

Abstract
Objective
To examine whether overlapping cognitive deficits exist in currently drug-abstinent chronic methamphetamine (MA) abusers and schizophrenia (SZ) patients.
Background
Both SZ and chronic MA abuse are associated with frontostriatal disruption as well as deficits in cognitive control such as selective attention. To identify overlapping cognitive profiles, we compared performance of the two groups on the Stroop attention task.
Method
Data were analyzed from 69 MA abusers who had been MA-abstinent for differing periods of time and from 23 SZ patients and 38 non-substance-abusing controls.
Results
The MA abusers in early abstinence displayed more Stroop interference than the SZ patients (p= 0.004), long-term abstinent MA abusers (p= 0.009), and controls (p = 0.002). In the MA abusers, the magnitude of Stroop interference correlated positively with longer drug use [p = 0.01] and negatively with longer drug abstinence [p= 0.04]. No correlations were found between psychotic symptoms and task performance.
Conclusions
On this task of attentional selection, only the MA abusers in early stages of abstinence showed performance deficits compared to controls. More research is needed to further elucidate overlapping patterns between MA abuse and SZ.
Keywords: schizophrenia, methamphetamine, selective attention, Stroop, cognition
Introduction
In the process of everyday functioning, human beings are confronted with many objects and events to which they must respond. Selection of task-relevant information is a critical element of successful behavior, and requires the engagement of top-down cognitive control mechanisms. Cognitive control can be defined as the ability to adapt behavior flexibly to current demands, by engaging attention to task-relevant information over time in the face of interference or competition from irrelevant information 1. Deficits in cognitive control have been documented in a number of clinical populations, including those with psychiatric disorders such as schizophrenia (SZ) 2-8 and those with long-term stimulant abuse, including methamphetamine (MA) 9-15.
In addition to deficits in cognitive control, both SZ patients and MA abusers share a similar behavioral and neural profile, in that both groups 1) report hallucinations and delusions, 2) exhibit signs of distractibility, and 3) display altered patterns of neural activation that involve dopamine-rich fronto-striatal brain regions 16-18. Given this overlapping profile across numerous domains, including cognition, it is surprising that relatively few studies have directly compared the two groups 19. As both MA abuse and SZ are linked to abnormalities within the dopamine system, the identification of overlapping as well as unique patterns between the two groups may give rise to a better understanding of the neural substrates involved in psychosis and cognitive deficits linked to the dopamine system.
Given that cognitive control deficits have been reported in both SZ patients and MA abusers, it was of specific interest to us to compare cognitive performance between the two groups 8, 15, 20-23. Many findings of reduced cognitive control have been linked to abnormal prefrontal function and reduced context processing in SZ and MA abuse 2, 8, 10, 14, 15, 20, 24-26. Although cognitive deficits have been linked to psychiatric symptoms and functional outcome in patients with SZ 27-29, less work has been carried out in substance abuse. Current models of addiction propose that deficits in behavioral regulation and cognitive control may contribute to habitual and sustained drug abuse 30. For example, substance abusers may be less able to engage cognitive control to overcome automatic, prepotent response tendencies (compulsive drug use), and are thus less likely to carry out behaviors associated with long-term rewards and positive outcomes (abstaining from drug use).
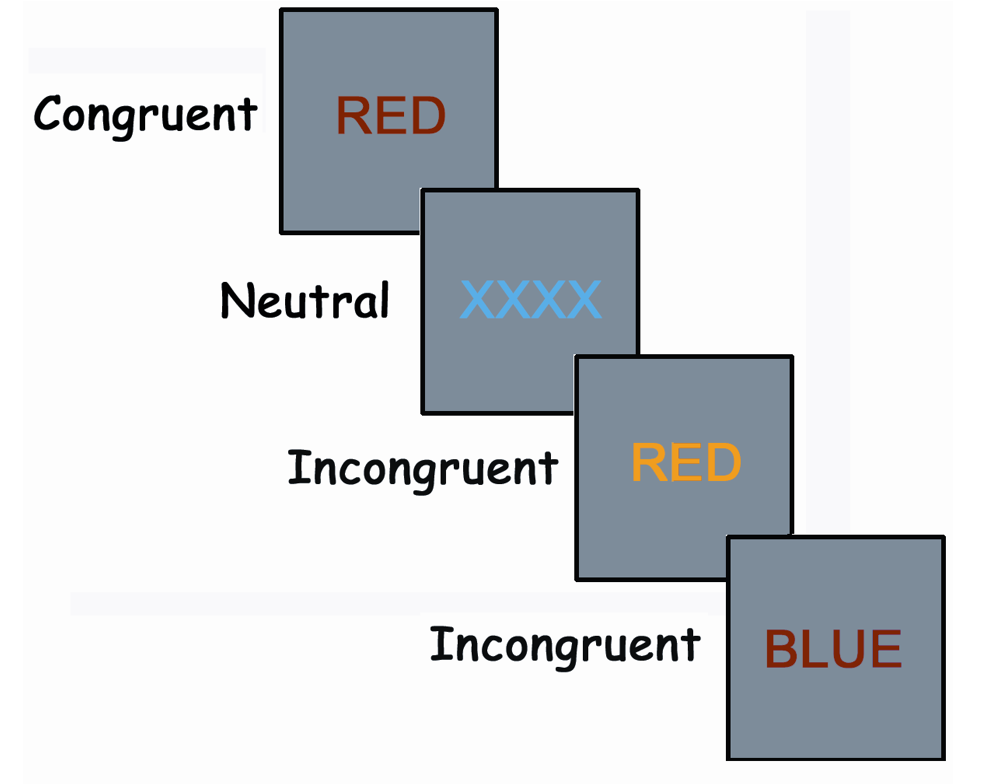
A number of tasks measure the ability to exert cognitive control, including the widely validated test of attentional selection, the Stroop color-word task. In the computerized single-trial version of the Stroop color-word task that we used, participants are presented with names of colors (eg, RED, GREEN, BLUE, YELLOW) that are printed in font colors that either match the word meaning (eg, RED printed in red ink) or are in conflict with the word meaning (eg, RED printed in blue ink). Participants are instructed to name the font color of the word that appears on the screen, and to ignore the meaning of the word. Thus, the Stroop task measures ability to attend to task-relevant information (font color) and override a prepotent but irrelevant task response (reading the word rather than naming the color) 31-33. Although multiple versions of the Stroop task are available 34, 35, we chose to administer the computerized single- trial version because 1) more precise reaction times (RTs) can be recorded in milliseconds; 2) RTs are not summed across a large stimulus set, thus controlling for outliers; 3) errors can be recorded for individual stimuli; and 4) single-word stimuli can be presented without distractors that may impact attentional performance in clinical populations over and above a potential effect of response interference 35, 36.
To measure overlapping cognitive patterns between long-term MA abusers during differing periods of MA abstinence, and SZ patients, we combined previously published behavioral data from studies that compared 69 currently drug-abstinent MA-dependent subjects to controls, with previously published data from 23 subjects with SZ 22, 23, 37, 38. All data reported in the current study were generated using the same computerized single-trial version of the Stroop attention task, with identical experimental parameters (e.g., stimulus timing, display size). Our hypotheses were: 1) Stroop interference effects would not differ between the SZ patients and matched controls (consistent with Salo, Robertson, and Nordahl39), and 2) we would find increased Stroop RT interference effects in the MA abusers 22, 37
Although early Stroop studies conducted in SZ patients did report increased Stroop effects, many of them used a card version that presented multiple words in a “cluttered field display” 40-43. In the card version, participants are presented with a series of cards containing 50-100 stimuli from one condition only (eg, incongruent stimuli) and are asked to name the ink color of each stimulus without stopping. The total time per card is the measure of performance 44. Other studies conducted since have demonstrated that the form of the Stroop task administered can affect the magnitude of Stroop interference in both SZ patients 36 and healthy controls 35. Because we collected our data with a single-trial Stroop design, we predicted no differences in Stroop interference between the SZ patients and controls 39, 45, 46. Furthermore, we predicted that the short-term MA-abstinent abusers would display more interference than the SZ patients. We based these predictions on the acute neurotoxic effects of MA on the anterior cingulate cortex and the prefrontal cortex that appear early in sobriety 47, 48. We also predicted positive correlations in the MA abusers between the magnitude of Stroop RT interference and years of abuse. Although our previous studies have not revealed a pattern of increased interference between SZ patients and controls, we analyzed the relationship between duration of illness and Stroop interference among the SZ patients as an analogous variable to duration of drug use in the MA abusers.
Materials and Methods
Subjects
The data in this paper were pooled from our previously published studies. Thus, the recruitment methods described are those that we used for all the groups in the original studies.
MA Abusers
We recruited all 69 MA-dependent subjects (28 males and 41 females) through outpatient substance abuse treatment centers. Of the total, 41 had not used MA for between 3 weeks and 6 months prior to the study, and 28 had not used MA for at least 1 year prior to study.
The short- and long-term abstinent MA abusers did not differ from each other in age [F (1, 67) = 1.14; p = 0.29], years of MA use [F < 1], education [F < 1], or premorbid IQ as determined by the National Adult Reading Test (NART) [F < 1] (Table 1). The combined MA group did not differ significantly in age from either the controls [F < 1] or the SZ patients [p = 0.10]. However, additional analyses revealed that the long-term abstinent group was slightly older than the controls [p = 0.043]. There was also a significant age difference between the controls and SZ patients [F (1, 56) = 8.03; p = 0.006]. There was a significant group difference in education levels [F (3,128) = 10.9; p = < 0.0001], with the controls having more education than the short-term abstinent group (mean= 12.6 years; SD=1.8), the long-term abstinent group (mean= 12.6; SD=1.6) and SZ subjects (mean= 12.8; SD=1.7).
Table 1. Demographic Characteristics of Participants.
| Control Subjects | Recent Abstinent MA Abusers | Distant Abstinent MA Abusers | SZ Patients | |
|---|---|---|---|---|
| (n = 38) | (n = 41) | (n =28) | (n=23) | |
| Age, years, mean (SD) | 33.8 (9.3) | 36.2 (8.9) | 38.4 (7.7) † | 40.0 (8.3) †† |
| Females | 17 | 22 | 19 | 6 |
| Education, y, mean (SD) | 14.5 (2.1) | 12.6 (1.8) †† | 12.8 (1.7) †† | 12.8 (1.7) †† |
| NART score | 114.0 (7.3) | 107.0 (5.3) †† | 106.9 (5.7) †† | ----- |
| Right-handed | 36 | 39 | 26 | 21 |
Significantly different from control group at p < 0.05
Significantly different from control group at p < 0.01
MA indicates methamphetamine; SZ, schizophrenia; NART, National Adult Reading Test.
All 69 MA-abusing subjects had been diagnosed with MA dependence by the Structured Clinical Interview for DSM Disorders (SCID) and had been drug-abstinent for a minimum of 3 weeks49 (Table 2). Random urine screens were performed at the referring sites to verify drug abstinence, and none of the screens yielded positive results. Exclusionary criteria were 1) a history of significant head trauma or neurological injury, 2) a co-occurring non-substance-related Axis I disorder, or 3) substance dependence other than MA (except nicotine) within the past year, or alcohol abuse within the past 5 years.
Table 2. Substance Use Characteristics of Abstinent Methamphetamine Abusers.
| Recent Abstinent | Distant Abstinent | |
|---|---|---|
| (n = 41) | (n = 28) | |
| Duration, years, mean (SD) | 14.2 (8.4) | 13.3 (6.7) |
| Months abstinent, mean (SD) | 2.7 (1.6) | 51.9 (34.1) †† |
| Age of first use, years, mean (SD) | 19.3 (5.2) | 18.8 (7.4) |
| Tobacco smokers | 24 | 22 |
Significantly different at p < 0.01
MA indicates methamphetamine.
SZ Patients
The SZ group included 23 patients, 21 with schizophrenia and 2 with schizoaffective disorder. The data from 2 male patients were excluded from the analysis because of an excessive number of errors on the Stroop task—more than 25%. The exclusion of these 2 patients did not significantly alter the demographic distribution.
All of the SZ patients had been diagnosed according to DSM-IV criteria, were medicated, and had used the same neuroleptic medication for at least 2 months before participating in the study, and at a fixed dosage for at least 2 weeks (Table 3). The SZ patients were interviewed by a psychiatrist and underwent an abbreviated version of the Structured Clinical Interview for DSM Disorders. All of the SZ patients were administered the Scales for the Assessment of Positive and Negative Symptoms (SAPS/SANS) interviews to assess their psychiatric symptoms. Exclusionary criteria for this group were 1) a history of significant head trauma or neurological injury, 2) co-existing Axis II disorder, and 3) a history of drug or alcohol abuse within the past year.
Table 3. Symptom and Medication Data from the 23 Schizophrenia Subjects.
| Symptoms | ||
|---|---|---|
| Onset of illness (age) | 24.5 (±7.3) | |
| Chronicity (years) | 15.9 (±9.1) | |
| SAPS rating (mean) | 17.8 (±14.9) | |
| Medication | Number of Patients | Mean Dose |
|---|---|---|
| Quetiapine | 7 | 255 mg |
| Sertindole | 3 | 18.6 mg |
| Clozapine | 5 | 305 mg |
| Risperidone | 2 | 8 mg |
| Haloperidol | 3 | 7.5 mg |
| Valproic acid | 2 | 1500 mg |
| Chlorpromazine | 1 | 1500 mg |
| Thioridazine | 1 | 125 mg |
| Loxapine | 1 | 25 mg |
| Thiothixene | 1 | 20 mg |
| Benzodiazepenes | 3 | --- |
| Anticholinergics | 4 | --- |
Note: The data from 2 patients were excluded due to excessive errors
SAPS indicates Scale for Assessment of Positive Symptoms.
Controls
We recruited 38 non-substance using controls (21 males and 17 females) from the surrounding community. Exclusionary criteria determined from the Structured Clinical Interview for DSM Disorders were 1) a history of significant head trauma or neurological injury, 2) an Axis I disorder, 3) a history of drug or alcohol abuse within the past year, and 4) a family history of psychiatric illness.
All study participants reported normal color vision and had normal or corrected-to-normal visual acuity. They signed informed consent and were paid a modest stipend for participating in the study.
Apparatus
Stimuli were presented on a 14″ VGA color monitor. A personal computer controlled stimulus presentation and data collection. Voice responses were recorded via a voice-operated relay connected to the computer.
Stimuli
We used 4 colors: red, green, blue, and yellow. For the incongruent stimuli, we presented each of the 4 color names on the computer screen in each of the 3 other font colors. For the congruent stimuli, we displayed each of the 4 color names in its own font color. The neutral stimuli consisted of strings of XXXXs displayed in one of the 4 colors. All words were in upper-case letters and subtended 1 vertical degree. The width of each word display varied as a function of the word presented (range 3-6 letters; approximately 2.4 - 5.4 visual degrees). Supplemental Digital Content 1 illustrates the color and word combinations.
Procedure
Subjects were instructed to name the font color while ignoring the word itself. They were told to avoid a speed/accuracy tradeoff. Each trial began with a blank screen, followed by the word stimulus at the center of the screen. The onset of the subject's voice triggered the voice-operated relay switch (recorded by the computer to the nearest msec) and terminated the stimulus display on the screen. The experimenter then typed in the first letter to record the subject's response. The fixed response stimulus interval (RSI) was 494 milliseconds (msec). There were 2 blocks of trials, each composed of 162 stimuli: 58 neutral, 54 congruent, and 50 incongruent. An introductory practice block was not included in the analysis.
Data Analysis
Median RTs for every condition were computed for each subject. Only correct responses were included in the RT analyses. Medians were used instead of means, to reduce the influence of outlier responses, which can exaggerate group differences, especially in patient studies 50. Analysis of variance procedures for repeated measures were used to analyze the data in a 4 × 3 mixed design with “group” as a between-subjects factor (short-term abstinent vs. long-term abstinent vs. SZ vs. controls) and “word type” (incongruent vs. neutral vs. congruent) as the within-subjects factor. Further analyses were conducted to examine error responses as well as speed-accuracy patterns. Planned comparisons of interference (median incongruent RT minus median neutral RT) and facilitation (median neutral RT minus median congruent RT) were performed.
Results
Reaction Time Analysis
Analyses revealed main effects of group [F (3, 126) = 10.47, p > 0.0001] and Stroop word type [F (2,252) = 588.11, p < 0.001], as well as a significant interaction between group and word type [F (6,242) = 4.87, p < 0.001]. Planned analyses revealed that interference effects (incongruent vs. neutral) were greater in the short-term abstinent MA abusers (177 msec) than in the controls (130 msec) [p = 0.002], SZ patients (120 msec) [p = 0.004], and long-term abstinent MA abusers (131msec) [p = 0.009]. RT interference effects did not differ significantly between the long-term abstinent MA abusers and the SZ patients [p = 0.58], between the long-term abstinent MA abusers and controls [p = 0.95], or between the SZ patients and controls [p = 0.52]. No gender differences emerged within the MA abusers (p = 0.33) or within the controls (p = 0.27). We performed analyses of covariance (ANCOVA) controlling for differences in baseline RT, education, and parental education scores. The group differences in interference endured when baseline RT, age, and education were used as covariates. We examined facilitation effects (neutral vs. congruent); no significant group by Stroop interactions emerged [F (3,126) = 1.39; p=0.25]. Specifically, all groups showed the same pattern of faster RTs to the congruent stimuli than to the neutral stimuli.
Error Analyses
Although error trials were not included in the RT analyses, further analyses examined the effect of error responses on Stroop effects (Table 4). All 4 groups made significantly more errors in the incongruent condition (8%) than the neutral condition (1%). The error rates did not differ among the 4 groups [F < 1]. Analyses revealed no evidence of a speed-accuracy trade-off for any of the 4 groups [short-term abstinent MA abusers: r=0.19, p= 0.23; long-term abstinent MA abusers; r=0.24, p= 0.21; SZ; r = 0.04, p= 0.85; controls; r=0.009, p = 0.96]. In fact, among the 69 MA abusers, there was a slight trend for those subjects with faster RTs to make fewer conflict errors than those with longer RTs.
Table 4. Median Reaction Times and % Accuracy for Within-trial Stroop Conditions Across Groups.
| Reaction Time in msec (SD) | % Errors | |
|---|---|---|
| Controls (n=38) | ||
| Incongruent | 757 (94.0) | 0.09 (.09) |
| Neutral | 627 (72.1) | 0.01 (.02) |
| Interference | 130 | |
| Baseline reaction time | 664 (104.8) | |
| Short-term Abstinent MA Abusers (n=41) | ||
| Incongruent | 852 (133.8) | 0.10 (.09) |
| Neutral | 675 (87.9) | 0.01 (.01) |
| Interference | 177 †† | |
| Baseline reaction time | 724 (138.4) | |
| Long-term Abstinent MA Abusers (n=28) | ||
| Incongruent | 780 (111.4) | 0.07 (.04) |
| Neutral | 649 (63.6) | 0.01 (.01) |
| Interference | 131 | |
| Baseline reaction time | 684 (108.1) | |
| SZ Patients (n=23) | ||
| Incongruent | 900 (200.6) | 0.07 (.07) |
| Neutral | 780 (150.9) | 0.02 (.02) |
| Interference | 120 | |
| Baseline reaction time | 808 (174) | |
Significantly different from control group and distant abstinent MA abusers at p < 0.01
MA indicates methamphetamine; SZ, schizophrenia.
Correlations with Symptoms and Drug Use Patterns
Given the range of symptoms in any study of psychiatric disorders, we wanted to examine whether drug use patterns and psychiatric symptoms correlated with cognitive performance in our 69 MA abusers and 23 SZ patients. Given our previously published finding of a relationship between duration of drug abstinence and cognitive performance22, we examined whether a similar correlation existed in our current expanded data set of MA abusers. Consistent with our previous findings, regression analyses in the MA abusers revealed a positive correlation between Stroop interference and duration of MA use [r=0.30; p = 0.01] and a negative correlation with months of MA abstinence [r=0.25; p= 0.03]. In other words, the MA abusers with longer periods of drug use performed worse on the task, while the MA abusers with extended periods of MA sobriety performed better. Similar analyses in the 23 SZ patients using duration of illness as a regression variable failed to reach significance [r= 0.13; p= 0.54], perhaps because of the limited sample size.
As both the MA abusers and SZ patients reported psychotic symptoms, we wanted to examine whether these symptoms correlated with their cognitive performance. Among the 69 MA abusers, 68% (n=47) reported a history of MA-induced psychotic symptoms, including paranoid delusions and hallucinations. Although weak correlations have been observed in SZ patients between positive symptoms (eg, delusions and hallucinations) and cognitive processes, less is known about such a relationship with drug-induced psychoses 51. Given that such a large percentage of MA abusers experience drug-induced psychosis, it was of interest to examine this relationship.
We observed no difference in Stroop interference effects between our MA abusers with a history of MA-induced psychosis and those with no history (F (1, 67) = 0.14; p= 0.71). Furthermore, we examined the correlation between Stroop interference and the frequency of MA-induced psychotic episodes among those MA abusers with a history of MA-induced psychosis. We did not find a significant correlation between the frequency of MA-induced psychotic episodes and Stroop interference (r=0.008, p= 0.96). We then examined the Scales for the Assessment of Positive Symptoms scores from our 23 SZ patients to determine if any relationship existed between scores of positive symptoms (delusions and hallucinations) and performance on the Stroop task. Analyses revealed no correlation (r= 0.112, p= 0.62). As these SZ patients were relatively high-functioning, they did not have prominent negative symptoms.
Discussion
We found that the MA abusers in early stages of abstinence (3 weeks - 6 months) exhibited greater deficits in attentional selection and cognitive control than the SZ subjects, controls, and MA abusers who had stopped abusing MA longer than 1 year prior to the study. Significant correlations were observed between duration of MA use, time of sobriety, and performance on the Stroop task. Longer periods of MA abstinence appeared to improve performance, while longer durations of use correlated with greater task deficits. These findings are consistent with other published studies that have reported cognitive deficits during the early periods of MA abstinence 52, 53. Importantly, although the short-term abstinent MA abusers displayed significantly greater RT interference than the long-term abstinent MA abusers, they did not differ on baseline RT, demonstrating that overall slowing is not the underlying mechanism producing the group differences. Furthermore, it was only the SZ patients who were significantly slower than all the other subjects, yet their pattern of performance on the Stroop task was similar to both the controls and the long-term abstinent MA abusers.
It is perhaps unexpected that the MA abusers in early abstinence would perform worse than the SZ patients. However, a careful review of the Stroop literature suggests that studies that have reported increased RT Stroop interference in patients with SZ used a different form of the Stroop task (i.e., card version), which may have placed additional cognitive demands on the SZ patients. (For a review, see Henik and Salo.54) The majority of single-trial Stroop studies have actually reported equivalent Stroop RT interference between SZ patients and controls. 31, 45, 55-58 In several of these studies, SZ patients showed more facilitation than normal controls, but no difference in RT interference 31, 59. Similar findings of equivalent Stroop RT interference in SZ patients have also been reported in priming experiments that used Stroop stimuli, 38, 46, 60, 61 and in neuroimaging studies 62, 63. Other studies that have measured top-down behavioral control have also failed to find deficits in SZ patients 64. In a study that used the Attention Network Test, SZ patients displayed decreased alerting efficiency but no deficits in top-down control. Thus, the lack of increased Stroop RT interference observed in our study is indeed consistent with the literature.
Our data cannot answer why the short-term abstinent MA abusers exhibited greater RT interference than the SZ patients. Dysfunction has been observed within the anterior cingulate and prefrontal cortices of both groups; thus, one might predict similar performance deficits 8, 15, 21, 25, 62, 65, 66. One possible mechanism for the greater deficits in the short-term abstinent MA group than the SZ patients is that the acute neurotoxic effects of MA early in abstinence might have more profound effects on the anterior cingulate cortex and prefrontal cortex.45, 47, 67 This could explain the differences in Stroop RT interference observed between the short- and long-term abstinent MA abusers. As mentioned, our 23 SZ patients were relatively high-functioning. It is quite possible that more severely ill patients might have exhibited more pronounced deficits on the Stroop task. Nonetheless, our patients had been ill for an average of 16 years, and their average age was 40. More studies are needed to explore this issue.
We found no significant relationships between psychotic symptoms and cognitive performance across the clinical groups. These findings are consistent with findings in the SZ literature, in which weak correlations have been observed between cognitive performance and symptoms 51. Thus, neither the symptoms of schizophrenia nor the drug-induced psychotic symptoms associated with long-term MA use appear to underlie our patients' cognitive patterns. More work is needed to examine this issue in substance abuse. It is important to keep in mind that the data in this study can address performance on only one aspect of attentional function, the ability to attend selectively and suppress a prepotent response within each trial. We do not claim that these results are generalizable to a broader range of cognitive processes.
Limitations
Among our 69 MA abusers, it is possible that a history of drug abuse other than MA—a common comorbidity in such individuals—could have contributed to the cognitive patterns that we observed. To minimize this risk, we studied patients whose primary drug of choice was MA, with no dependence on other drugs beside nicotine, and who had not abused alcohol for at least 5 years prior to the study. It is also possible that differences in age and education could have impacted the results; however, statistical analyses co-varying for these demographic differences did not alter the findings.
Conclusion
Although there are overlapping clinical and cognitive similarities between MA abusers and SZ patients, few studies have directly measured attentional performance between these 2 groups.19 A major strength of our study is that all 130 subjects across the 4 groups were tested on exactly the same computerized version of the Stroop attention task, using identical experimental parameters. We did not find that general slowing was a source of the group differences. Instead, for our task, the residual effects of MA during the first 6 months of abstinence seem to be causing the most pronounced cognitive deficits. We did not detect a relationship between psychotic symptoms and cognitive performance, although both groups reported such symptoms. Neither the drug-induced psychotic symptoms in the MA abusers nor the severity of symptoms in the SZ patients appeared to correlate with performance.
Although this was not designed as a clinical study, the improved attentional performance in the group who had stopped abusing MA for at least 12 months suggests that they can make adaptive changes. Specifically, their greater ability than the short-term abstinent MA group to shift attention from a prepotent response in the Stroop task may correlate with their ability to resist the prepotent response to use illicit drugs. Such cognitive improvements have the potential to be used to predict treatment outcome. The pattern of cognitive performance in the SZ patients is more difficult to interpret from a clinical perspective. Because our 23 SZ patients were high-functioning, it is difficult to generalize across the disorder. Further studies using broader measures of cognitive function in larger groups of MA and SZ patients are needed to assess their overlapping cognitive patterns.
Supplementary Material
{kind=link}
Acknowledgments
Preparation of this article was supported by Grant Awards MH11706, DA16293, and DA023029 to R.S.
Footnotes
The authors have no conflicts of interest to disclose.
References
- 1.Botvinick MM, Braver TS, Barch DM, et al. Conflict monitoring and cognitive control. Psychol Review. 2001;108:624–652. doi: 10.1037/0033-295x.108.3.624. [DOI] [PubMed] [Google Scholar]
- 2.Barbalat G, Chambon V, Franck N, et al. Organization of cognitive control within the lateral prefrontal cortex in schizophrenia. Arch Gen Psychiatry. 2009;66:377–386. doi: 10.1001/archgenpsychiatry.2009.10. [DOI] [PubMed] [Google Scholar]
- 3.Eisenberg DP, Berman KF. Executive function, neural circuitry, and genetic mechanisms in schizophrenia. Neuropsychopharmacology. 2010;35:258–277. doi: 10.1038/npp.2009.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ragland JD, Laird AR, Ranganath C, et al. Prefrontal activation deficits during episodic memory in schizophrenia. Am J Psychiatry. 2009;166:863–874. doi: 10.1176/appi.ajp.2009.08091307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cohen JD, Botvinick M, Carter CS. Anterior cingulate and prefrontal cortex: who's in control? Nat Neurosci. 2000;3:421–423. doi: 10.1038/74783. [DOI] [PubMed] [Google Scholar]
- 6.Kerns JG, Cohen JD, MacDonald AW, 3rd, et al. Anterior cingulate conflict monitoring and adjustments in control. Science. 2004;303:1023–1026. doi: 10.1126/science.1089910. [DOI] [PubMed] [Google Scholar]
- 7.Kerns JG, Cohen JD, Stenger VA, et al. Prefrontal cortex guides context-appropriate responding during language production. Neuron. 2004;43:283–291. doi: 10.1016/j.neuron.2004.06.032. [DOI] [PubMed] [Google Scholar]
- 8.MacDonald AW, 3rd, Carter CS. Event-related FMRI study of context processing in dorsolateral prefrontal cortex of patients with schizophrenia. J Abnorm Psychol. 2003;112:689–697. doi: 10.1037/0021-843X.112.4.689. [DOI] [PubMed] [Google Scholar]
- 9.Nordahl TE, Salo R, Leamon M. Neuropsychological effects of chronic methamphetamine use on neurotransmitters and cognition: a review. J Neuropsychiatry Clin Neurosci. 2003;15:317–325. doi: 10.1176/jnp.15.3.317. [DOI] [PubMed] [Google Scholar]
- 10.Paulus MP, Hozack N, Frank L, et al. Decision making by methamphetamine-dependent subjects is associated with error-rate-independent decrease in prefrontal and parietal activation. Biol Psychiatry. 2003;53:65–74. doi: 10.1016/s0006-3223(02)01442-7. [DOI] [PubMed] [Google Scholar]
- 11.Sim T, Simon SL, Domier CP, et al. Cognitive deficits among methamphetamine users with attention deficit hyperactivity disorder symptomatology. J Addict Dis. 2002;21:75–89. doi: 10.1300/j069v21n01_07. [DOI] [PubMed] [Google Scholar]
- 12.Simon SL, Domier CP, Sim T, et al. Cognitive performance of current methamphetamine and cocaine abusers. J Addict Dis. 2002;21:61–74. doi: 10.1300/j069v21n01_06. [DOI] [PubMed] [Google Scholar]
- 13.Kalechstein AD, Newton TF, Green M. Methamphetamine dependence is associated with neurocognitive impairment in the initial phases of abstinence. J Neuropsychiatry Clin Neurosci. 2003;15:215–220. doi: 10.1176/jnp.15.2.215. [DOI] [PubMed] [Google Scholar]
- 14.Monterosso JR, Aron AR, Cordova X, et al. Deficits in response inhibition associated with chronic methamphetamine abuse. Drug Alcohol Depend. 2005;79:273–277. doi: 10.1016/j.drugalcdep.2005.02.002. [DOI] [PubMed] [Google Scholar]
- 15.Salo R, Ursu S, Buonocore MH, et al. Impaired prefrontal cortical function and disrupted adaptive cognitive control in methamphetamine abusers: a functional magnetic resonance imaging study. Biol Psychiatry. 2009;65:706–709. doi: 10.1016/j.biopsych.2008.11.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Scott JC, Woods SP, Matt GE, et al. Neurocognitive effects of methamphetamine: a critical review and meta-analysis. Neuropsychol Rev. 2007;17:275–297. doi: 10.1007/s11065-007-9031-0. [DOI] [PubMed] [Google Scholar]
- 17.Baicy K, London ED. Addiction. Vol. 102. Abingdon, England: 2007. Corticolimbic dysregulation and chronic methamphetamine abuse; pp. 5–15. [DOI] [PubMed] [Google Scholar]
- 18.Meredith CW, Jaffe C, Ang-Lee K, et al. Implications of chronic methamphetamine use: a literature review. Harv Rev Psychiatry. 2005;13:141–154. doi: 10.1080/10673220591003605. [DOI] [PubMed] [Google Scholar]
- 19.Jacobs E, Fujii D, Schiffman J, et al. An exploratory analysis of neurocognition in methamphetamine-induced psychotic disorder and paranoid schizophrenia. Cogn Behav Neurol. 2008;21:98–103. doi: 10.1097/WNN.0b013e31816bdf90. [DOI] [PubMed] [Google Scholar]
- 20.Barch DM, Carter CS, MacDonald AW, 3rd, et al. Context-processing deficits in schizophrenia: diagnostic specificity, 4-week course, and relationships to clinical symptoms. J Abnorm Psychology. 2003;112:132–143. [PubMed] [Google Scholar]
- 21.Carter CS, MacDonald AW, 3rd, Ross LL, et al. Anterior cingulate cortex activity and impaired self-monitoring of performance in patients with schizophrenia: an event-related fMRI study. Am J Psychiatry. 2001;158:1423–1428. doi: 10.1176/appi.ajp.158.9.1423. [DOI] [PubMed] [Google Scholar]
- 22.Salo R, Nordahl TE, Galloway GP, et al. Drug abstinence and cognitive control in methamphetamine-dependent individuals. J Substance Abuse Treat. 2009;37:292–297. doi: 10.1016/j.jsat.2009.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Salo R, Nordahl TE, Natsuaki Y, et al. Attentional control and brain metabolite levels in methamphetamine abusers. Biol Psychiatry. 2007;61:1272–1280. doi: 10.1016/j.biopsych.2006.07.031. [DOI] [PubMed] [Google Scholar]
- 24.Barch DM, Carter CS, Braver TS, et al. Selective deficits in prefrontal cortex function in medication-naive patients with schizophrenia. Arch Gen Psychiatry. 2001;58:280–288. doi: 10.1001/archpsyc.58.3.280. [DOI] [PubMed] [Google Scholar]
- 25.MacDonald AW, 3rd, Carter CS, Kerns JG, et al. Specificity of prefrontal dysfunction and context processing deficits to schizophrenia in never-medicated patients with first-episode psychosis. Am J Psychiatry. 2005;162:475–484. doi: 10.1176/appi.ajp.162.3.475. [DOI] [PubMed] [Google Scholar]
- 26.Salo R, Nordahl TE, Buonocore MH, et al. Cognitive control and white matter callosal microstructure in methamphetamine-dependent subjects: a diffusion tensor imaging study. Biol Psychiatry. 2009;65:122–128. doi: 10.1016/j.biopsych.2008.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Green MF. Cognitive impairment and functional outcome in schizophrenia and bipolar disorder. J Clin Psychiatry. 2006;67 9:3–8. discussion 36-42. [PubMed] [Google Scholar]
- 28.Carter CS, Barch DM. Cognitive neuroscience-based approaches to measuring and improving treatment effects on cognition in schizophrenia: the CNTRICS initiative. Schizophr Bull. 2007;33:1131–1137. doi: 10.1093/schbul/sbm081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ventura J, Hellemann GS, Thames AD, et al. Symptoms as mediators of the relationship between neurocognition and functional outcome in schizophrenia: a meta-analysis. Schizophr Res. 2009;113:189–199. doi: 10.1016/j.schres.2009.03.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jentsch JD, Taylor JR. Impulsivity resulting from frontostriatal dysfunction in drug abuse: implications for the control of behavior by reward-related stimuli. Psychopharmacology. 1999;146:373–390. doi: 10.1007/pl00005483. [DOI] [PubMed] [Google Scholar]
- 31.Carter CS, Robertson LC, Nordahl TE. Abnormal processing of irrelevant information in chronic schizophrenia: selective enhancement of Stroop facilitation. Psychiatry Res. 1992;41:137–146. doi: 10.1016/0165-1781(92)90105-c. [DOI] [PubMed] [Google Scholar]
- 32.Swick D, Jovanovic J. Anterior cingulate cortex and the Stroop task: neuropsychological evidence for topographic specificity. Neuropsychologia. 2002;40:1240–1253. doi: 10.1016/s0028-3932(01)00226-3. [DOI] [PubMed] [Google Scholar]
- 33.Ochsner KN, Kosslyn SM, Cosgrove GR, et al. Deficits in visual cognition and attention following bilateral anterior cingulotomy. Neuropsychologia. 2001;39:219–230. doi: 10.1016/s0028-3932(00)00114-7. [DOI] [PubMed] [Google Scholar]
- 34.MacLeod CM. Half a century of research on the Stroop effect: an integrative review. Psychol Bull. 1991;109:163–203. doi: 10.1037/0033-2909.109.2.163. [DOI] [PubMed] [Google Scholar]
- 35.Salo R, Henik A, Robertson LC. Interpreting Stroop interference: an analysis of differences between task versions. Neuropsychology. 2001;15:462–471. doi: 10.1037//0894-4105.15.4.462. [DOI] [PubMed] [Google Scholar]
- 36.Boucart M, Mobarek N, Cuervo C, et al. What is the nature of increased Stroop interference in schizophrenia? Acta Psychol. 1999;101:3–25. doi: 10.1016/s0001-6918(98)00037-7. [DOI] [PubMed] [Google Scholar]
- 37.Salo R, Nordahl TE, Possin K, et al. Preliminary evidence of reduced cognitive inhibition in methamphetamine-dependent individuals. Psychiatry Res. 2002;111:65–74. doi: 10.1016/s0165-1781(02)00111-7. [DOI] [PubMed] [Google Scholar]
- 38.Salo R, Henik A, Nordahl TE, et al. Immediate versus sustained processing in schizophrenia. J Int Neuropsychol Soc. 2002;8:794–803. doi: 10.1017/s1355617702860076. [DOI] [PubMed] [Google Scholar]
- 39.Salo R, Robertson LC, Nordahl TE. Normal sustained effects of selective attention are absent in schizophrenic patients withdrawn from medication. Psychiatry Res. 1996;62:121–130. doi: 10.1016/0165-1781(96)02804-1. [DOI] [PubMed] [Google Scholar]
- 40.Wapner S, Krus DM. Effects of lysergic acid diethylamide, and differences between normals and schizophrenics on the Stroop Color-Word Test. J Neuropsychiatry. 1960;2:76–81. [PubMed] [Google Scholar]
- 41.Abramczyk RR, Jordan DE, Hegel M. “Reverse” Stroop effect in the performance of schizophrenics. Percept Mot Skills. 1983;56:99–106. doi: 10.2466/pms.1983.56.1.99. [DOI] [PubMed] [Google Scholar]
- 42.Brebion G, Smith MJ, Gorman JM, et al. Reality monitoring failure in schizophrenia: the role of selective attention. Schizophr Res. 1996;22:173–180. doi: 10.1016/s0920-9964(96)00054-0. [DOI] [PubMed] [Google Scholar]
- 43.Hanes KR, Andrewes DG, Smith DJ, et al. A brief assessment of executive control dysfunction: discriminant validity and homogeneity of planning, set shift, and fluency measures. Arch Clin Neuropsychol. 1996;11:185–191. [PubMed] [Google Scholar]
- 44.Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol. 1935;18:643–662. [Google Scholar]
- 45.Henik A, Carter CS, Salo R, et al. Attentional control and word inhibition in schizophrenia. Psychiatry Res. 2002;110:137–149. doi: 10.1016/s0165-1781(02)00100-2. [DOI] [PubMed] [Google Scholar]
- 46.Salo R, Robertson LC, Nordahl TE, et al. The effects of antipsychotic medication on sequential inhibitory processes. J Abnorm Psychol. 1997;106:639–643. doi: 10.1037//0021-843x.106.4.639. [DOI] [PubMed] [Google Scholar]
- 47.Nordahl TE, Salo R, Natsuaki Y, et al. Methamphetamine users in sustained abstinence: a proton magnetic resonance spectroscopy study. Arch Gen Psychiatry. 2005;62:444–452. doi: 10.1001/archpsyc.62.4.444. [DOI] [PubMed] [Google Scholar]
- 48.Salo R, Buonocore MH, Leamon M, et al. Extended findings of brain metabolite normalization in MA-dependent subjects across sustained abstinence: A proton MRS study. Drug Alcohol Depend. 2011;113:133–138. doi: 10.1016/j.drugalcdep.2010.07.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.First MB, Spitzer L, Gibbon M, et al. Structured Clinical Interview for DSM-IV Axis I Disorders. New York, NY: Biometrics Research Department; 1995. [Google Scholar]
- 50.Ratcliff R. Methods for Dealing With Reaction Time Outliers. Psychol Bull. 1993;114:510–532. doi: 10.1037/0033-2909.114.3.510. [DOI] [PubMed] [Google Scholar]
- 51.Blaney PH, Millon T. Oxford sTextbook of Psychopathology. New York sNew York: Oxford University Press; 2009. [Google Scholar]
- 52.Simon SL, Dacey J, Glynn S, et al. The effect of relapse on cognition in abstinent methamphetamine abusers. J Substance Abuse Treat. 2004;27:59–66. doi: 10.1016/j.jsat.2004.03.011. [DOI] [PubMed] [Google Scholar]
- 53.Simon SL, Dean AC, Cordova X, et al. Methamphetamine dependence and neuropsychological functioning: evaluating change during early abstinence. J Studies Alcohol Drugs. 2010(71):335–344. doi: 10.15288/jsad.2010.71.335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Henik A, Salo R. Schizophrenia and the stroop effect. Behav Cog Neurosci Rev. 2004;3:42–59. doi: 10.1177/1534582304263252. [DOI] [PubMed] [Google Scholar]
- 55.Barch DM, Carter CS, Hachten PC, et al. The “benefits” of distractibility: mechanisms underlying increased Stroop effects in schizophrenia. Schizophr Bull. 1999;25:749–762. doi: 10.1093/oxfordjournals.schbul.a033416. [DOI] [PubMed] [Google Scholar]
- 56.Perlstein WM, Carter CS, Barch DM, et al. The Stroop task and attention deficits in schizophrenia: a critical evaluation of card and single-trial Stroop methodologies. Neuropsychology. 1998;12:414–425. doi: 10.1037//0894-4105.12.3.414. [DOI] [PubMed] [Google Scholar]
- 57.Taylor SF, Kornblum S, Tandon R. Facilitation and interference of selective attention in schizophrenia. J Psychiatr Res. 1996;30:251–259. doi: 10.1016/0022-3956(95)00046-1. [DOI] [PubMed] [Google Scholar]
- 58.Chen EY, Wong AW, Chen RY, et al. Stroop interference and facilitation effects in first-episode schizophrenic patients. Schizophr Res. 2001;48:29–44. doi: 10.1016/s0920-9964(00)00107-9. [DOI] [PubMed] [Google Scholar]
- 59.Barch DM, Carter CS, Perlstein W, et al. Increased stroop facilitation effects in schizophrenia are not due to increased automatic spreading activation. Schizophr Res. 1999;39:51–64. doi: 10.1016/s0920-9964(99)00025-0. [DOI] [PubMed] [Google Scholar]
- 60.Laplante L, Everett J, Thomas J. Inhibition through negative priming with Stroop stimuli in schizophrenia. Br J Clin Psychol. 1992;31(Pt 3):307–326. doi: 10.1111/j.2044-8260.1992.tb00998.x. [DOI] [PubMed] [Google Scholar]
- 61.Salo R, Henik A, Nordahl TE, et al. Time course of inhibition and facilitation in patients with schizophrenia. Cog Neuropsychiatry. 2002;7:283–300. doi: 10.1080/13546800244000003. [DOI] [PubMed] [Google Scholar]
- 62.Carter CS, Mintun M, Nichols T, et al. Anterior cingulate gyrus dysfunction and selective attention deficits in schizophrenia: [15O]H2O PET study during single-trial Stroop task performance. Am J Psychiatry. 1997;154:1670–1675. doi: 10.1176/ajp.154.12.1670. [DOI] [PubMed] [Google Scholar]
- 63.Nordahl TE, Carter CS, Salo RE, et al. Anterior cingulate metabolism correlates with stroop errors in paranoid schizophrenia patients. Neuropsychopharmacology. 2001;25:139–148. doi: 10.1016/S0893-133X(00)00239-6. [DOI] [PubMed] [Google Scholar]
- 64.Nestor PG, Kubicki M, Spencer KM, et al. Attentional networks and cingulum bundle in chronic schizophrenia. Schizophr Res. 2007;90:308–315. doi: 10.1016/j.schres.2006.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Paulus MP, Hozack NE, Zauscher BE, et al. Behavioral and functional neuroimaging evidence for prefrontal dysfunction in methamphetamine-dependent subjects. Neuropsychopharmacology. 2002;26:53–63. doi: 10.1016/S0893-133X(01)00334-7. [DOI] [PubMed] [Google Scholar]
- 66.Paulus MP, Lovero KL, Wittmann M, et al. Reduced behavioral and neural activation in stimulant users to different error rates during decision making. Biol Psychiatry. 2008;63:1054–1060. doi: 10.1016/j.biopsych.2007.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Volkow ND, Chang L, Wang GJ, et al. Loss of dopamine transporters in methamphetamine abusers recovers with protracted abstinence. J Neurosci. 2001;21:9414–9418. doi: 10.1523/JNEUROSCI.21-23-09414.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.