adoption (Growth: γ10 = .34, p< .01; Efficacy: γ10 = .41, p< .01; Adaptability: γ10 = .40, p< .01; and Influence: γ10 = .40, p< .01). Staff members who engage in professional growth activities, feel confident in their work, adapt to new work pressures, and who have a self reported influence on others are more likely to try innovations received in training. However, the relationship between influence and innovation adoption did not vary significantly between programs. Therefore the error term (u1) was dropped from the analyses, thereby “fixing” the relationship between influence and innovation adoption. Each staff attribute accounted for additional within-program variation in innovation adoption, beyond that explained by counselors’ professional qualifications (Growth: 15.1%, Efficacy: 8.7%, Adaptability: 11.5%, and Influence: 13.5%). As a result of grand mean centering the Level-1 variables, the intercept term or base rate, as reported in Table 2, represents the between group variance in innovation adoption after controlling for or partitioning out the effects of the Level-1 variables. Specifically in Model 1, on average, programs have innovation adoption ratings of 33.46 after controlling for professional growth, experience, Master’s degree, certification, and caseload.
Hypothesis 2 stated that positive perceptions of leader practices would be associated with more innovation adoption. HLM analysis revealed that program-level perceptions of leadership relate to individual measures of innovation adoption (γ01 = .39, p< .01). Staff members with leaders that are supportive of change are more likely to try innovations received in training. Leadership explained 32.3% of the between-program variation in innovation adoption, beyond that explained by counselor professional qualifications.
Hypothesis 3 stated that positive perceptions of leader practices would be associated with more change-oriented staff attributes. HLM analyses revealed that leadership at the program-level significantly relates to staff measures of professional growth (γ01 = .65, p< .01), efficacy (γ01 = .36, p< .01), adaptability (γ01 = .25, p< .05), and influence (γ01 = .35, p< .01). Based on these HLM results, Hypothesis 3 is supported. Because staff attributes were not the primary outcome variables in tests of mediation, the amount of between-group variability in staff attributes accounted for by leadership was not calculated at this stage.
Hypothesis 4 stated that change-oriented staff attributes would mediate the relationship between leader practices and innovation adoption, such that more positive perceptions of leader practices would be related to more innovation adoption by increasing change-oriented staff attributes. Given the results of Hypotheses 1-3, the preconditions for mediation were supported (Baron & Kenny, 1986). The final step in the test for mediation revealed that, when regressed onto innovation adoption simultaneously, both program-level leadership and staff-level efficacy remained significant (Leadership: γ01= .23, p< .05; Efficacy: γ10 = .38, p< .01). Similar results were found when influence (Leadership: γ01 = .26, p< .01; Influence: γ10 = .37, p< .01) and adaptability (Leadership: γ01 = .27, p< .01; Adaptability: γ10 = .39, p< .01) were examined as the staff-level measure. In the efficacy and professional qualifications model, leadership accounted for 10.8% of between-program variation in average innovation adoption ratings compared to 12.4% of between-program variation in the influence and professional qualifications model and 16.6% of between-program variation in the adaptability and professional qualifications model. However, when professional growth was examined as the staff attribute, growth served as a significant correlate of innovation adoption (γ10 = .32, p< .01), but program-level leadership was not significant (γ01 = .14, ns).
Based on these findings and the strategies suggested by Baron & Kenny (1986), the relationship between leadership and innovation adoption was fully mediated by professional growth. Specifically, once individual ratings of growth were controlled for, program-level perceptions of leadership were no longer significantly related to innovation adoption, suggesting that growth serves as a single, dominant mediator. Three of the four change-oriented staff attributes (i.e., efficacy, influence, and adaptability) served as partial mediators of the relationship between leadership and innovation adoption (Shanock & Eisenberger, 2006) because this relationship was still significant (even after controlling for staff attributes). The continued relationship suggests that there are multiple mediating factors operating on the relationship beyond that of efficacy, influence, or adaptability.
3.3. Test ofmoderator effects
An intercepts-as-outcomes model was used to examine the individual effects of climate and leadership on each of the staff attributes and to evaluate the moderating effects of climate on the leadership-staff attribute relationship (Herold et al., 2008). Both main effects and the interaction effect between leadership and climate were evaluated. Table 3 provides a summary of the hierarchical linear models and results used to test Hypothesis 5. Before conducting tests of moderator effects, just as with tests of mediation, the proportion of variance accounted for by professional qualifications was examined in relation to each staff attribute (as the primary dependent variables). Experience and certification within the field, as well as counselor education (i.e., a Master’s degree) were found to significantly relate to efficacy and influence; whereas they were not related to growth or adaptability. Caseload was not related to the staff attributes. Models evaluating efficacy and influence therefore included experience, Master’s degree, and certification as covariates (see Table 3, Models 15 and 17). In the moderation analyses, experience and Master’s degree were both related to influence and efficacy, while certification was only related to influence. Organizational structure was also considered in relation to each staff attribute. Parent organization affiliation and accreditation were not significantly associated with influence, efficacy, growth, or adaptability and were therefore not included as covariates in tests of moderation.
Table 3.
HLM Results for Test of Moderation
| Models | Coefficient (SE)
|
||||||
|---|---|---|---|---|---|---|---|
| Base Rate (γ00) | Leadership (γ01) | Climate (γ02) | L X CL (γ03) | Experience (γ10) | Master’s (γ20) | Certification (γ30) | |
| Hypothesis 5: Moderator Effect of Climate on Leadership-Staff Attribute | |||||||
| Model 14: GR (Y) | 35.43 (.37)** | .41 (.11)** | .65 (.17)** | .02 (.02) | -- | -- | -- |
| Model 15a: EF (Y) | 40.63 (.37)** | .18 (.11) | .30 (.15) | -.03 (.02) | 1.14 (.39)** | 2.04 (.49)** | .32 (.56) |
| Model 16: AD (Y) | 37.84 (.33)** | .18 (.10) | .13 (.14) | -.01 (.01) | -- | -- | -- |
| Model 17a: IN (Y) | 35.70 (.40)** | .21 (.12) | .41 (.17)* | .03 (.02) | 1.23 (.52)* | 1.37 (.64)* | 2.35 (.74)** |
GR = Growth, EF = Efficacy, AD = Adaptability, IN = Influence, L = Leadership, CL = Climate
Note: Y = outcome variable, γ00 = base rate of dependent measure
controlling for experience, Master’s degree, and certification
p< .05;
p< .01
HLM results suggest that the nuturing of change-oriented staff attributes depends in part on whether the organization has a climate receptive to change. When leadership and climate were added into the same model, climate remained significantly associated with influence (Leadership: γ01 = .21, ns; Climate: γ02 = .41, p< .05); however, leadership was no longer significant. These results suggest that staff self-ratings of influence are more heavily dependent upon program-level perceptions of climate than leadership. When professional growth served as the outcome, both leadership and climate remained significant (Leadership: γ01 = .41, p< .01; Climate: γ02 = .65, p< .01). Leadership and climate were not significant in relation to adaptability (Leadership: γ01 = .18, ns; Climate: γ02 = .13, ns) or efficacy (Leadership: γ01 = .18, ns; Climate: γ02 = .30, ns).
Leadership and climate reduced the intercept variance at the program-level by 70.3% in relation to influence beyond that explained by professional qualifications. In the model for growth, leadership and climate greatly reduced the variance between programs (95%) in individual growth ratings. No significant variance remained in average growth (T00 = .44, ns) once leadership and climate were accounted for.
More importantly, these analyses evaluated whether climate interacted with leadership in relation to staff attributes. Hypothesis 5, which stated that organizational climate for change would moderate the relationship between leader practices and change-oriented staff attributes, was not supported. In all four models, HLM results revealed no significant interaction effects of leadership and climate on efficacy (Leadership X Climate: γ03 = -.03, ns), influence (Leadership X Climate: γ03 = .03, ns), growth (Leadership X Climate: γ03 = .02, ns), or adaptability (Leadership X Climate: γ03 = -.01, ns). These results suggest that climate impacts the development of change-oriented staff attributes directly, rather than indirectly through an interaction with leadership.
4. Discussion
While adoption of new innovations may be initiated or mandated by leadership in order to improve clinical practice, the decision to actively use a new intervention in client care is often determined by the individual counselor. The main focus of this study is on “bottom-up adoption,” the degree to which individuals within an organization make a choice to try an innovation, not the degree to which leaders mandate change. This perspective diverges from leader driven change in relation to innovation adoption. Bottom-up adoption places the emphasis on how leaders foster personal staff commitment to innovation adoption. One of the unique contributions of the current study is a glimpse into the process by which staff members decide to try new innovations in their clinical work as facilitated by the combined effect of creative and engaged leaders and change-oriented staff attributes.
To summarize the findings, the propensity to adopt new interventions is facilitated by two important mechanisms (1) an innovative organization with creative leadership and (2) change-oriented thinking (staff attributes). Innovative leadership and a climate for change are linked with change-oriented attributes (i.e., efficacy, influence on others, professional growth, and adaptability). The current study further defines the process of individual adoption by showing that change-oriented attributes facilitate the impact that leadership has on change-oriented action (i.e., innovation adoption).
These findings extend the work of Saldana and colleagues (Saldana et al., 2007), by disaggregating the staff attributes into 4 components and examining how each independently relates to innovation adoption. All 4 of the change-oriented attributes (i.e., efficacy, professional growth, influence, and adaptability) were significantly related to counselors’ trial use of new innovations.
An additional contribution of this study is an empirical examination of the impact that leader practices have on followers (e.g., Aarons, 2006; Bass et al., 2003). Specifically, staff in programs with more positive perceptions of leadership, more frequently report adoption of new program practices and more self-perceived change-oriented attributes including efficacy on the job, influence on others, seeking of professional growth, and adaptability to a changing work environment.
Beyond these simple associations, the current study provides an indication of how each attribute interrelates with leader practices to influence individual adoption. The impact that leadership has on innovation adoption is in part connected with each staff attribute. Counselors’ perception of their leaders remains related to trying new interventions even when accounting for the relationship between efficacy, influence, and adaptability on innovation adoption. These findings suggest that strong positive leaders need to continue to instill confidence in their employees’ work, desire to influence organizational improvement, and adaptability to new work objectives in order to maximize innovation adoption among their counselors.
While there is a complex link between leadership and influence, efficacy, and adaptability, there is a single, strong connection between leadership and innovation adoption through perceptions of opportunities for professional growth. In fact, when the relationship between professional growth and innovation adoption is considered, leadership is no longer related to innovation adoption. This indicates that the affect that positive leader practices have on counselors’ decisions to try new interventions is largely related to staff members’ engaging in professional growth practices. Therefore leader actions, including support of new interventions and promotion of a clear and forward-thinking mission, instill in followers a propensity for “evidence-based thinking” (Rosenberg et al., 2010) and action.
One of the major implications for programming in the substance abuse treatment setting is the distinct possibility that leaders’ support of innovative thinking and action results in employees strengthening their own change-oriented skills (i.e., efficacy, influence on others, professional growth, and adaptability) and carrying this change-oriented thinking into action by trying new innovations in their clinical work. This “cascading effect” (Avolio & Bass, 2004; Waldman & Yammarino, 1999), illustrating that leader actions affect staff choices, helps to emphasize the importance of training leaders to be supportive of innovation and to building an environment that bolsters open thinking among staff members.
The current study also provides additional support for the impact that workplace practices and procedures have on the relationship between leadership and individual decisions (Osborn, et al., 2002). The findings suggest that when the climate is receptive to change and there is supportive and innovative leadership, counselors perceive more opportunities for professional growth than when the climate or leadership is less supportive of change. The moderator effect of organizational climate on the leadership-professional growth relationship was not supported, suggesting that the affect of leadership on seeking professional growth is not strengthened by program-level perceptions of organizational climate. Subsequently, positive leadership and an innovative climate (less stress and more emphasis on change and autonomy) can serve as exclusive motivators for staff to make professional self improvements.
Findings also suggest that self perceptions of influence on others are more closely connected to climate than leadership. Counselors working in environments with stronger climates for change report having more influence on others in their workplace. Whereas, regardless of whether the climate is viewed as being receptive to change or if there is innovative leadership, the counselors are equally likely to be adaptable to a changing work environment and to feel confident in completion of work tasks.
Simpson et al. (2007) suggests that climate strengthens the relationship between perceptions of an innovation and trial use, reflecting the “back end” of the individual innovation adoption process. The current study focuses on the “front end” of the change process and how climate interacts with the development of attitudes toward change. Organizational climate serves as one mechanism that is related to efficacy, propensity toward influencing coworkers, engaging in professional growth activities, and adaptability to a changing climate, all of which have been found in the current study to serve as correlates of innovation adoption. These findings, along with those of Simpson et al. (2007), collectively suggest that organizational climate underlies the entire process of innovation adoption, from the development of innovative thinking, to specific attitudes toward the innovation, and eventual adoption of new practices.
As in all studies, the methodology and analytic procedure include some limitations and highlight opportunities for further development. The study design is cross-sectional, with the measures collected at the same time point and within the same assessment. While a longitudinal design would enable interpretation of predictive relationships, the consistent nature of the findings with other studies (Fuller et al., 2007; Joe et al., 2007; Saldana et al., 2007) reinforces the interpretative relationships. Further, the sample represents 71 outpatient programs in 9 states; therefore generalizability of findings to residential settings may be limited.
While the current study contributes to an understanding of issues involved in moving research into practice, information on the types of evidence-based practices implemented by staff was unavailable. Future studies might consider how the packaging of evidence-based practices (e.g., disseminating mechanisms) interacts with innovative leadership, climate, and staffing. It might be possible that innovations designed as modularized treatment protocols (which offer counselors flexibility in matching treatment to clients’ needs while maintaining key elements of the intervention) might be more adoptable by counselors that engage in change-oriented staff attributes (i.e., professional growth, influence on others, and job efficacy) and who are employed in treatment programs with supportive and innovative leadership. Conversely, staff managed by top down, leader-driven change and those lacking change-oriented attributes might be more adept at trying new interventions or approaches packaged as structured manuals.
In summary, this study offers insight into the process of individual innovation adoption. Programs, funding agencies, and policy initiatives that promote leadership development training, facilitate a climate receptive to change, and foster innovative thinking among staff are better positioned to promote new ideas and action among clinicians.
Acknowledgments
The authors would like to thank the Gulf Coast, Great Lakes, Northwest Frontier, and South Coast Addiction Technology Transfer Centers (ATTCs) for their assistance with recruitment and training. We would also like to thank the individual programs (program leadership, counseling staff) that participated in the assessments and training in the TCOM Project.
This work was funded impart by the National Institute on Drug Abuse (Grants R01 DA014468, R01 DA013093). The interpretations and conclusions, however, do not necessarily represent the position of the NIDA, NIH, or Department of Health and Human Services. More information (including intervention manuals and data collection instruments that can be downloaded without charge) is available on the Internet at www.ibr.tcu.edu, and electronic mail can be sent to ibr@tcu.edu.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Aarons GA. Transformational and transactional leadership: Association with attitudes toward evidence based practice. Psychiatric Services. 2006;57:1162–1169. doi: 10.1176/appi.ps.57.8.1162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Avolio BJ, Bass BM. Multifactor Leadership Questionnaire: Manual and sampler set. 3. Menlo Park, CA: Mind Garden, Inc; 2004. [Google Scholar]
- Avolio BJ, Bass BM, Jung DI. Re-examining the components of transformational and transactional leadership using the Multifactor Leadership Questionnaire. Journal of Occupational and Organizational Psychology. 1999;72:441–462. [Google Scholar]
- Bandura A. The explanatory and predictive scope of self-efficacy theory. Journal of Social & Clinical Psychology. 1986;4:359–373. [Google Scholar]
- Baron R, Kenny D. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bass BM, Avolio BJ, Jung DI, Berson Y. Predicting unit performance by assessing transformational and transactional leadership. Journal of Applied Psychology. 2003;88:207–218. doi: 10.1037/0021-9010.88.2.207. [DOI] [PubMed] [Google Scholar]
- Bass BM, Riggio RE. Transformational leadership. Mahwah, NJ: L. Erlbaum Associates; 2006. [Google Scholar]
- Bliese PD. Within group agreement, non-independence, and reliability: Implications for data aggregation and analyses. In: Klein KJ, Kozlowski SWJ, editors. Multilevel theory, research, and methods in organizations: Foundations, extensions, and new directions. San Francisco: Jossey-Bass; 2000. pp. 349–381. [Google Scholar]
- Bliese P, Halverson R, Schriesheim C. Benchmarking multilevel methods in leadership: The articles, the model, and the data set. The Leadership Quarterly. 2002;13:3–14. [Google Scholar]
- Bommer W, Rich G, Rubin R. Changing attitudes about change: Longitudinal effects of transformational leader behavior on employee cynicism about organizational change. Journal of Organizational Behavior. 2005;26:733–753. [Google Scholar]
- Broome KM, Flynn PM, Knight DK, Simpson DD. Program structure, staff perceptions, and client engagement in treatment. Journal of Substance Abuse Treatment. 2007;33:149–158. doi: 10.1016/j.jsat.2006.12.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broome KM, Knight DK, Edwards JR, Flynn PM. Leadership, burnout, and job satisfaction in outpatient drug-free treatment programs. Journal of Substance Abuse Treatment. 2009;37:160–170. doi: 10.1016/j.jsat.2008.12.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conger JA, Kanungo RN. Charismatic leadership in organizations. Thousand Oaks, CA: Sage Publications; 1998. [Google Scholar]
- Denton G, Smith J, Faust J, Holmboe E. Comparing the efficacy of staff versus house staff instruction in an intervention to improve hypertension management. Academic Medicine. 2001;76:1257–1260. doi: 10.1097/00001888-200112000-00022. [DOI] [PubMed] [Google Scholar]
- Donohue KS, Wong L. Understanding and applying transformational leadership. Military Review. 1994;74:24–31. [Google Scholar]
- Ehrhart M. Leadership and procedural justice climate as antecedents of unit-level organizational citizenship behavior. Personnel Psychology. 2004;57:61–94. [Google Scholar]
- Elenkov DS, Manev IM. Senior expatriate leadership’s effects on innovation and the role of cultural intelligence. Journal of World Business. 2009;44:357–369. [Google Scholar]
- Farrell JL, Young DW, Taxman FS. Effects of organizational factors on use of juvenile supervision practices. Criminal Justice and Behavior. 2011;38:565–583. [Google Scholar]
- Flynn PM, Simpson DD. Adoption and implementation of evidence-based treatment. In: Miller PM, editor. Evidence-based addiction treatment. San Diego, CA: Elsevier; 2009. pp. 419–437. [Google Scholar]
- Fuller B, Rieckmann T, Nunes E, Miller M, Arfken C, Edmundson E, McCarty D. Organizational Readiness for Change and opinions toward treatment innovations. Journal of Substance Abuse Treatment. 2007;33:183–192. doi: 10.1016/j.jsat.2006.12.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gavin M, Hofmann D. Using hierarchical linear modeling to investigate the moderating influence of leadership climate. The Leadership Quarterly. 2002;13:15–33. [Google Scholar]
- Greener JM, Joe GW, Simpson DD, Rowan-Szal GA, Lehman WEK. Influence of organizational functioning on client engagement in treatment. Journal of Substance Abuse Treatment. 2007;33:139–147. doi: 10.1016/j.jsat.2006.12.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffin M, Mathieu J. Modeling organizational processes across hierarchical levels: Climate, leadership, and group process in work groups. Journal of Organizational Behavior. 1997;18:731–744. [Google Scholar]
- Herold D, Fedor D, Caldwell S, Liu Y. The effects of transformational and change leadership on employees’ commitment to a change: A multilevel study. Journal of Applied Psychology. 2008;93(2):346–357. doi: 10.1037/0021-9010.93.2.346. [DOI] [PubMed] [Google Scholar]
- Hofmann DA. An overview of the logic and rationale of hierarchical linear models. Journal of Management. 1997;23:723–744. [Google Scholar]
- Hofmann DA, Gavin MB. Centering decisions in hierarchical linear models: Implications for research in organizations. Journal of Management. 1998;24(5):623–641. [Google Scholar]
- Hofmann DA, Morgeson F, Gerras S. Climate as a moderator of the relationship between leader-member exchange and content specific citizenship: Safety climate as an exemplar. Journal of Applied Psychology. 2003;88:170–178. doi: 10.1037/0021-9010.88.1.170. [DOI] [PubMed] [Google Scholar]
- James L. Aggregation bias in estimates of perceptual agreement. Journal of Applied Psychology. 1982;67:219–229. [Google Scholar]
- James LR, McIntyre MD. Perceptions of organizational climate. In: Murphy KR, editor. Individual differences and behavior in organizations. San Francisco: Jossey-Bass; 1996. pp. 416–450. [Google Scholar]
- Joe GW, Broome KM, Simpson DD, Rowan-Szal GA. Counselor perceptions of organizational factors and innovations training experiences. Journal of Substance Abuse Treatment. 2007;33:171–182. doi: 10.1016/j.jsat.2006.12.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirk RE. Experimental design: Procedures for the behavioral sciences. New York: Brooks/Cole; 1998. [Google Scholar]
- Klein KJ, Dansereau F, Hall RJ. Levels issues in theory development, data collection, and analysis. Academy of Management Review. 1994;19:195–229. [Google Scholar]
- Klein KJ, Knight AP. Innovation implementation: Overcoming the challenge. Current Directions in Psychological Science. 2005;14:243–246. [Google Scholar]
- Knight DK, Broome KM, Simpson DD, Edwards JR, Flynn PM. Stability and change in staff perceptions of organizational functioning. Presentation at the Addiction Health Services Research Conference; Athens, GA. 2007. Oct, [Google Scholar]
- Knudsen HK, Ducharme LD, Roman PM, Link T. Buprenorphine diffusion: The attitudes of substance abuse treatment counselors. Journal of Substance Abuse Treatment. 2005;29:95–106. doi: 10.1016/j.jsat.2005.05.002. [DOI] [PubMed] [Google Scholar]
- Knudsen HK, Roman PM. Modeling the use of innovations in private treatment organizations: The role of absorptive capacity. Journal of Substance Abuse Treatment. 2004;26:353–361. doi: 10.1016/s0740-5472(03)00158-2. [DOI] [PubMed] [Google Scholar]
- Knudsen HK, Studts JL, Boyd S, Roman PM. Structural and cultural barriers to the adoption of smoking cessation services in addiction treatment organizations. Journal of Addictive Diseases. 2010;29:294–305. doi: 10.1080/10550887.2010.489446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kozlowski S, Hattrup K. A disagreement about within-group agreement: Disentangling issues of consistency versus consensus. Journal of Applied Psychology. 1992;77:161–167. [Google Scholar]
- Lehman WEK, Greener JM, Simpson DD. Assessing organizational readiness for change. Journal of Substance Abuse Treatment. 2002;22:197–209. doi: 10.1016/s0740-5472(02)00233-7. [DOI] [PubMed] [Google Scholar]
- McLellan AT, Carise D, Kleber HD. Can the national addiction treatment infrastructure support the public’s demand for quality care? Journal of Substance Abuse Treatment. 2003;25:117–121. [PubMed] [Google Scholar]
- McNulty T, Oser C, Johnson J, Knudsen H, Roman P. Counselor turnover in substance abuse treatment centers: An organizational-level analysis. Sociological Inquiry. 2007;77:166–193. [Google Scholar]
- National Institute on Drug Abuse. NIDA/SAMHSA blending initiative. 2006 Retrieved September 23, 2009, from http://www.drugabuse.gov/Blending/
- Osborn RN, Hunt JG, Jauch LR. Toward a contextual theory of leadership. The Leadership Quarterly. 2002;13:797–837. [Google Scholar]
- Podsakoff PM, MacKenzie SB, Moorman RH, Fetter R. Transformational leader behaviors and their effects on followers’ trust in leader, satisfaction, and organization citizenship behaviors. Leadership Quarterly. 1990;1:107–142. [Google Scholar]
- Raudenbush SW, Bryk AS. Hierarchical linear models: Applications and data analysis methods. 2. Thousand Oaks, CA: Sage; 2002. [Google Scholar]
- Raudenbush SW, Bryk AS, Congdon RT. HLM 6: Hierarchical linear and nonlinear modeling. Lincolnwood, IL: Scientific Software International; 2005. [Google Scholar]
- Real K, Poole MS. Innovation implementation: Conceptualization and measurement in organizational research. Research in Organizational Change and Development. 2005;15:63–134. [Google Scholar]
- Rogers EM. Diffusion of innovations. 5. New York: Free Press; 2003. [Google Scholar]
- Roman PM, Johnson JA. Adoption and implementation of new technologies in substance abuse treatment. Journal of Substance Abuse Treatment. 2002;22:211–218. doi: 10.1016/s0740-5472(02)00241-6. [DOI] [PubMed] [Google Scholar]
- Rosenberg L. The reality of implementing evidence based practices. The Journal of Behavioral Health Services Research. 2010;37:1–3. doi: 10.1007/s11414-009-9195-x. [DOI] [PubMed] [Google Scholar]
- Rowold J, Laukamp L. Charismatic leadership and objective performance indicators. Applied Psychology: An International Review. 2009;58:602–621. [Google Scholar]
- Saldana L, Chapman JE, Henggeler SW, Rowland MD. Assessing organizational readiness for change in adolescent treatment programs. Journal of Substance Abuse Treatment. 2007;33:159–169. doi: 10.1016/j.jsat.2006.12.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schoenwald S, Henggeler S. Current strategies for moving evidence-based interventions into clinical practice: Introductory comments. Cognitive and Behavioral Practice. 2003;10:275–277. [Google Scholar]
- Schyns B. The influence of occupational self-efficacy on the relationship of leadership behavior and preparedness for occupational change. Journal of Career Development. 2004;30:247–261. [Google Scholar]
- Shanock L, Eisenberger R. When supervisors feel supported: Relationships with subordinates’ perceived supervisor support, perceived organizational support, and performance. Journal of Applied Psychology. 2006;91:689–695. doi: 10.1037/0021-9010.91.3.689. [DOI] [PubMed] [Google Scholar]
- Simpson DD. A conceptual framework for transferring research to practice. Journal of Substance Abuse Treatment. 2002;22:171–182. doi: 10.1016/s0740-5472(02)00231-3. [DOI] [PubMed] [Google Scholar]
- Simpson DD. Organizational readiness for stage-based dynamics of innovation implementation. Research on Social Work Practice. 2009;19:541–551. [Google Scholar]
- Simpson DD, Flynn PM. Moving innovations into treatment: A stage-based approach to program change. Journal of Substance Abuse Treatment. 2007;33:111–120. doi: 10.1016/j.jsat.2006.12.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simpson DD, Joe GW, Rowan-Szal GA. Linking the elements of change: Program and client responses to innovation. Journal of Substance Abuse Treatment. 2007;33:201–209. doi: 10.1016/j.jsat.2006.12.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Srivastava A, Bartol K, Locke E. Empowering leadership in management teams: Effects on knowledge sharing, efficacy, and performance. Academy of Management Journal. 2006;49:1239–1251. [Google Scholar]
- Waldman D, Yammarino F. CEO charismatic leadership: Levels-of-management and levels-of-analysis effects. Academy of Management Review. 1999;24:266–285. [Google Scholar]
- Wu C, Neubert M, Yi X. Transformational leadership, cohesion perceptions, and employee cynicism about organizational change: The mediating role of justice perceptions. Journal of Applied Behavioral Science. 2007;43:327–351. [Google Scholar]