

Abstract
Previous cross-cultural studies have repeatedly demonstrated that East Asians are more likely to show a dialectical emotional style than Americans, but do not distinguish between specific types of dialectical emotional styles. Using an age diverse sample, we found that compared to Americans, Japanese are more likely to experience both positive and negative emotions moderately frequently (i.e., moderate dialectical), but are no more likely to experience them frequently (i.e., high dialectical). Thus, dialectical emotions prevalent in East Asia may be characterised by a “middle way” rather than by emotional extremes. Furthermore, we explored whether dialectical emotion types are associated with better health profiles depending on cultural background. Our results show that the moderate dialectical type is associated with fewer physical symptoms in Japan than in the USA. Together, these findings show the cultural differences in the experience of balanced positive and negative emotions and their health correlates.
Keywords: Culture, Positive and negative emotion, Dialectical emotion, Health
Fortune and misfortune are like the twisted strands of a rope.
An East Asian proverb
The frequency with which one experiences positive or negative emotions differs from person to person. Previous studies have shown that people who tend to experience one positive emotion more frequently than other people are also more likely to experience other positive emotions more frequently than other people, while the same is true for negative emotions (Bradburn, 1969; Diener, Smith, & Fujita, 1995; Watson, Clark, & Tellegen, 1988). However, these findings focus on positive and negative emotion independently from each other and do not address how experiences of positive and negative emotion come together within a given person. We argue that among people who experience positive emotions more frequently than others, some may also experience negative emotions more frequently than others, whereas the others may experience negative emotions less frequently than others. The same may be true for those who experience positive emotions less frequently than others. Those people who report feeling both positive and negative emotions more frequently (or infrequently) than others are demonstrating a dialectical emotional style, which is defined as the propensity to experience both positive and negative over time, thus maintaining a balance between the two. A non-dialectical emotional style, on the other hand, is defined as the propensity to experience either more positive than negative emotion compared to others over time, or the reverse (more negative than positive emotion compared to others over time).
Cross-cultural studies have repeatedly documented that East Asians are more likely than Americans to show a dialectical emotional style as a group (Bagozzi, Wong, & Yi, 1999). Whereas Americans show strong negative correlations between positive and negative emotions, East Asians tend to show weaker negative, or even positive correlations between the two (Kitayama, Markus, & Kurokawa, 2000; Schimmack, Oishi, & Diener, 2002). However, the existing literature focusing on a group-level correlation does not examine how individuals experience different kinds of dialectical emotional styles. That is, the weaker correlation between positive and negative emotions among East Asians may be due to experiencing both equally frequently or infrequently. The present study addresses whether cultural differences can be observed across different kinds (high, moderate, low frequency) of dialectical emotional styles. Beyond that, and in the interest of advancing understanding of whether dialectical or non-dialectical emotion styles are functionally adaptive, with possible cultural variants therein, we also examine the health correlates of these various emotion styles.
Dialectical and non-dialectical emotional styles vis-à-vis cultural context
At the outset, we note that dialectical emotional styles manifested over time are distinct from momentary experience of both positive and negative emotion in a single situation. Studies of the latter deal primarily with the simultaneous experience of both positive and negative emotion in the moment (Bagozzi et al., 1999; Leu et al., in press; Miyamoto, Uchida, & Ellsworth, in press; Perunovic, Heller, & Rafaeli, 2007; Schimmack, 2001; Scollon, Diener, Oishi, & Biswas-Diener, 2005; Spencer-Rodgers, Peng, & Wang, 2010; Yik, 2007). Intensity ratings of positive and negative emotion in a specific moment, as well as and experience sampling methods, have been used to show cultural differences in momentary experience. The focus of the present study, in contrast, is how positive and negative emotions come together within each individual over time, thereby capturing accumulated emotional experience defined in terms of the frequency (rather than intensity) of positive and negative emotions across days, months, or even years.
Cross-cultural studies of dialectical self-view and dialectical thinking have suggested potential sources of cultural differences in dialectical emotions (Nisbett, Peng, Choi, & Norenzayan, 2001; Peng & Nisbett, 1999; Spencer-Rodgers, Boucher, Mori, Peng, & Wang, 2009). Peng and Nisbett (1999) proposed that East Asian dialectical thinking is characterised by a belief that reality is constantly changing and tolerance of contradictions by finding a “middle way”. Compared to Americans, East Asians tend to expect the present state of affairs to change (Ji, Nisbett, & Su, 2001), to prefer dialectical proverbs containing contradictions, such as “beware of your friends not your enemies”, and to seek a middle way when approaching contradictions (Peng & Nisbett, 1999). We argue that the dialectical thinking characteristic of East Asian culture underlies a cultural script about how positive and negative emotions should be combined within each individual. The dominant cultural script in East Asian culture may be to seek a middle way by experiencing a balance between positive and negative emotion.
In the Western culture, on the other hand, contradiction is something to be resolved and the middle ground should be avoided (Peng & Nisbett, 1999). When approaching contradictions, Americans tend toward polarising attitudes, whereas East Asians tend to seek a middle way (Peng & Nisbett, 1999). On the other hand, cross-cultural studies on self-evaluation have widely documented that, compared to East Asians, Westerners have more positive views toward themselves (Heine & Hamamura, 2007; Heine, Lehman, Markus, & Kitayama, 1999) and report higher well-being (Diener, Suh, Smith, & Shao, 1995; Uchida, Norasakkunkit, & Kitayama, 2004). The tendency to focus on the positives may underlie an American cultural script, which emphasises maximisation of positive emotions and minimisation of negative emotions (Kitayama et al., 2000).
The differences in dominant cultural scripts about how positive and negative emotions come together are reflected in cultural differences in dialectical emotions. Studies focusing on the correlation between positive and negative emotions showed that East Asians are more likely than Americans to show a dialectical emotional style (Bagozzi et al., 1999; Kitayama et al., 2000; Schimmack et al., 2002; Scollon et al., 2005). For example, Schimmack et al. (2002) examined correlations between frequency ratings of positive and negative emotions during the past month across 40 countries and found that negative correlations between positive and negative emotions were weaker in Asian cultures than in other cultures. In addition, using a daily experience sampling method, Scollon et al. (2005) demonstrated that Asians but not Americans show positive correlations between positive and negative emotions at a between-individual level.
Although the correlational data indicate cultural differences in overall relationships between positive and negative emotions, they do not distinguish between different types of dialectical emotional styles. That is, the weaker negative (and sometimes positive) correlation among Asians may be due to a larger number of Asians showing high, moderate, or low dialectical emotion types. At the same time, the stronger negative correlation among Americans can be due to a larger number of Americans feeling positive emotions frequently and negative emotions infrequently compared to others (“mostly positive” emotion type), or negative emotions frequently and positive emotions infrequently compared to others (“mostly negative” emotion type).
To address the above issues, we conceptualise dialectical emotions as the relative balance of positive and negative emotions compared to the distributions of those emotions in each culture. It is important to note that our conceptualisation of dialectical emotions is based on relative levels of positive and negative emotions compared to the cultural standards, which we argue is important given the notably different distributions that occur for each kind of emotion—i.e., across cultures, people are more likely to feel positive emotions than negative emotions (Diener & Diener, 1996; Schimmack, Radhakrishnan, Oishi, Dzokoto, & Ahadi, 2002; Suh, Diener, Oishi & Triandis, 1998). That is, defining dialectical emotions in terms of comparable absolute levels fails to adjust for the fact that people everywhere are far less likely to feel negative compared to positive emotions.
As illustrated in Figure 1, one can show a dialectical emotional style by experiencing a balance of positive and negative emotions: (i) frequently; (ii) moderately frequently; or (iii) infrequently. Although the previous studies have not focused on the distinction between them, the three subtypes have unique characteristics. The most characteristic of the “middle way” thinking (Peng & Nisbett, 1999) is the emotion type where positive and negative emotions are felt equally compared to others, but with moderate frequency. One who falls into this type can be characterised as showing “middle way” thinking, or a “moderate dialectical” emotion type. The emotion type where positive and negative emotions are felt with high frequency constitutes the “high dialectical” emotion type. Traditionally, high dialectical type has been considered to be the most characteristic of dialecticism or ambivalence. For example, measures of ambivalence operationalise ambivalence as the degree to which individuals hold equally strong positive and negative reactions (Priester & Petty, 1996),1 reflecting an assumption that ambivalence is not only about holding positive and negative reactions equally but also about holding them intensively/frequently. The other emotion type, where both positive and negative emotions are rarely experienced, can be called the “low dialectical” emotion type. The low dialectical emotion type has been overlooked in the literature on dialectical emotions because it has generally been considered to be a manifestation of low emotionality. However, the low dialectical emotion type shows a balance between infrequent experiences of positive and negative emotions, and thus may also be an indication of dialecticism because infrequent experiences of emotions of one valence do not imply frequent experiences of emotions of the opposite valence. We also consider two subtypes of non-dialectical emotional styles: “mostly positive” and “mostly negative”. The former is characterised by frequent experience of positive emotions combined with infrequent experience of negative emotions, whereas the latter is characterised by frequent experience of negative emotions and infrequent experience of positive emotions. These constitute important comparative types when considering links to health.
Figure 1.

Emotion typology.
Central questions are whether East Asians are more likely than Americans to fall into any of the three dialectical emotion types, whereas Americans are more likely than East Asians to fall into the non-dialectical emotion types. As we argued above, there are cultural scripts about how positive and negative emotions are combined within each individual. The East Asian cultural script emphasises a middle way by maintaining a balance between positive and negative emotion, whereas the cultural script in Western culture focuses on maximising positive emotions and minimising negative emotions. The cultural script can influence positive and negative emotions in at least two ways: through changes in means and distributions. Because correlation and typology approaches are insensitive to means, changes in means would not influence emotion types. On the other hand, changes in distributions should lead to different frequencies of emotion types. The presence of dominant cultural script does not mean that all members of the culture are equally affected by the cultural script (which would only influence means). Some individuals in a given culture may show an emotional style attuned to the cultural script, whereas the others may show an emotional style incompatible to the cultural script. However, more importantly, the proportion of individuals who align their emotional style with a dominant cultural script (e.g., “maximise positive”) will be expected to be greater in a culture in which the script is dominant (e.g., the USA) than in a culture where it is not (e.g., Japan).
We thus predicted that a larger number of East Asians than Americans would fall into the moderate dialectical emotion type, because it exemplifies the cultural script of a middle way. Showing the moderate dialectical emotion type requires one to experience both positive and negative emotions moderately frequently, thus achieving both a balance and a middle way simultaneously. We also predicted that East Asians would be more likely than Americans to fall into the low dialectical type. People may fall into the low dialectical type for at least two reasons: dialecticism or emotional detachment. For both reasons, we predicted that East Asians would be more likely to fall into this type because Eastern culture not only emphasises dialecticism (Peng & Nisbett, 1999) but also values detachment and not being swayed by feeling, as reflected in Buddhism (de Silva, 1995). At the same time, evidence supporting cultural differences in the high dialectical emotion type is unclear. The previous studies using measures of ambivalence demonstrated that East Asians show higher ambivalence, which is based on intensity as well as on balance, than Americans when evaluating themselves (Choi & Choi, 2002; Hamamura, Heine, & Paulhus, 2008; Spencer-Rodgers, Peng, Wang, & Hou, 2004), suggesting that East Asians may be more likely to fall into high dialectical emotion types than Americans. However, East Asians' tendency to report more negative reactions than Americans might have contributed to their higher ambivalence scores. Thus, it is unclear whether previous cross-cultural findings using ambivalence indices reflect cultural differences in the tendency for dialecticism or the tendency to experience negative emotions.
On the other hand, we predicted that a larger number of Americans than East Asians would fall into mostly positive non-dialectical emotion type, which is consistent with the American cultural script to experience the maximum amount of positive and minimum amount of negative emotions. A prediction about cultural differences in mostly negative non-dialectical type, however, is unclear. Cultural differences in dialectical thinking suggest that the mostly negative type is more prevalent among Americans than among East Asians, whereas cultural differences in positivity seem to suggest that the mostly negative type is more prevalent among East Asians than among Americans.
Dialectical emotional styles and health
Previous studies linking emotion to health have consistently shown that decreased negative emotion and increased positive emotion are associated with positive physical and mental health outcomes (Kiecolt-Glaser, McGuire, Robles, & Glaser, 2002; Kring, 2001; Lyubomirsky, King, & Diener, 2005; Pressman & Cohen, 2005), thereby suggesting a possibility that, across cultures, the mostly positive non-dialectical type is associated with better health and the mostly negative nondialectical type is associated with worse health. An important issue yet to be examined is whether dialectical emotions are associated with more beneficial outcomes in East Asia than in the USA. Compared to Americans, Chinese tend to view those who make dialectical predictions as wise (Ji et al., 2001). In that context, where a cultural script prescribes dialectical and middle way thinking and feeling, dialectical emotions may be associated with positive functioning, including better health outcomes, compared to Western cultures where a cultural script does not value dialecticism (Nisbett et al., 2001; Peng & Nisbett, 1999).
Cultural differences in coping styles may shed light on understanding mental and physical health correlates of emotional styles. Whereas Westerners try to influence and change their environments to fit their needs, Easterners tend to adjust themselves to their environments (Morling, Kitayama, & Miyamoto, 2002; Weisz, Rothbaum, & Blackburn, 1984). Maintenance of relative balance between positive and negative emotion (i.e., dialectical emotion style) may better prepare Easterners to attune and adjust to both positive and negative cues in their environments and thus may promote better adjustment. A previous study has shown that whereas the influencing tendency is associated with lower depression and anxiety among non-Asians, the association was weaker or even reversed among Asians and Asian Americans (Sastry & Ross, 1998), pointing out a possibility that culturally dominant strategies are associated with better health outcomes than culturally non-dominant ones. It is thus possible that the dialectical emotional style that fosters the adjustment strategy is associated with better heath outcomes in East Asia than in the USA.
Nonetheless, some have pointed to the positive role of negative emotions even in Western culture. Meaning in life and deep connection to others are frequently found when one is facing adversity and experiencing difficulty and pain, indicating that experiencing negative emotions, for some people, brings positive experiences (Ryff & Singer, 1998, 2003). Negative emotions, within a certain range, may thus be positively linked with health (Mayne, 2001). Several different lines of research—whether it be the study with people in close relationships, breast cancer patients, or people who have experienced traumatic events—suggest that experiencing and expressing negative emotions rather than suppressing them has beneficial outcomes, such as high relationship quality and fewer clinic visits, and even longer survival rate (Graham, Huang, Clark & Helgeson, 2008; Pennebaker, 1993; Spiegel, Bloom, Kraemer, & Gottheil, 1989), though the evidence showing the causal role of negative emotion is mixed (King, 2002).
Although researchers have examined the effects of positive and negative emotions on human functioning independently from each other, how health is influenced by the intermingling of the two has received little attention. In the realm of mental health, Keyes (2002) proposed a model that combined different positive and negative indicators of mental health and explored the health implications thereof. Keyes found that those who showed high mental health and no depression (i.e., labelled “flourishing”) had the least health impairments (e.g., functional limitation of daily activity or the number of workdays lost or cut back), whereas those who showed depression and low positive mental health (i.e., labelled “depressed and languishing”) had the most health impairments. The primary focus was on the “flourishing” quadrant (i.e., mostly positive non-dialectical type according to our formulation) and how it promotes health compared to the other mental health types.
We argue, however, that the particular cultural context within which one is embedded may make different positive and negative combinations more, or less, prevalent, and have distinct health correlates.2 Specifically, we hypothesised that dialectical emotional style is linked to better health in Japan than in the USA. In addition, given the literature on health costs of negative emotion and health benefits of positive emotions (Keyes, 2002; Kiecolt-Glaser et al., 2002; Kring, 2001; Lyubomirsky et al., 2005; Pressman & Cohen, 2005), we also hypothesised that, across cultures, the mostly positive non-dialectical type is linked to the best health, whereas the mostly negative non-dialectical type is linked to the worst health.
Our health measures include subjective ratings of overall health as well as specific health symptoms (e.g., headaches, trouble sleeping) in the past month. The latter measure of health symptoms strengthens the link between the temporal focus of our emotion assessments (in the past 30 days), given comparable temporal frames. Global assessments of overall health have been shown to be important predictors of numerous outcomes, including length of life (Idler & Benjamini, 1997; Siegel, Bradley, & Kasl, 2003). At the same time, global measures may also be more likely to reflect one's beliefs rather than actual experience (Robinson & Clore, 2002), which is another reason for including assessment of specific health symptoms in the past month in addition to the global subjective health measures. We explored whether the hypothesised relationships between culture and emotion types would be found for both types of health measures or whether the results would depend on the type of health measures examined.
Guiding hypotheses
We adopted a typological approach to dialecticism and hypothesised that Japanese adults would be more likely than American adults to fall into the moderate and low dialectical emotion type, whereas Americans adults would be more likely than Japanese adults to fall into the mostly positive non-dialectical emotion type. We also explored whether there were cultural differences in the proportion of individuals who fell into the high dialectical emotion type and the mostly negative non-dialectical emotion type. Second, we examined cultural differences in the health correlates of emotion types. We hypothesised that, across cultures, the mostly positive non-dialectical type would be linked to the best health, whereas the mostly negative non-dialectical type would be linked to the worst health. We also hypothesised that the dialectical emotional style would be linked to better health in Japan than in the USA. We further explored whether cultural differences in health correlates depend on specific types of dialectical emotions.
METHOD
Participants
The American sample
We used the data from the Midlife in the United States (MIDUS) II survey, which is a national probability sample recruited through random digit dialling procedures. The survey included a telephone interview and a self-administered questionnaire. The present analyses are based on 3828 individuals (1722 males and 2106 females) who completed emotion measures. The ages ranged from 30 to 84 years (M=55.92). Thirty-three percent of the individuals had a high-school degree or less and 38.7% had a 4-year college degree or higher.
The Japanese sample
A convenience sample of Japanese adults from both the metropolitan area (Tokyo) and a provincial capital area (Sapporo) were recruited to participate in a survey study. Participants in Tokyo were recruited through adult education classes; the participants in Sapporo were recruited through college students, who asked their adult family members to fill out the questionnaire. The present analyses are based on 494 Japanese adults (212 males and 282 females) who completed the emotion measures. Participants completed a self-administered questionnaire. The ages ranged from 20 to 81 years (M=51.57). As to educational background, 36.4% completed high-school or less and 33.5% had a 4-year college degree of higher. Although the Japanese sample is not a probability sample, demographic factors were comparable with the American sample. In addition, the demographic factors of the Japanese sample were also comparable to the Japanese census data. According to the 2000 Japanese national population census data, among the individuals over 14 years old, 41.6% have a high-school degree or less, 24.6% have a 4-year college degree or higher, and 8.2% are still in school.
Emotion measures
Positive and negative emotions
To measure dialectical emotions, participants were asked to rate how much of the time during the past 30 days they felt six negative emotions and six positive emotions (see Mroczek & Kolarz, 1998, for details about the sources) using a 5-point rating scale ranging from none of the time to all the time. The positive emotions were: cheerful; in good spirits; extremely happy; calm and peaceful; satisfied; and full of life. The negative emotions were: so sad nothing could cheer you up; nervous; restless or fidgety; hopeless; that everything was an effort; and worthless. Cronbach's alphas were .91 and .94 for positive emotions and .85 and .87 for negative emotions, Americans and Japanese, respectively.
Health measures
Subjective health
To assess overall health, participants were asked to report their health on an 11-point scale ranging from 0 (the worst possible health) to 10 (the best possible health).
Physical symptoms
The level of health was also measured by the number of specific physical symptoms (i.e., headaches, backaches, sweating a lot, irritability, hot flushes or flashes, aches or stiffness in joints, trouble sleeping, leaking urine, and pain or discomfort during intercourse) that participants reported experiencing during the past 30 days.
Procedure
The measures were collected as part of the larger self-administered questionnaire. Respondents first responded to the subjective health measure together with other measures relevant to health (e.g., health locus of control), which was followed by questions about physical symptoms. Subsequently, they reported their experiences of negative and positive emotions. The order of the four measures was the same in both cultures.
RESULTS
The comparison of the means showed that Americans reported experiencing positive emotions more frequently (M=3.43, SD=0.70) and negative emotions less frequently (M=1.50, SD=0.56) than Japanese did (Ms=3.36, 1.75, SDs=0.70, 0.69), ts(4320)=2.06, 8.99, 95% CIs=.00 to .14, .19 to .30, ds=.10, .43, positive and negative emotion, respectively. Following the previous studies on dialectical emotion, we first computed the correlation between positive and negative emotion. Consistent with previous cross-cultural studies, Americans showed a stronger inverse relationship between positive and negative emotion (r=−.61) than Japanese (r=−.42), Z=5.45, p<.001, q=0.26 (Cohen, 1977).
Cultural differences in dialectical emotion types
Next, we used a typological approach to classify respondents into three dialectical types and two non-dialectical types. This was accomplished by first partitioning the two cultural samples into quartiles according to their separate positive and negative emotions scores and then generating a 4×4 table with positive emotion quartiles as a row and negative emotion quartiles as a column (Goodman, 1969; see Table 1). We determined the quartiles separately for Japanese and Americans, given cultural differences in use of self-rating scales. To deal with the latter, researchers often standardise the data before cross-cultural comparison (Bond, 1988; Tsai, Knutson, & Fung, 2006). We adjusted for this cultural difference by determining the quartiles based on the distribution within each culture.
Table 1.
A crosstab table according to respondent's placement in positive emotion quartile and negative emotion quartile by culture
| Positive emotion quartile | Negative emotion quartile |
|||
|---|---|---|---|---|
| highest | 2nd highest | 2nd lowest | lowest | |
| Americans highest | 77 (2.01) | 196 (5.12) | 245 (6.40) | 965 (25.21) |
| 2nd highest | 72 (1.88) | 192 (5.02) | 151 (3.94) | 342 (8.93) |
| 2nd lowest | 212 (5.54) | 205 (5.36) | 145 (3.79) | 200 (5.22) |
| lowest | 503 (13.10) | 170 (4.44) | 69 (1.80) | 84 (2.19) |
| Japanese highest | 10 (2.02) | 19 (3.85) | 37 (7.49) | 71 (14.37) |
| 2nd highest | 24 (4.86) | 30 (6.07) | 38 (7.69) | 42 (8.50) |
| 2nd lowest | 45 (9.11) | 36 (7.29) | 27 (5.47) | 30 (6.07) |
| lowest | 36 (7.29) | 20 (4.05) | 17 (3.44) | 12 (2.43) |
Note: Numbers are cell counts. Percentages are shown in parentheses.
To deal with ties between quartiles, we rounded each cut up to a whole number. For example, if the 25th percentile of the positive emotion measure was a score of 13.47, we rounded up to a score of 14, so that respondents with the same score would not be distributed into different quartiles. This resulted, however, in having less than 20% of the respondents in the last quartile. The distributions for both cultures were, however, skewed toward the higher end for the positive emotion rating and the lower end for the negative emotion rating, and quartile cuts were counted from the skewed ends. Thus, counting in the above fashion allowed us to better reflect the distributions of the emotion ratings.
Looking at Table 1, it is noteworthy that the largest cultural differences were found in the most extreme two non-dialectical cells: the highest positive and the lowest negative cell (i.e., extremely positive cell; 25% and 14%, Americans and Japanese, respectively, Z=5.31, p<.001, h=.28; Cohen, 1977) and the highest negative and the lowest positive cell (i.e., extremely negative cell; 13% and 7%, Americans and Japanese, respectively, Z=3.71, p<.001, h=20). These patterns are consistent with the stronger negative correlation between positive and negative emotion found in the American sample than in the Japanese sample. The fact that Americans were more likely than Japanese to fall not only into the extremely positive cell but also into the extremely negative cell suggests that dialecticism is underlying the cultural differences in the correlation. At the same time, the cultural difference was larger for the extremely positive cell (11%) than for the extremely negative cell (6%), Z=3.27, p<.001, h=.18, suggesting that cultural differences in positivity may also play a role. On the other hand, there were four cells that Japanese were significantly more likely than Americans to fall into, though there were spread across the table, Zs=2.45 to 4.23, hs=.06 to .17.
To test our hypothesis regarding specific emotion types, we divided the respondents into emotion types as depicted in Figure 1 based on their location on the transition table. The mostly positive non-dialectical group (positive emotion ranges=3.5 to 5, 3.17 to 5 and Ms=3.98, 4.05, for Americans and Japanese, respectively; negative emotion ranges=1 to 1.33, 1 to 1.67 and Ms=1.11, 1.14) corresponded to three cells in the top right corner and the mostly negative non-dialectical group (positive emotion ranges=1 to 3.33, 1 to 3 and Ms=2.53, 2.67, and negative emotion ranges=1.5 to 5, 1.83 to 5 and Ms=2.24, 2.65) corresponded to three cells in the bottom left corner. The low dialectical group (positive emotion ranges=1 to 3.33, 1 to 3 and Ms=3.11, 2.70, and negative emotion ranges=1 to 1.33, 1 to 1.67 and Ms=1.14, 1.16) was three cells in the bottom right corner, the moderate dialectical group (positive emotion ranges=3 to 3.67, 3 to 3.83 and Ms=3.38, 3.23, and negative emotion ranges=1.33 to 1.67, 1.33 to 2.17 and Ms=1.47, 1.75) was four cells in the middle, and the high dialectical group (positive emotion ranges=3.5 to 5, 3.17 to 5 and Ms=3.92, 3.80, and negative emotion ranges=1.5 to 5, 1.83 to 5 and Ms=1.79, 2.44) was three cells in the top left corner.
We compared proportions of those falling into each of the emotion types to examine cultural differences in the prevalence of emotion types. As shown in Figure 2, supporting our hypothesis, Japanese were more likely than Americans to fall into the moderate dialectical type (Z=4.48, p<.001, h=.20). As predicted, Japanese were more likely to fall into the low dialectical type than Americans, though the difference was marginally significant (Z=1.94, p=.05, h=.09). The cultural difference in the prevalence of the high dialectical type was not statistically significant (Z=1.24, ns, h=.06). On the other hand, compared to Japanese, Americans were more likely to fall into the mostly positive non-dialectical type (Z=4.36, p<.001, h=.21), which supported our second hypothesis. However, the difference in the prevalence of the mostly negative non-dialectical type was not statistically significant (Z=1.33, ns, h=.06). We further conducted multinomial regressions for Americans and Japanese separately to examine within-culture differences in the proportions of emotion types. Most of the differences between emotion types were significant in the USA, Wald=23.25 to 638.26, dfs=1, ps<.001, and in Japan, Wald=3.86 to 42.39, dfs=1, ps<.05 to .001, except for the difference between low and high dialectical emotion types, Wald=0.09, 0.32, dfs=1, ns, for Americans and Japanese, respectively. Importantly, in Japan, the difference between mostly positive type and moderately dialectical type was not significant either, Wald=1.28, df=1, p>.2, suggesting that moderately dialectical type was as prevalent as mostly positive type in Japan.
Figure 2.
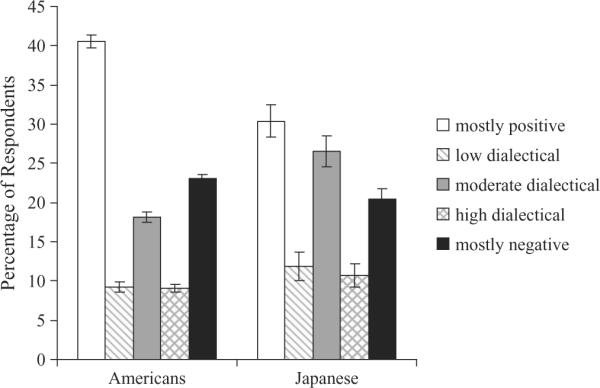
Percentage of respondents falling into emotion types. Error bars represent standard errors.
Together, the above findings suggest that Japanese adults are more likely than Americans adults to fall into the moderate dialectical emotion type. On the other hand, the Americans are more likely than the Japanese to fall into the mostly positive non-dialectical type. We did not observe cultural differences in the high dialectical type or in the mostly negative non-dialectical type. Cultural differences in the low dialectical type were weak, though in the predicted direction.
Cultural differences in health concomitants of dialectical emotions
We next examined whether dialectical emotions are associated with better health profiles in Japan than in the USA. Health status was measured in terms of subjective rating of general health as well as the number of physical symptoms respondents reported to have experienced during the past 30 days. The two measures were significantly correlated with each other in both cultures, rs=−.29.
Overall, the Japanese reported lower subjective health than the Americans did (Ms=6.83 vs. 7.40, SDs=1.90, 1.57), t(4302)=7.07, d=0.34, but fewer health symptoms than the Americans did (Ms=2.53 vs. 4.88 out of 9 health conditions, SDs=1.97, 1.97), t(4299)=25.04, d=1.20. Although cultural differences in levels of health are interesting in themselves, we did not want such differences in overall means (as are frequently found in cultural research; e.g., Bond, 1988) to obscure the comparison between cultures. We thus standardised the measures within each culture.
To examine how dialectical emotion types are linked to subjective rating of general health across cultures, a 2 (Culture: Japan, USA)×5 (Emotion Types: mostly positive vs. mostly negative vs. low dialectical vs. moderate dialectical vs. high dialectical)×2 (Gender) analysis of covariance (ANCOVA) was performed with age as a covariate and subjective health as a dependent variable. As shown in Figure 3, there was a main effect of Emotion Types, F(4, 4275)=73.71, p<.001. Planned contrasts showed that the mostly positive emotion type was associated with higher subjective health than any of the dialectical emotion types, t(4275)=9.64, 7.67, 7.36, p<.001, d=0.58, 0.51, 0.49, for low, moderate, and high dialectical types, respectively, which in turn were associated with higher subjective health than the mostly negative type, t(4275)=9.91, 13.75, 11.18, p<.001, d=0.51, 0.60, 0.57. This supports our hypothesis that, across cultures, the mostly positive type is associated with the best health and the mostly negative type is associated with the worst health. None of the other effects were significant, including the hypothesised interaction between Culture and Emotion Type.
Figure 3.

Subjective health: Interaction between emotion type and culture. Error bars represent standard errors.
To examine whether dialectical emotion types are linked to a more specific measure of health across cultures, a 2 (Culture)×5 (Emotion Types: mostly positive vs. mostly negative vs. low dialectical vs. moderate dialectical vs. high dialectical)×2 (Gender) ANCOVA was performed with age as a covariate and physical symptoms as a dependent variable. In addition to the main effect of Emotion Type, F(4, 4272)=79.76, p<.001, a two-way interaction between Culture and Emotion Types was significant, F(4, 4272)=4.40, p<.005. As shown in Figure 4, supporting our hypothesis, in both cultures, the mostly positive non-dialectical type was associated with the lowest number of physical symptoms, whereas the mostly negative non-dialectical type was associated with the largest number of physical symptoms, though the mostly positive type was not significantly different from the low dialectical type among Japanese, t(4272)=1.11, ns. In addition, whereas the moderate dialectical type was associated with a lower number of reported physical symptoms in Japan than in the USA, t(4272)=2.20, p<.05, d=0.27, the mostly negative non-dialectical types were associated with a larger number of physical symptoms in Japan than in the USA, t(4275)=2.39, p<.05, d=0.26. There was no cultural difference in low and high dialectical and mostly positive types, ts(4272)=1.40, 1.79, 0.87, ns, d=0.20, 0.28, 0.07, low dialectical, high dialectical, and mostly positive, respectively.3
Figure 4.
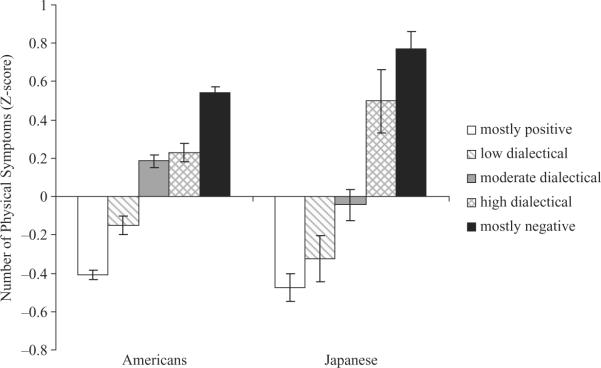
Number of physical symptoms: Interaction between emotion type and culture. Error bars represent standard errors.
To examine whether emotion types explain physical symptoms above and beyond the absolute levels of positive and negative emotion, we entered the level of positive and negative emotion as covariates. Both the main effect of Emotion Type, F(1, 4270)=6.84, p<.001, and the interaction between Culture and Emotion Type remained significant, F(4, 4270)=3.66, p<.01. Even after controlling for the level of positive and negative emotions, moderate dialectical emotion type was significantly associated with better health in Japan than in the USA, t(4270)=4.37, p<.01. The cultural differences were not significant for the other emotion types, ts<1.79. These findings provide support to our hypothesis that dialectical emotional style—especially the moderately dialectical type—is associated with better health in Japan than in the USA. At the same time, once the levels of emotions were controlled for, cultural differences in the health correlates of the mostly negative non-dialectical type disappeared. The effects of the mostly negative non-dialectical type on health symptoms may be mainly driven by the absolute levels of positive and negative emotion.
Furthermore, we also included subjective health as another covariate to explore whether dialectical emotion types explain physical symptoms even when subjective judgement of health is controlled for. Again, both the main effect of Emotion Type, F(1, 4251)=6.84, p<.001, and the interaction between Culture and Emotion Type remained significant, F(4, 4251)=3.83, p=.005. The moderate dialectical type was associated with fewer reported physical symptoms in Japan than in the USA, t(4251)=4.29, p<.01. The cultural differences in other emotion types were not significant, ts<1.71. The fact that cultural differences in the health benefits of emotion types were observed even after controlling for subjective health suggests that the observed effects on health reflect relatively objective health benefits.
DISCUSSION
Previous cross-cultural studies have repeatedly demonstrated that East Asians tend to show more dialectical emotional styles than Americans. The present study extended the previous studies by exploring the specific ways in which positive and negative emotions are combined. By distinguishing between different types of dialectical emotional style, we found that Japanese are more likely than Americans to show a moderate dialectical type. On the other hand, Americans are more likely than Japanese to show a mostly positive emotion type. The cultural differences in high dialectical emotion type and in mostly negative emotion type were not significant. Cultural differences in the low dialectical emotion type were statistically marginal. Furthermore, we explored whether dialectical emotion types were linked to better health profiles depending on one's cultural background. Our results show that the moderate dialectical emotion type was associated with fewer health symptoms in Japan than in the USA. Overall, such results suggest culturally contingent pathways between emotions and health.
Cultural differences and similarity in emotional types
The present study found that Japanese are more likely than Americans to fall into the moderately dialectical emotion type, whereas Americans are more likely than Japanese to fall into the mostly positive emotion type. A previous cross-cultural study on cognition has shown that, when dealing with contradictions, East Asians tend to seek a middle way, whereas Americans tend to polarise their attitudes (Peng & Nisbett, 1999). The present results suggest that such cognitive differences can be extended to emotional experiences. Whereas East Asians seek a middle way by maintaining a balance between a moderate amount of emotions (compared to the cultural standards), Americans tend to polarise their emotional experiences by maximising positive emotions and minimising negative emotions. At the same time, cultural differences in the high dialectical type were not significant, indicating that cultural differences in emotional dialectics are manifested mostly in the middle-way thinking rather than in the large swing of the emotional pendulum. East Asian culture may socialise individuals to seek a balance in a relatively moderate way.
It is noteworthy that cultural differences in the mostly negative type were not significant either. In addition, the crosstab table (Table 1) showed that Americans were more likely than Japanese to fall into the highest negative and the lowest positive (i.e., the extreme case of the mostly negative type). Cross-cultural studies have repeatedly demonstrated the relative negativity of East Asians compared to Westerners (Diener et al., 1995; Heine & Hamamura, 2007; Heine et al., 1999; Uchida et al., 2004). In fact, we also found cultural differences in the overall means of positive and negative emotions; Japanese tended to feel positive emotions less frequently and negative emotions more frequently than Americans. However, when we focused on the emotional styles, which were determined based on the distribution within each culture, there was no cultural difference in the likelihood of falling into the mostly negative type and Americans were more likely than Japanese to fall into the extremely negative cell, although Americans were, as predicted, much more likely to fall into the mostly positive type and to the extremely positive cell than Japanese. Furthermore, the mostly negative type was associated with worse health symptoms in Japan than in the USA, suggesting that being predominantly negative in emotional experience is not adaptive in Japan. It appears that Japan is a culture that does not extol negative over positive emotion, but rather a balance between the two.
Health implications
The moderate dialectical emotion type was associated with better health, specifically a fewer number of health symptoms over the last 30 days, in Japan than in the USA. Thus, practising the middle way emotionally seems to have health benefits in Japan. These results suggest that culturally distinct emotion types may be functionally adaptive. What is equally noteworthy is that the moderate dialectical emotion type in the USA is conducive to poorer health, after controlling for overall cultural differences in the level of health. Thus, cultural context, or more importantly, fit of one's emotional style with the cultural context, seems to be essential for understanding variation in health symptoms. At the same time, the present research is based on a single time of measurement, which obscures causal directionality. Dialectical emotional styles may confer better health in Japan than in the USA, but it is also possible that better health increases emotional balance in Japan, whereas good health in the USA may promote the mostly positive non-dialectical emotion profile.
On the other hand, the moderate dialectical emotion type was not associated with higher ratings of global health in Japan than in the USA. It is noteworthy that we observed the health benefits of the moderate dialectical emotion type with the specific measure of health (i.e., physical symptoms such as headaches and back pain), but not with the more global measure of health. Non-specific measures tend to reflect people's beliefs about their health rather than the actual experience of health (Robinson & Clore, 2002). It is possible that, in Japan, the moderate dialectical emotion may be associated with better health experiences, but not with one's beliefs about overall health.
It should be noted that we also found cultural differences in the overall number of health symptoms and subjective rating of health. Literature on cultural differences in physical health provides mixed evidence along these lines. Some have found poorer physical health among Americans than among Japanese (Alonso et al., 2004; Janevic, Ajrouch, Merline, Akiyama, & Antonucci, 2000), whereas the others do not find such cultural differences (Janevic et al., 2000). Interestingly, corresponding to our results, those that found better health among Japanese tend to use specific health conditions as an index of physical health, whereas those that did not tend to use global self-report measures of health (e.g., asking respondents to rate how healthy they are).
Limitations and future directions
There are several limitations of the present study. A first is the use of self-report measures to assess both emotional experience as well as health outcomes, and thereby, possibly compounding person-specific tendencies to construe one's feelings and one's health in generally positive or negative ways. To strengthen the evidence that dialectical and non-dialectical emotional styles are functionally adaptive in ways that differ by culture, it would be valuable to assess health with more objective indicators, such as measures of stress hormones (e.g., levels of daily salivary cortisol, cardiovascular risk factors, or inflammatory factors) and sleeping quality, many of which have been shown to covary with psychosocial factors and socioeconomic status (e.g., Friedman et al., 2007; Ryff et al., 2006). Examining how emotional styles are linked to such objective measures of health, depending on the cultural context, would richly extend the present findings. Furthermore, the present study as well as the literature does not provide evidence to determine whether low dialectical emotion type is a manifestation of dialecticism or emotional detachment. Future research may disentangle the causes of low dialectical emotion type by measuring physiological responses to a physical challenge task, which examines whether the low dialectical type is associated with quick recovery from the challenge task or with blunted physiological reaction.
Second, the present study measured retrospective emotions and thus may reflect participants' beliefs about their emotions rather than their actual emotions. Cultural differences tend to be larger when self-reports are based on one's beliefs than on immediate experience (Robinson & Clore, 2002). At the same time, recent studies demonstrated cultural differences in dialectal emotions even when measuring online report of emotions (Bagozzi et al., 1999; Perunovic et al., 2007), indicating that actual emotional experience may also differ across cultures.
Third, the present study focused on the East–West differences in dialectical emotions but there may be sociocultural variations within each culture. For example, low socioeconomic status in the USA is associated with lower perceived control and lower health (Lachman & Weaver, 1998). The lack of control may lead low SES individuals to fall into the dialectical emotional style, since they may need to adjust to positive and negative events impinging on them (Markus, Ryff, Curhan, & Palmersheim, 2004). High SES individuals, in turn, may be especially likely to fall into the mostly positive emotional type, because they can exert control over their lives to maximise the positive and minimise the negative. In addition, individuals are not fixed into a particular emotional type. Throughout the life-course trajectory, individuals may change the configuration of their positive and negative emotions depending on role changes or other adversities. Examining the age trajectories of emotional types and how they may depend on cultural context will allow us to capture the nature of dialectical emotions across time.
Fourth, future research may also examine social relational factors that underlie emotional styles. It is likely that relational contexts promote certain emotional styles; managing multiple roles or being embedded in the prescribed relationships instead of voluntarily choosing the relationships (Adams, 2003; Adams & Plaut, 2003) may be associated with experiencing dialectical emotions. For example, living with in-laws may bring both positives and negatives to one's life. In addition, major life events provide particular context with which one needs to cope. Previous research has suggested that, in the USA, positive and negative emotions are more inversely correlated when people recently experienced stressful life events (e.g., the death of a spouse; Zautra, Reich, Davis, Potter, & Nicolson, 2000). Such an inverse correlation may indicate that non-dialectical emotion style is more prevalent than dialectical emotion style among stressed individuals, but does not tell us whether there are more mostly positive types than mostly negative types, or which emotional style leads to a better adjustment. The present typology could be useful in determining the specific emotional style that leads to resilience under stressful circumstances.
Conclusion
An emerging body of research has documented cultural differences in dialectical emotions (Bagozzi et al., 1999; Kitayama et al., 2000; Perunovic et al., 2007; Schimmack, 2009; Schimmack et al., 2002; Scollon et al., 2005). The present study extended these findings by replicating the previous cultural differences found with college samples in a more age-diverse sample and by specifying the particular ways in which positive and negative emotions are combined. In addition, health implications of dialectical emotional styles were explored. These findings show how the functions of dialectical emotional styles are contingent on cultural context in which one is embedded. Being dialectical can bring health benefits for people living in the Japanese cultural context, but may be accompanied by costs for those living in the USA, which heavily rests on a cultural prescription to be mostly positive.
Acknowledgments
This research was supported by two grants from the National Institute on Aging, one to conduct the MIDUS longitudinal follow-up study (P01-AG020166), and the other to conduct parallel research in Japan (R37-AG027343).
Footnotes
It is important to note that our conceptualisation of dialectical emotions is also distinct from formulations of hedonic balance (Bradburn, 1969), which is the relative preponderance of positive over negative emotions and is derived by subtracting negative emotions from positive emotions. Neither ambivalence indices nor hedonic balance distinguish between different degrees of dialectical emotions (high, moderate, or low frequency) and thus are different from our typology approach.
Also, while Keyes included numerous measures of psychological, social, and emotional functioning in defining his typology, we focus exclusively on specific combinations of positive and negative emotions.
In addition, females were more likely than males to report a larger number of physical symptoms, F(1, 4272) 33.91, p<.001. There was an interaction between culture and gender, indicating that the gender difference was larger in the USA than in Japan, F(1, 4272) 4.35, p<.05. There was no three-way interaction between gender, culture, and emotion type, F<1.
REFERENCES
- Adams G. The cultural grounding of personal relationship: Enemyship in North American and West African worlds. Journal of Personality and Social Psychology. 2003;88:948–968. doi: 10.1037/0022-3514.88.6.948. [DOI] [PubMed] [Google Scholar]
- Adams G, Plaut VC. The cultural grounding of personal relationship: Friendship in North American and West African worlds. Personal Relationships. 2003;10:335–349. doi: 10.1037/0022-3514.88.6.948. [DOI] [PubMed] [Google Scholar]
- Alonso J, Ferrer M, Gandek B, Ware J, Aaronson N, Mosconi P, et al. Health-related quality of life associated with chronic conditions in eight countries: Results from the International Quality of Life Assessment (IQOLA) Project. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment Care & Rehabilitation. 2004;13:283–298. doi: 10.1023/b:qure.0000018472.46236.05. [DOI] [PubMed] [Google Scholar]
- Bagozzi RP, Wong N, Yi Y. The role of culture and gender in the relationship between positive and negative affect. Cognition and Emotion. 1999;13:641–672. [Google Scholar]
- Bond MH. Finding universal dimensions of individual variation in multicultural studies of values: The Rokeach and Chinese value surveys. Journal of Personality and Social Psychology. 1988;55:1009–1015. [Google Scholar]
- Bradburn N. The structure of psychological well-being. Aldine; Oxford, UK: 1969. [Google Scholar]
- Choi I, Choi Y. Culture and self-concept flexibility. Personality and Social Psychology Bulletin. 2002;28:1508–1517. [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. rev. ed. Academic Press; New York: 1977. [Google Scholar]
- de Silva P. Theoretical perspectives on emotions in early Buddhism. In: Marks J, Ames RT, editors. Emotions in Asian thought: A dialogue in comparative philosophy. State University of New York Press; Albany, NY: 1995. pp. 109–121. [Google Scholar]
- Diener E, Diener C. Most people are happy. Psychological Science. 1996;7:181–185. [Google Scholar]
- Diener E, Smith H, Fujita F. The personality structure of affect. Journal of Personality and Social Psychology. 1995;69:130–141. [Google Scholar]
- Diener E, Suh EM, Smith H, Shao L. National differences in reported subjective well-being: Why do they occur? Social Indicators Research. 1995;34:7–32. [Google Scholar]
- Friedman E, Love G, Rosenkranz M, Urry H, Davidson R, Singer B, et al. Socioeconomic status predicts objective and subjective sleep quality in aging women. Psychosomatic Medicine. 2007;69:682–691. doi: 10.1097/PSY.0b013e31814ceada. [DOI] [PubMed] [Google Scholar]
- Goodman LA. How to ransack social mobility tables and other kinds of cross-classification tables. The American Journal of Sociology. 1969;75:1–40. [Google Scholar]
- Graham S, Huang J, Clark M, Helgeson V. The positives of negative emotions: Willingness to express negative emotions promotes relationships. Personality and Social Psychology Bulletin. 2008;34:394–406. doi: 10.1177/0146167207311281. [DOI] [PubMed] [Google Scholar]
- Hamamura T, Heine S, Paulhus D. Cultural differences in response styles: The role of dialectical thinking. Personality and Individual Differences. 2008;44:932–942. [Google Scholar]
- Heine SJ, Hamamura T. In search of East Asian self-enhancement. Personality and Social Psychology Review. 2007;11:1–24. doi: 10.1177/1088868306294587. [DOI] [PubMed] [Google Scholar]
- Heine SJ, Lehman DR, Markus HR, Kitayama S. Is there a universal need for positive self-regard? Psychological Review. 1999;106:766–794. doi: 10.1037/0033-295X.106.4.766. [DOI] [PubMed] [Google Scholar]
- Idler EL, Benjamini Y. Self-rated health and mortality: A review of twenty-seven community studies. Journal of Health and Social Behavior. 1997;38:21–37. [PubMed] [Google Scholar]
- Janevic M, Ajrouch K, Merline A, Akiyama H, Antonucci T. The social relations–physical health connection: A comparison of elderly samples from the United States and Japan. Journal of Health Psychology. 2000;5:413–429. doi: 10.1177/135910530000500402. [DOI] [PubMed] [Google Scholar]
- Ji LJ, Nisbett RE, Su Y. Culture, change, and prediction. Psychological Science. 2001;12:450–456. doi: 10.1111/1467-9280.00384. [DOI] [PubMed] [Google Scholar]
- Keyes CLM. The mental health continuum: From languishing to flourishing in life. Journal of Health and Social Behavior. 2002;43:207–222. [PubMed] [Google Scholar]
- Kiecolt-Glaser J, McGuire L, Robles T, Glaser R. Emotions, morbidity, and mortality: New perspectives from psychoneuroimmunology. Annual Review of Psychology. 2002;53:83–107. doi: 10.1146/annurev.psych.53.100901.135217. [DOI] [PubMed] [Google Scholar]
- King L. The writing cure: How expressive writing promotes health and emotional well-being. American Psychological Association; Washington, DC: 2002. Gain without pain? Expressive writing and self-regulation; pp. 119–134. [Google Scholar]
- Kitayama S, Markus HR, Kurokawa M. Culture, emotion, and well-being: Good feelings in Japan and the United States. Cognition and Emotion. 2000;14:93–124. [Google Scholar]
- Kring A. Emotion and psychopathology. In: Mayne TJ, Bonanno GA, editors. Emotions: Current issues and future directions. Guilford Press; New York: 2001. pp. 337–360. [Google Scholar]
- Lachman ME, Weaver SL. The sense of control as a moderator of social class differences in health and well-being. Journal of Personality and Social Psychology. 1998;74(3):763–773. doi: 10.1037//0022-3514.74.3.763. [DOI] [PubMed] [Google Scholar]
- Leu J, Mesquita B, Ellsworth PC, Zhang Z, Huijan Y, Buchtel E, et al. Situational differences in dialectical emotions: Boundary conditions in a cultural comparison of North Americans and East Asians. Cognition and Emotion. in press. Advance online publication. doi:10.1080/02699930802650911. [Google Scholar]
- Lyubomirsky S, King L, Diener E. The benefits of frequent positive affect: Does happiness lead to success? Psychological Bulletin. 2005;131:803–855. doi: 10.1037/0033-2909.131.6.803. [DOI] [PubMed] [Google Scholar]
- Markus H, Ryff C, Curhan K, Palmersheim K. In their own words: Well-being at midlife among high school-educated and college-educated adults. In: Brim OG, Ryff CD, Kessler RC, editors. How healthy are we? A national study of well-being at midlife. University of Chicago Press; Chicago: 2004. pp. 273–319. [Google Scholar]
- Mayne T. Emotions and health. In: Mayne TJ, Bonanno GA, editors. Emotions: Current issues and future directions. Guilford Press; New York: 2001. pp. 361–397. [Google Scholar]
- Miyamoto Y, Uchida U, Ellsworth PC. Culture and mixed emotions: Co-occurrence of positive and negative emotions in Japan and the US. Emotion. doi: 10.1037/a0018430. in press. [DOI] [PubMed] [Google Scholar]
- Morling B, Kitayama S, Miyamoto Y. Cultural practices emphasize influence in the US and adjustment in Japan. Personality and Social Psychology Bulletin. 2002;28:311–323. [Google Scholar]
- Mroczek DK, Kolarz CM. The effect of age on positive and negative affect: A developmental perspective on happiness. Journal of Personality and Social Psychology. 1998;75:1333–1349. doi: 10.1037//0022-3514.75.5.1333. [DOI] [PubMed] [Google Scholar]
- Nisbett RE, Peng K, Choi I, Norenzayan A. Culture and systems of thought: Holistic versus analytic cognition. Psychological Review. 2001;108:291–310. doi: 10.1037/0033-295x.108.2.291. [DOI] [PubMed] [Google Scholar]
- Peng K, Nisbett RE. Culture, dialectics, and reasoning about contradiction. American Psychologist. 1999;54:741–754. [Google Scholar]
- Pennebaker JW. Putting stress into words: Health, linguistic, and therapeutic implications. Behavioral Research and Therapy. 1993;31:539–548. doi: 10.1016/0005-7967(93)90105-4. [DOI] [PubMed] [Google Scholar]
- Perunovic WQE, Heller D, Rafaeli E. Within-person changes in the structure of emotion: The role of cultural identification and language. Psychological Science. 2007;18:607–613. doi: 10.1111/j.1467-9280.2007.01947.x. [DOI] [PubMed] [Google Scholar]
- Pressman S, Cohen S. Does positive affect influence health? Psychological Bulletin. 2005;131:925–971. doi: 10.1037/0033-2909.131.6.925. [DOI] [PubMed] [Google Scholar]
- Priester JR, Petty RE. The gradual threshold model of ambivalence: Relating the positive and negative bases of attitudes to subjective ambivalence. Journal of Personality and Social Psychology. 1996;71:431–449. doi: 10.1037//0022-3514.71.3.431. [DOI] [PubMed] [Google Scholar]
- Robinson MD, Clore GL. Belief and feeling: Evidence for an accessibility model of emotional self-report. Psychological Bulletin. 2002;128:934–960. doi: 10.1037/0033-2909.128.6.934. [DOI] [PubMed] [Google Scholar]
- Ryff C, Love G, Urry H, Muller D, Rosenkranz M, Friedman E, et al. Psychological well-being and ill-being: Do they have distinct or mirrored biological correlates? Psychotherapy and Psychosomatics. 2006;75:85–95. doi: 10.1159/000090892. [DOI] [PubMed] [Google Scholar]
- Ryff CD, Singer B. The contours of positive human health. Psychological Inquiry. 1998;9:1–28. [Google Scholar]
- Ryff CD, Singer B. Ironies of the human condition: Well-being and health on the way to mortality. In: Aspinwall LG, Staudinger UM, editors. A psychology of human strengths: Fundamental questions and future directions for a positive psychology. American Psychological Association; Washington, DC: 2003. pp. 271–287. [Google Scholar]
- Sastry J, Ross C. Asian ethnicity and the sense of personal control. Social Psychology Quarterly. 1998;61:101–120. [Google Scholar]
- Schimmack U. Pleasure, displeasure, and mixed feelings: Are semantic opposites mutually exclusive? Cognition and Emotion. 2001;15:81–97. [Google Scholar]
- Schimmack U. Culture, gender, and the bipolarity of momentary affect: A critical re-examination. Cognition and Emotion. 2009;23:599–604. [Google Scholar]
- Schimmack U, Oishi S, Diener E. Cultural influences on the relation between pleasant emotions and unpleasant emotions: Asian dialectic philosophies or individualism–collectivism? Cognition and Emotion. 2002;16:705–719. [Google Scholar]
- Schimmack U, Radhakrishnan P, Oishi S, Dzokoto V, Ahadi S. Culture, personality, and subjective well-being: Integrating process models of life satisfaction. Journal of Personality and Social Psychology. 2002;82:582–593. [PubMed] [Google Scholar]
- Scollon C, Diener E, Oishi S, Biswas-Diener R. An experience sampling and cross-cultural investigation of the relation between pleasant and unpleasant affect. Cognition and Emotion. 2005;19:27–52. [Google Scholar]
- Siegel M, Bradley EH, Kasl S. Self-rated life expectancy as a predictor of mortality: Evidence from the HRS and AHEAD surveys. Gerontology. 2003;49:265–271. doi: 10.1159/000070409. [DOI] [PubMed] [Google Scholar]
- Spencer-Rodgers J, Boucher H, Mori S, Peng K, Wang L. The dialectical self-concept: Contradiction, change, and holism in East Asian cultures. Personality and Social Psychology Bulletin. 2009;35:29–44. doi: 10.1177/0146167208325772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spencer-Rodgers J, Peng K, Wang L, Hou Y. Dialectical self-esteem and East–West differences in psychological well-being. Personality and Social Psychology Bulletin. 2004;30:1416–1432. doi: 10.1177/0146167204264243. [DOI] [PubMed] [Google Scholar]
- Spiegel D, Bloom JR, Kraemer HC, Gottheil E. Effect of psychosocial treatment on survival of patients with metastatic breast cancer. Lancet. 1989;2:888–891. doi: 10.1016/s0140-6736(89)91551-1. [DOI] [PubMed] [Google Scholar]
- Suh E, Diener E, Oishi S, Triandis H. The shifting basis of life satisfaction judgments across cultures: Emotions versus norms. Journal of Personality and Social Psychology. 1998;74:482–493. [Google Scholar]
- Tsai JL, Knutson B, Fung HH. Cultural variation in affect valuation. Journal of Personality and Social Psychology. 2006;90:288–307. doi: 10.1037/0022-3514.90.2.288. [DOI] [PubMed] [Google Scholar]
- Uchida Y, Norasakkunkit V, Kitayama S. Cultural constructions of happiness: Theory and empirical evidence. Journal of Happiness Studies. 2004;5:223–239. [Google Scholar]
- Watson D, Clark L, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology. 1988;54:1063–1070. doi: 10.1037//0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- Weisz J, Rothbaum F, Blackburn TC. Standing out and standing in: The psychology of control in America and Japan. American Psychologist. 1984;39:955–969. [Google Scholar]
- Yik M. Culture, gender, and the bipolarity of momentary affect. Cognition and Emotion. 2007;21:664–680. [Google Scholar]
- Zautra A, Reich J, Davis M, Potter P, Nicolson N. The role of stressful events in the relationship between positive and negative affects: Evidence from field and experimental studies. Journal of Personality. 2000;68:927–951. doi: 10.1111/1467-6494.00121. [DOI] [PubMed] [Google Scholar]