

Abstract
Background
Recent studies have described unique clinical and radiographic characteristics of femoral stress fractures or low-energy fractures associated with long-term bisphosphonate therapy. However, it is unclear whether these fractures require subsequent surgery after the initial treatment.
Questions/purposes
We performed a cohort analysis of bisphosphonate-associated femoral stress fractures to (1) confirm the unique clinical and radiographic findings compared with existing literature, (2) determine whether any patients with completed fractures had no preexisting transverse stress fracture lines, (3) assess the need for additional surgical procedures, and (4) determine whether the hospital length of stay (LOS) differed for patients with prophylactic fixation of stress fractures versus fixation of completed fractures.
Methods
We retrospectively reviewed 16 patients with 24 diaphyseal and subtrochanteric femoral stress fractures (14) or low-energy fractures (10) who had been on bisphosphonates for 3 to 10 years. Data included demographics, symptoms, medication history, radiographic characteristics, treatment parameters, LOS, and outcome. Minimum followup was 9 months (average, 44.0 months; median, 31 months; range, 9–112 months).
Results
All patients had clinical and radiographic findings similar to those reported in the literature. Two of four patients sustained completed fractures after radiographs failed to reveal transverse lateral fracture lines. None of the 14 prophylactically treated impending fractures progressed or required additional surgery; however, in five of 10 femurs treated after fracture completion, six additional surgeries were performed. The average hospital LOS was shorter in patients who underwent prophylactic fixation (3.8 days) than in patients treated for completed fractures (5.6 days).
Conclusions
Bisphosphonate-associated stress fractures and completed fractures are unique, possessing subtle characteristic radiographic features. Completed fractures may occur through the thickened bone in the absence of an appreciable transverse stress fracture line. Our observations suggest prophylactic reconstruction nail fixation may avoid fracture completion and may be associated with a shorter hospital LOS and less morbidity than treatment of completed fractures.
Level of Evidence
Level IV, diagnostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Electronic supplementary material
The online version of this article (doi:10.1007/s11999-011-2194-2) contains supplementary material, which is available to authorized users.
Introduction
Osteoporosis, defined as bone mineral density (BMD) of more than 2.5 SDs less than that of healthy young adults, is a major health problem in the United States [4] and commonly leads to fragility fractures of the vertebrae, wrist, and hip [15]. In addition to exercise, calcium, and vitamin D, bisphosphonates are commonly used to combat postmenopausal osteoporosis [1, 3, 14]. More than 150 million prescriptions for oral alendronate, risedronate, and ibandronate were dispensed in the outpatient setting for the period 2005 to 2009 in the United States alone [19]. Bisphosphonates reportedly increase BMD [6, 7, 11]. In the Fracture Intervention Trial, long-term bisphosphonate therapy decreased the risk of vertebral and femoral neck fractures in postmenopausal patients with severe osteoporosis [3, 6].
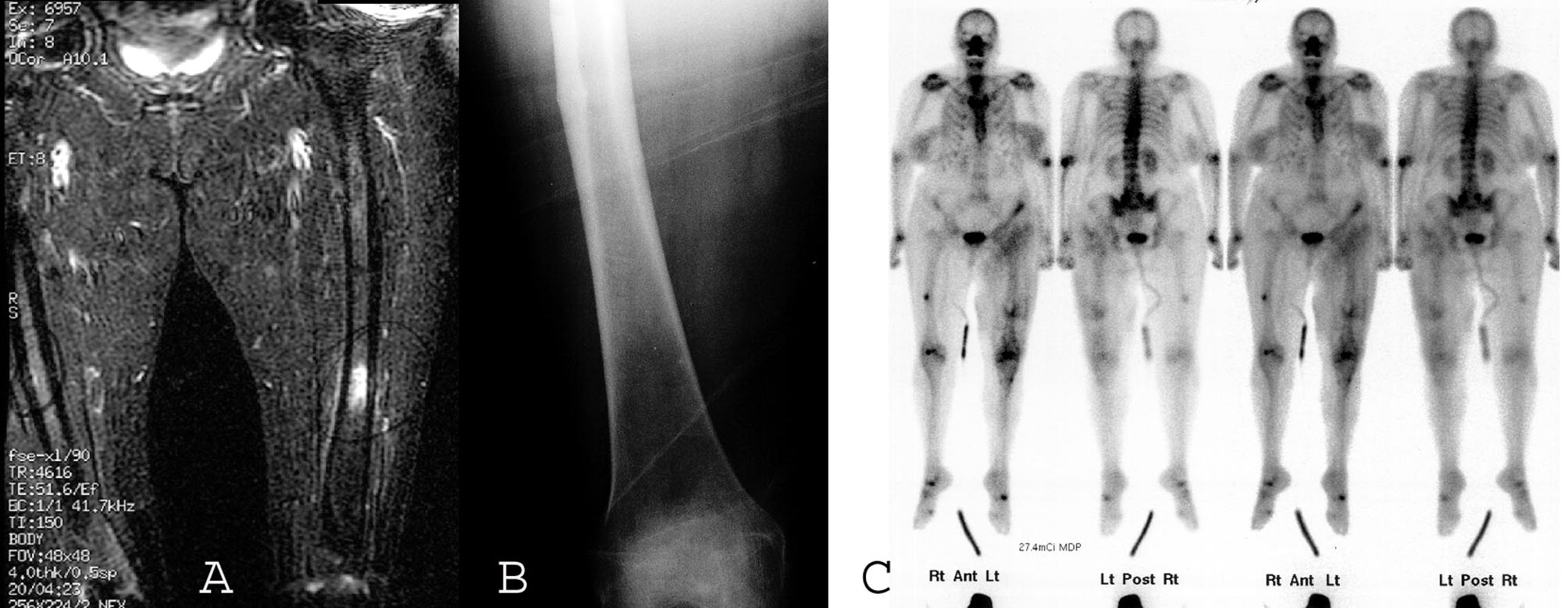
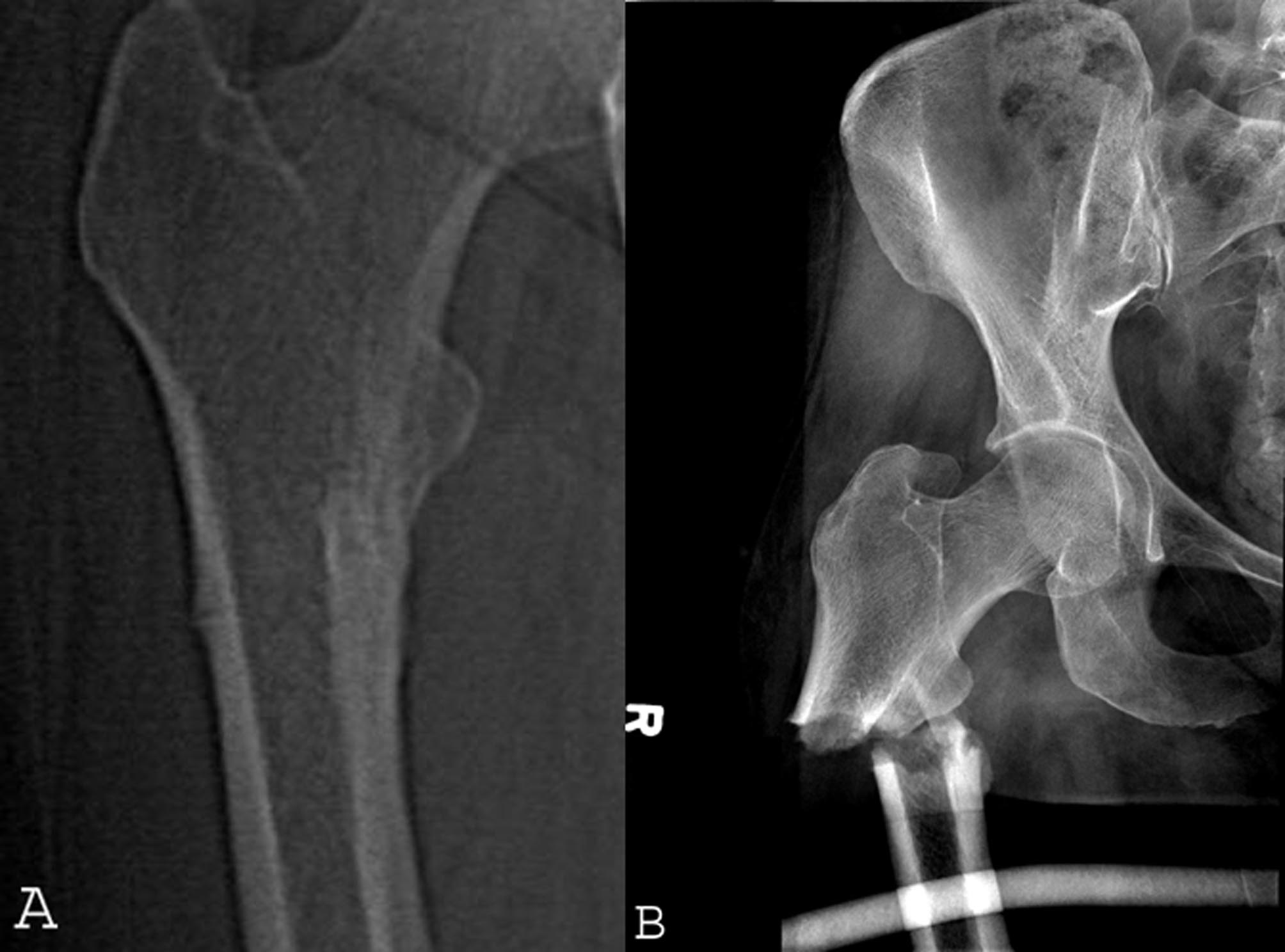
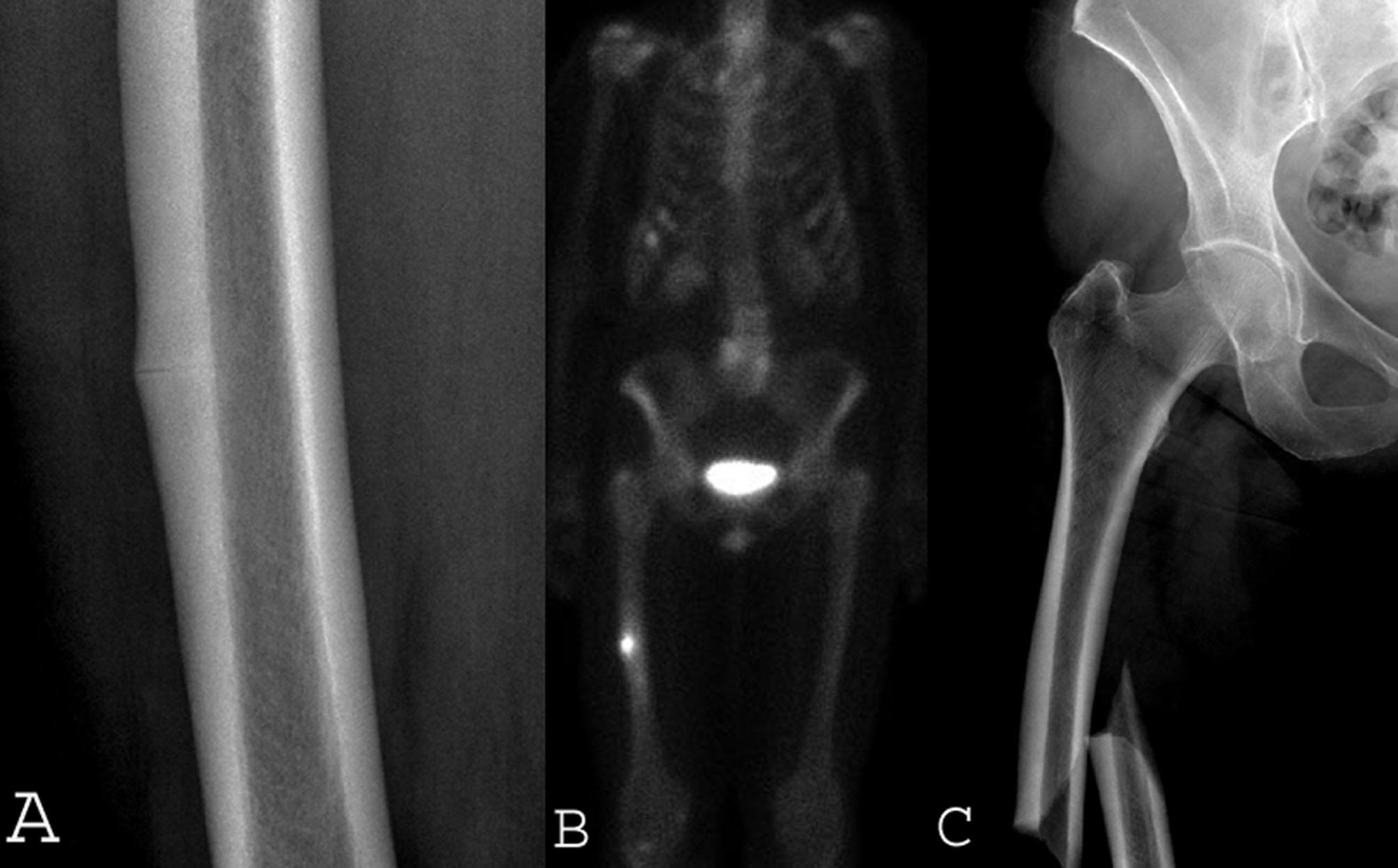
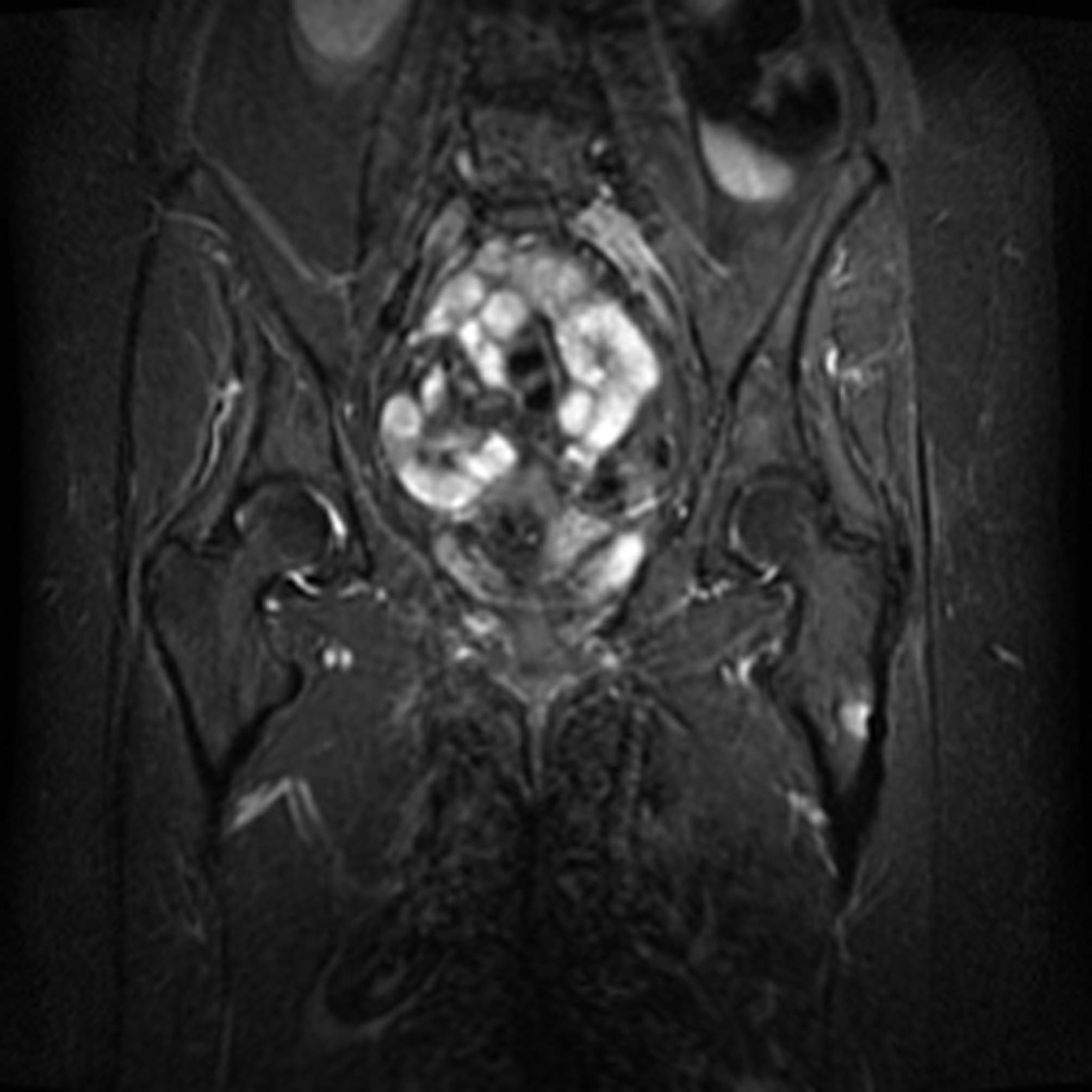
Since 2005, several reports have described patients on long-term bisphosphonate therapy who developed unusual stress fractures and/or low-energy fractures in the subtrochanteric and diaphyseal regions of the femur [2, 4, 5, 9–11, 17]. The femoral shaft is usually an uncommon site for osteoporotic fractures [5, 13]. Virtually all reported patients had been on bisphosphonate therapy for at least 3 years [2, 4, 5, 9–11], raising concerns regarding prolonged bisphosphonate therapy. The clinical and radiographic findings in these bisphosphonate-associated stress fractures are provided (Table 1). A frequently reported prodromal symptom is pain in the affected limb [9, 10]. We encountered several patients with stress fractures who were symptomatic for various lengths of time but were undiagnosed or misdiagnosed until a complete femoral fracture occurred. Our clinical experience indicated the radiographic prefracture findings in many cases were quite subtle, often consisting of an innocuous-appearing lateral cortical thickening as described by Sayed-Noor and Sjödén [16]. Koh et al. [9] reported completed fractures occurred only in those patients who had developed complete transverse stress fracture lines in the lateral cortex. This “dreaded black line” of an impending femoral stress fracture is similar to that described in the proximal anterior tibia of athletes with stress fractures from overuse [9]. The cortical thickening may obscure the hairline transverse lateral cortical stress fracture lines on plain film. The subtle nature of the radiographic findings of these stress fractures, especially those without an observable stress fracture line, led several of our colleagues and the senior author (WGW) to initially overlook their importance until progression into a completed fracture was observed, an observation contrary to the report of Koh et al. [9], who reported virtually no fracture completions without the prior existence of a transverse fracture line.
Table 1.
Literature reports of clinical and radiographic findings in bisphosphonate-associated fractures
| Study | Sex (F:M) | Age (years)* | Number of impending/completed fractures | Patients with prodromal pain | Duration of bisphosphonate use (years)* | Fractures with transverse line before fracture | Fractures with lateral cortical thickening | Number of prophylactic reconstruction nails that failed/total number treated with nail | Patients with bilateral fractures |
|---|---|---|---|---|---|---|---|---|---|
| Banffy et al. [2] | 34 F | All > 50 | 12/28 | 6.4 (3–10) | 100% | 100% | 0/6 | 0% | |
| Capeci and Tejwani [4] | 7 F | 61 (53–75) | 7 (impending) | 57.10% | 8.6 (5–13) | 100% | 0/3 | 100% | |
| Koh et al. [9] | 16 F | Median 68 (53–92) | 12/4 | 100% (of completed fractures) | 4.5 (2–7) | 100% | 100% | ||
| Kwek et al. [10] | 17 F | 66 (53–82) | 17 (completed) | 76% | 4.8 (2–8) | 100% | 100% | 53% | |
| Neviaser et al. [11] | 25 F | 69.4 | 25 (completed) | 6.2 (1–10) | 76% | 76% | |||
| Current study | 15:1 | 69.1 (51–90) | 14/10 | 100% | 6.3 (3–10) | 50% (2/4) | 96% (22/23) | 0/14 | 50% |
* Values are expressed as mean, with range in parentheses; F = female; M = male.
Our study purposes were to (1) confirm the clinical and radiographic features of long-term bisphosphonate treatment-associated stress fractures as compared with existing literature, (2) determine whether any patients with completed fractures had no preexisting transverse stress fracture lines, (3) determine the frequency of additional surgical procedures, and (4) determine whether the hospital length of stay (LOS) for prophylactic fixation of stress fractures differed from that for fixation of completed fractures.
Patients and Methods
After Institutional Review Board approval, we retrospectively reviewed the medical records of 16 patients who had 24 diaphyseal and subtrochanteric femoral stress fractures and/or completed low-energy fractures treated between January 2002 and September 2010 and who had been on bisphosphonate treatment for at least 3 years. Fifteen were personal patients of the authors; one additional patient heard of the study through a practice colleague and agreed to be included. Thirteen of the 16 patients were patients of the senior author (WGW), who maintains a comprehensive database of all surgically treated patients. We reviewed all femur fractures treated by this author from January 2002 through September 2010. He treated 400 femur fractures (excluding 16 periprosthetic fractures): 218 traumatic fractures, 74 pathologic fractures, 72 impending pathologic fractures, and 35 stress fractures (20 associated with bisphosphonate usage [13 patients] and 15 not associated with bisphosphonate usage [15 patients]). Of the 400 femur fractures, 230 primarily involved the hip region (defined as intertrochanteric level or more proximal), 166 primarily involved the remainder of the femur, and four involved both areas. We clinically and radiographically reviewed the records of the 28 patients with 35 stress fractures to determine whether there had been any patients with similar clinical histories or fracture patterns. The 13 patients (20 bisphosphonate-associated fractures) treated by the senior author plus two patients (two bisphosphonate-associated fractures) treated by the other authors plus the one patient (two bisphosphonate-associated fractures) contributed by a practice colleague comprise the study cohort (16 patients, 24 bisphosphonate-associated fractures). We made no effort to review the records of all femur fractures at our Level 1 trauma center, which treats more than 200 femur shaft fractures alone per year, because there is no specific diagnostic code for low-energy femur fractures.
Of the 16 patients studied, there were 15 women and one man (mean age, 69.1 years; median, 67.5 years; range, 51–90 years). The patients had been treated a mean of 6.3 years (median, 6 years; range, 3–10 years) with any bisphosphonate. With the exception of one man on long-term bisphosphonate therapy for an underlying myeloma, the other 15 patients were all older women on bisphosphonate treatment for osteoporosis (Table 1). Three of the 16 patients sustained complete femoral fractures before any physician visits occurred and therefore before any radiographic studies were obtained. Four patients sustained five completed femur fractures after consulting physicians but before any prophylactic surgeries were performed. No patients were lost to followup, although two died after 67 and 84 months of followup, respectively. Two patients with less than 1-year followup had all been treated since June 2010. Six patients who had not had recent followup (> 1 year) because they were doing well at last visit were contacted by telephone as part of their medical followup care and all six denied pain or functional limitations. All living patients have followup within 12 months of the date of manuscript revision. Minimum followup of the 16 patients was 9 months (average, 44.0 months; median, 31 months; range, 9–112 months). No patients were recalled specifically for this study; all data were obtained from medical records and radiographs.
Routine followup consisted of postoperative visits with radiographs at 2 to 3 weeks, every 2 to 3 months until the lesion or fracture was healed, and annually thereafter until discharge due to a clinical determination of a healed status. We used medical records to collect demographic data, nature and duration of symptoms, previous diagnoses rendered by prior physicians, medication history including dosage and duration of bisphosphonates, treatment methods, followup status, complications, and results of treatment.
The senior author reviewed all patients’ radiographic images to identify features associated with the fractures and stress fractures, including the presence of lateral cortical thickening, any stress fracture lines, any fractures and their bony orientation, and any associated features on radiographic studies, such as stress fracture lines, periosteal and endosteal changes, edema, bone scan activity, or any other notable findings.
We compared the LOS data for the two groups (prophylactically treated versus completed fracture treated) using a nonparametric rank sum test.
Results
The clinical (Table 2) and radiographic (Table 3) findings of the 16 patients with 24 impending or completed stress fractures of the femur are shown. Of the eight patients with bilateral involvement, two fractured both sides, two had bilateral impending fractures, and four had completed fractures on one side and impending fractures on the other side. The male patient received a left prophylactic intramedullary (IM) reconstruction (recon) nail in 1991 for an impending fracture from myeloma and has had no further problems in that femur for 19 years. After 10 years of monthly intravenous bisphosphonates, he developed a painful contralateral subtrochanteric stress fracture that has subsequently remained pain-free after prophylactic fixation. Prodromal hip and/or thigh pain occurred in all 16 patients. Eleven patients were initially misdiagnosed as having trochanteric bursitis, unidentified femoral lesions, or spine-associated radicular pain. Six patients with seven bisphosphonate-associated stress fractures developed completely displaced fractures while under a physician’s care.
Table 2.
Clinical data from patients treated with bisphosphonates
| Fracture status | Patient | Age (years) | Sex | Side | Alendronate | Duration (years) | Other bisphosphonates | Duration (years) | Followup (months) | Additional surgery |
|---|---|---|---|---|---|---|---|---|---|---|
| Stress fracture treated prophylactically | 1 | 76 | Female | Left | Yes | 3+ | No | 67 | No | |
| 2 | 76 | Female | Right | Yes | 3+ | No | 84 | No | ||
| 3 | 74 | Female | Right | Yes | 3 | No | 72 | No | ||
| 4 | 76 | Female | Right | Yes | 7 | No | 59 | No | ||
| 4 | 76 | Female | Left | Yes | 7 | No | 59 | No | ||
| 5 | 65 | Female | Right | Yes | 9+ | No | 42 | No | ||
| 6 | 79 | Male | Right | No | Zoledronic acid, pamidronate | 10 | 25 | No | ||
| 7 | 53 | Female | Left | Yes | 5+ | Risedronate | 1+ | 10 | No | |
| 8 | 90 | Female | Right | Yes | 9 | Ibandronate | 1+ | 20 | No | |
| 9 | 61 | Female | Left | Yes | 3+ | Zoledronic acid | 1.5 | 20 | No | |
| 9 | 61 | Female | Right | Yes | 3+ | Zoledronic acid | 1.5 | 19 | No | |
| 10 | 69 | Female | Right | Yes | 8.5 | No | 18 | No | ||
| 11 | 64 | Female | Right | Yes | 4+ | No | 80 | No | ||
| 12 | 84 | Female | Left | No | Risedronate | 6 | 10 | No | ||
| Completed fracture after radiographic studies | 3 | 74 | Female | Left | Yes | 3 | No | 74 | No | |
| 7 | 51 | Female | Right | Yes | 4 | Risedronate | 1+ | 28 | Yes* | |
| 10 | 69 | Female | Left | Yes | 8.5 | No | 18 | No | ||
| 13 | 72 | Female | Right | Yes | 4+ | Zoledronic acid | 1 | 9 | No | |
| 14 | 66 | Female | Left | Yes | 10+ | No | 16 | No | ||
| 14 | 66 | Female | Right | Yes | 9+ | No | 29 | No | ||
| 16 | 66 | Female | Right | Yes | 7 | No | 73 | Yes† | ||
| Completed fracture before any radiographic studies | 5 | 60 | Female | Left | Yes | 4+ | No | 112 | Yes‡ | |
| 15 | 65 | Female | Left | Yes | 10 | No | 11 | Yes§ | ||
| 16 | 65 | Female | Left | Yes | 6 | No | 89 | Yes∥ |
* Dynamized at 6 months; revised at 10 months for broken intramedullary nail; †nonunion requiring revision reconstruction nail at 15 months; ‡dynamized at 3 months; §dynamized at 7 months; ∥nonunion requiring revision reconstruction nail at 18 months.
Table 3.
Radiographic observations from patients treated with bisphosphonates
| Fracture status | Patient | Black line on plain film | Black line on CT | MRI | Bone scan | Radiographic thick cortex | Transverse lateral cortical fracture |
|---|---|---|---|---|---|---|---|
| Stress fracture treated prophylactically | 1 | NA | No | NA | NA | Yes | NA |
| 2 | No | No | A, B, C | NA | Yes | NA | |
| 3 | Yes* | NA | A, B | E | Yes | NA | |
| 4 | Yes | NA | NA | E | Yes | NA | |
| 4 | Yes | NA | NA | E | Yes | NA | |
| 5 | No | No | NA | E | Yes | NA | |
| 6 | No | NA | NA | NA | Yes | NA | |
| 7 | No | NA | C | NA | No¶ | NA | |
| 8 | NA | NA | A, B | NA | Yes | NA | |
| 9 | No | NA | NA | NA | Yes | NA | |
| 9 | Yes† | NA | NA | NA | Yes | NA | |
| 10 | No | No | A, B | NA | Yes | NA | |
| 11 | No‡ | No | A, B | NA | Yes | NA | |
| 12 | No‡ | NA | A, B | NA | Yes | NA | |
| Completed fracture after radiographic studies | 3 | NA | NA | B, D | NA | Yes | Yes |
| 7 | Yes* | Yes | B§ | F§ | Yes | Yes | |
| 10 | No | No | A, B | NA | Yes | Yes | |
| 13 | Yes* | NA | NA | E | Yes | Yes | |
| 14 | NA | NA | A, B | NA | Yes | Yes | |
| 14 | NA | NA | A, B∥ | NA | Yes | Yes | |
| 16 | No | NA | NA | E | Yes | Yes | |
| Completed fracture before any radiographic studies | 5 | NA | NA | NA | NA | Yes | Yes |
| 15 | NA | NA | NA | NA | Yes | Yes | |
| 16 | NA | NA | NA | NA | NA# | Yes** |
* Subtle; †partial-thickness black line; ‡developed a thin black line in the zone of thickened cortical bone after intramedullary nail fixation; §4 months before CT scan and fracture; ∥6 months before fracture (3 months before symptom onset); ¶periosteal reactive bone present (she had minimal thickening on the opposite side before it fractured); #original fracture films not available; **original fracture films not available; transverse fracture exhibits rounding of edges on 16 months postoperative films; NA = not available; A = lateral cortical thickening; B = localized edema pattern; C = visible stress fracture line; D = lateral cortical irregularity, questionable thickening; E = focal lateral cortical increased activity; F = focal increased activity, medial greater than lateral.
Of the 15 other femoral stress fractures identified in the review of the 400 fractures surgically treated by the senior author, six were stress fractures of the femoral neck (only one was on bisphosphonates) and nine were stress fractures involving the medial femoral diaphyseal cortex (two were on bisphosphonates and one was on calcitonin).
Of the four patients with completed bisphosphonate-associated stress fractures who had preoperative radiographs, only two patient’s radiographic studies revealed a complete transverse horizontal stress fracture line. These lines, when present, were subtle.
Of the 14 femurs with bisphosphonate-associated stress fractures treated with prophylactic IM recon nail fixation, none had subsequently developed a completed fracture nor required any additional surgery at the time of last followup. None required ambulatory aids. None had pain except one patient with progressive collapsing lumbar scoliosis who has bilateral leg pain of unclear etiology and one fully active patient with a persistent lateral cortical stress fracture line who had intermittent nonlimiting discomfort 80 months after prophylactic fixation. Of 10 fractured femurs in eight patients with bisphosphonate-associated stress fractures, three fractures united uneventfully (see Appendix 1; supplemental materials are available with the online version of CORR). Three of these femoral reconstructions underwent distal interlocking screw removal at 3, 6, and 7 months, respectively, two of which united. The third patient had a fractured nail at 10 months, requiring a revision reamed IM recon nail insertion that culminated in fracture healing. One patient (Patient 16) had nonunion failures of bilateral fractures previously treated elsewhere with interlocked IM nails; both were revised to reamed IM recon nails (at 15 and 18 months, respectively) and both united over the next 6 months. Two completed fractures in one patient manifested incomplete bridging union across both fracture sites at the last radiographic followup of 16 and 29 months, respectively, thereby remaining at risk of subsequent fixation failure.
The average hospital LOS was shorter (p = 0.0467) in patients who underwent prophylactic fixation (3.8 days; SD, 1.6 days; range, 2–6 days) than in patients treated for completed fractures (5.6 days; SD, 1.6 days; range, 3–8 days).
Discussion
Bisphosphonates are widely utilized to treat osteoporosis [1, 3, 4, 14, 19]. Alendronate is the most commonly prescribed bisphosphonate and the one most commonly implicated in reports of bisphosphonate-associated femoral stress fractures [5, 8, 17]. Our main objectives were to (1) confirm the clinical and radiographic characteristics of long-term bisphosphonate treatment-associated stress fractures compared to the literature, (2) determine whether any patients with completed fractures had no preexisting transverse stress fracture lines, (3) determine the need for additional surgery, and (4) determine whether the associated hospital LOS differed in patients who had prophylactic internal fixation compared to those who had fixation of completed fractures.
Our retrospective study has limitations. First, the incidence of these fractures cannot be determined from our data. Other completed stress fractures may have masqueraded as traumatic fractures and been unrecognized. Second, we lacked information on the patient’s bone metabolic parameters. Such information might allow one to determine patients at risk. Third, as with prior reports, we are unable to define specific characteristics other than prolonged continuous bisphosphonate usage that placed this minority of bisphosphonate-treated patients at higher risk for this complication; thus, this complication must be considered when treating any patient on long-term bisphosphonates. Fourth, this small retrospective study may have inherent biases such as the lack of a larger control group with stress fractures not associated with bisphosphonate usage. Fifth, many factors affect hospital LOS, and a much larger group with more complete data would be required to confirm the differences in complications and LOS for treating completed versus impending stress fractures.
Similar to prior series, our patient population consisted of predominantly osteoporotic older women on bisphosphonates for at least 3 years [4, 5, 8–11, 16–18]. The bilaterality in more than ½ of the osteoporotic women is in keeping with prior reports [12], as is the presence of prodromal pain in all of our patients. The identification of bisphosphonate usage in only three of the senior author’s 15 other patients with femoral stress fractures supports the concept that these lateral femoral cortex-initiated bisphosphonate-associated stress fractures are unique. All of our patients had clinical (Table 2) and radiographic (Table 3) findings similar to those of prior reports (Table 1). Shane et al. [18] described radiographic and clinical characteristics that included fractures with minimal to atraumatic activity, transverse lateral fracture line configuration, localized periosteal reaction, increased lateral cortical thickness, delayed healing, bilaterality, and prodromal symptoms. Bone scans and MR images were 100% sensitive in our patients.
Of four patients with completed fractures who had preoperative plain radiographs, only two had transverse black lines, contrary to the reports of Koh et al. [9] and Shane et al. [18]. This finding confirms completed fractures can occur in the absence of the dreaded black line.
None of the 14 impending stress fractures we treated prophylactically subsequently fractured or required additional surgery, confirming prophylactic fixation of painful impending stress fractures may obviate the need for further surgical intervention. Banffy et al. [2] reported on 12 stress fractures, six treated nonoperatively and six treated prophylactically. They found five of six patients treated nonoperatively failed and progressed to fracture completion in an average time of 10 months (range, 3–18 months). All six patients treated prophylactically had no complications postoperatively [2]. Shane et al. [18] recommend prophylactic nail fixation for incomplete fractures accompanied by pain, particularly since patients may progress to a completed fracture. If the pain is minimal or absent, a trial of nonoperative treatment with limited weightbearing with the assistance of a medical device may be considered [18]. Incidentally, the absence of stress fracture development in the man with 10 years of bisphosphonate administration on the side with a preexisting IM recon nail, in the presence of a stress fracture reaction in the unprotected side, is anecdotal evidence of the potential benefit of prophylactic internal fixation.
In a study by Banffy et al. [2] comparing patients treated prophylactically and those treated after fracture completion, four of their 33 patients with completed fractures had postoperative complications, including nonunion, delayed union, and painful hardware. Two patients required symptomatic hardware removal. No prophylactically treated patients experienced complications [2]. None of our 14 prophylactically treated femurs required subsequent surgery and all but one (the patient with lumbar scoliosis) have been satisfied with their pain relief. Conversely, of the eight patients with 10 completed fractures, four patients have required six additional surgeries in five femurs, including screw removal for dynamization (three) and complete revision for a fractured nail (one) or nonunion (two). The observed fracture unions in a fifth patient (who had bilateral fractures) are incomplete and she remains at risk for future failure. The shorter hospital LOS for the prophylactically treated stress fractures compared to fixation of completed fractures we found in this study mirrors what the senior author showed in a prior study of impending versus completed pathologic femur fractures due to metastatic disease. In that study, prophylactic fixation compared to repair after fracture completion was also associated with a shorter hospital LOS (7 versus 11 days) [20]. Banffy et al. [2] also found the average LOS was shorter for patients treated prophylactically (3.8 days) than for patients after fracture completion (5.6 days). We believe it is preferable to prevent a fracture rather than to treat one.
Based on our limited data, we can make no firm recommendations regarding the recommended duration of bisphosphonate therapy. Shane et al. [18] stated the optimal duration of bisphosphonate therapy is unknown. Black et al. [3] found patients who discontinued alendronate after 5 years did not increase their true fracture risk over the subsequent 5 years. An individual patient’s fracture risk should be considered before discontinuing bisphosphonate medication [18]. Calcium and vitamin D should usually be administered for the treatment of osteoporosis; other osteoporotic medications such as teriparatide may need to be considered [18].
For the majority of patients on bisphosphonates, this type of femoral stress fracture and low-energy fracture is unlikely to occur. However, orthopaedic surgeons and other physicians should be aware of this complication, as they are likely to encounter such patients due to the millions of patients on bisphosphonate medications. The subtle radiographic findings need to be appreciated so that prophylactic fixation can be performed before a painful completed fracture occurs with its attendant greater morbidity.
Electronic supplementary material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgments
The authors thank Dr Frederick Dorey, PhD, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA, for his assistance in performing the statistical analysis and Elizabeth A. Newman, BS, Medical Student Researcher, for her superb assistance, including reviewing the 400 femur fractures, updating and verifying all data, and participating in the manuscript revisions.
Footnotes
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA approval status, of any drug or device before clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
References
- 1.Advisory Task Force on Bisphosphonate-Related Osteonecrosis of the Jaws, American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg. 2007;65:269–376. [DOI] [PubMed]
- 2.Banffy MB, Vrahas MS, Ready JE, Abraham JA. Nonoperative versus prophylactic treatment of bisphosphonate-associated femoral stress fractures. Clin Orthop Relat Res. 2011;469:2028–2034. doi: 10.1007/s11999-011-1828-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Black DM, Schwartz AV, Ensrud KE, Cauley JA, Levis S, Quandt SA, Satterfield S, Wallace R, Bauer DC, Palermo L, Wehren LE, Lombardi A, Santora AC. Cummings SR; FLEX Research Group. Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. JAMA. 2006;296:2927–2938. doi: 10.1001/jama.296.24.2927. [DOI] [PubMed] [Google Scholar]
- 4.Capeci CM, Tejwani NC. Bilateral low-energy simultaneous or sequential femoral fractures in patients on long-term alendronate therapy. J Bone Joint Surg Am. 2009;91:2556–2561. doi: 10.2106/JBJS.H.01774. [DOI] [PubMed] [Google Scholar]
- 5.Cermak K, Shumelinsky F, Alexiou J, Gebhart MJ. Case reports: subtrochanteric femoral stress fractures after prolonged alendronate therapy. Clin Orthop Relat Res. 2010;468:1991–1996. doi: 10.1007/s11999-009-1192-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cummings SR, Black DM, Thompson DE, Applegate WB, Barrett-Connor E, Musliner TA, Palermo L, Prineas R, Rubin SM, Scott JC, Vogt T, Wallace R, Yates AJ, LaCroix AZ. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures. JAMA. 1998;280:2077–2082. doi: 10.1001/jama.280.24.2077. [DOI] [PubMed] [Google Scholar]
- 7.Ensrud KE, Barrett-Connor EL, Schwartz A, Santora AC, Bauer DC, Suryawanshi S, Feldstein A, Haskell WL, Hochberg MC, Torner JC, Lombardi A, Black DM. Randomized trial of effect of alendronate continuation versus discontinuation in women with low BMD: results from the Fracture Intervention Trial Long-term Extension. J Bone Miner Res. 2004;19:1259–1269. doi: 10.1359/JBMR.040326. [DOI] [PubMed] [Google Scholar]
- 8.Goddard MS, Reid KR, Johnston JC, Khanuja HS. Atraumatic bilateral femur fracture in long-term bisphosphonate use. Orthopedics. 2009;32(8). pii: orthosupersite.com/view.asp?rID = 41933. doi: 10.3928/01477447-20090624-27. [DOI] [PubMed]
- 9.Koh JS, Goh SK, Png MA, Kwek EB, Howe TS. Femoral cortical stress lesions in long-term bisphosphonate therapy: a herald of impending fracture? J Orthop Trauma. 2010;24:75–81. doi: 10.1097/BOT.0b013e3181b6499b. [DOI] [PubMed] [Google Scholar]
- 10.Kwek EB, Goh SK, Koh JS, Png MA, Howe TS. An emerging pattern of subtrochanteric stress fractures: a long-term complication of alendronate therapy? Injury. 2008;39:224–231. doi: 10.1016/j.injury.2007.08.036. [DOI] [PubMed] [Google Scholar]
- 11.Neviaser AS, Lane JM, Lenart BA, Edobor-Osula F, Lorich DG. Low-energy femoral shaft fractures associated with alendronate use. J Orthop Trauma. 2008;22:346–350. doi: 10.1097/BOT.0b013e318172841c. [DOI] [PubMed] [Google Scholar]
- 12.Nieves JW, Cosman F. Atypical subtrochanteric and femoral shaft fractures and possible association with bisphosphonates. Curr Osteoporos Rep. 2010;8:34–39. doi: 10.1007/s11914-010-0007-2. [DOI] [PubMed] [Google Scholar]
- 13.Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin Endocrinol Metab. 2005;90:1294–1301. doi: 10.1210/jc.2004-0952. [DOI] [PubMed] [Google Scholar]
- 14.Ott SM. Editorial: long-term safety of bisphosphonates. J Clin Endocrinol Metab. 2005;90:1897–1899. doi: 10.1210/jc.2005-0057. [DOI] [PubMed] [Google Scholar]
- 15.Pols HA, Felsenberg D, Hanley DA, Stepán J, Muñoz-Torres M, Wilkin TJ, Qin-sheng G, Galich AM, Vandormael K, Yates AJ, Stych B. Multinational, placebo-controlled, randomized trial of the effects of alendronate on bone density and fracture risk in postmenopausal women with low bone mass: results of the FOSIT study. Osteoporos Int. 1999;9:461–468. doi: 10.1007/PL00004171. [DOI] [PubMed] [Google Scholar]
- 16.Sayed-Noor AS, Sjödén GO. Case reports: two femoral insufficiency fractures after long-term alendronate therapy. Clin Orthop Relat Res. 2009;467:1921–1926. doi: 10.1007/s11999-009-0725-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Schneider JP. Bisphosphonate and low-impact femoral fractures: current evidence on alendronate-fracture risk. Geriatrics. 2009;64:18–23. [PubMed] [Google Scholar]
- 18.Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O’Keefe R, Papapoulos S, Sen HT, Meulen MC, Weinstein RS, Whyte M. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone Mineral Research. J Bone Miner Res. 2010;25:2267–2294. doi: 10.1002/jbmr.253. [DOI] [PubMed] [Google Scholar]
- 19.US Food and Drug Administration. Background document for meeting of Advisory Committee for Reproductive Health Drugs and Drug Safety and Risk Management. Available at: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/DrugSafetyandRiskManagementAdvisoryCommittee/UCM270958.pdf. Accessed October 10, 2011.
- 20.Ward WG, Holsenbeck S, Dorey FJ, Sprang J, Howe D. Metastatic disease of the femur: surgical treatment. Clin Orthop Relat Res. 2003;415(suppl):S230–S244. doi: 10.1097/01.blo.0000093849.72468.82. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.