

Abstract
Interleukin (IL)-6 is a cytokine featuring redundancy and pleiotropic activity. While IL-6, when transiently produced, contributes to host defense against acute environmental stress, continuous dysregulated IL-6 production plays a significant pathological role in several systemic autoimmune diseases. In response to the expectation that IL-6 blockade would constitute a novel therapeutic strategy for the treatment of these diseases, tocilizumab, a humanized anti-IL-6 receptor antibody, was developed. Clinical trials have verified the efficacy and the safety of tocilizumab for patients with rheumatoid arthritis, resulting in approval of this innovative biologic for the treatment of rheumatoid arthritis in more than 90 countries worldwide. Pathological analyses of the effect of IL-6 on the development of autoimmune diseases and a considerable number of case reports and pilot studies have also indicated the beneficial effects of this antibody on other systemic autoimmune diseases, including systemic lupus erythematosus, systemic sclerosis, polymyositis, and large-vessel vasculitis.
1. Introduction
Interleukin (IL)-6 is a cytokine featuring redundancy and pleiotropic activity. It was successfully cloned in 1996 as a B-cell differentiation factor, which promotes B-cell differentiation into antibody-producing cells [1]. Subsequent in vitro studies and analysis of IL-6 transgenic mice have shown that IL-6 acts not only on B cells but also on T cells, hepatocytes, hematopoietic progenitor cells, and various other cells [2–4]. One of the important functions of IL-6 is the differentiation of CD4positive naïve T cells into effector cells. IL-6 in the presence of TGF-β promotes naïve T-cell differentiation into Th17 cells, while IL-6 inhibits TGF-β-induced regulatory T-cell (Treg) differentiation [5], causing imbalance between Th17 and Treg, which is a primary pathogenic factor in several autoimmune diseases [6].
IL-6 transmits its signal through its binding to transmembrane receptors or the soluble IL-6 receptor (IL-6R) [7, 8]. After binding of IL-6 to IL-6R, the resultant IL-6/IL-6R complex associates with gp130 and induces homodimerization of gp130, which triggers signal transduction system [9].
The pathological significance of IL-6 for diseases was first demonstrated in a case of cardiac myxoma [10]. The culture fluid obtained from the myxoma tissues of a patient who presented with fever, arthritis with positivity for antinuclear factor, increased C-reactive protein (CRP) levels and hypergammaglobulinemia and was diagnosed with undifferentiated connective tissue disease, contained a large quantity of IL-6, which suggested that IL-6 might contribute pathologically to chronic inflammation and autoimmunity. Subsequent studies have shown that dysregulation of IL-6 production is implicated in the pathogenesis of Castleman's disease [11], rheumatoid arthritis (RA) [12], and various other autoimmune, inflammatory, and malignant diseases [2–4].
Because of the biological activities of IL-6 and its pathological role in diseases, it was anticipated that IL-6 blockage would constitute a novel treatment strategy for autoimmune and inflammatory diseases [4, 13–15]. To this end, tocilizumab was developed, which is a humanized anti-IL-6R monoclonal antibody (Ab) of the IgG1 class that was generated by grafting the complementarity determining regions of a mouse anti-human IL-6R Ab onto human IgG1. Tocilizumab blocks IL-6-mediated signal transduction by inhibiting IL-6 binding to transmembrane and soluble IL-6R.
2. Approval of Tocilizumab for the Treatment of Rheumatoid Arthritis
2.1. Pathological Role of IL-6 in Rheumatoid Arthritis
RA is a chronic, progressive inflammatory disease of the joints and surrounding tissues accompanied by intense pain, irreversible joint destruction, and systemic complications such as fatigue, anemia, and fever [16]. At the local level, inflammatory cells invade the otherwise relatively acellular synovium leading to neovascularization, synoviocyte hyperplasia, and formation of pannus tissue, which in turn causes destruction of cartilage, erosion of the adjacent bone, and, ultimately, loss of function of the affected joint. The biological activities of IL-6 such as proinflammatory activity, augmentation of synovial fibroblast proliferation, osteoclast differentiation, matrix metalloproteinase (MMP), and vascular endothelial growth factor (VEGF) production, as well as lymphocyte differentiation and its elevation in both serum and synovial fluids of patients with RA [17–22] indicate that IL-6 is one of the key cytokines involved in the development of RA.
It has been demonstrated in animal model of RA, that are type II collagen-induced arthritis (CIA), and antigen-induced arthritis, IL-6 performs a major role in the development and progression of joint destruction, while IL-6 deficiency generated by gene knockout or IL-6 blockade by means of anti-IL-6R Ab reduces the incidence and severity of arthritis in these models [23–28]. In the CIA model, immunization with type II collagen predominantly increased the frequency of Th17 cells and treatment of mice with anti-IL-6R Ab during priming markedly suppressed the induction of Th17 cells and arthritis development, while treatment with anti-IL-6R Ab on day 14 failed to suppress both Th17 differentiation and arthritis [29]. Similarly, in a glucose-6-phosphate-isomerase- (GPI-)induced arthritis model, administration of anti-IL-6R Ab on day 0 or 3 suppressed Th17 differentiation and protected against arthritis induction, while injection of anti-IL-6R Ab on day 14, at the peak of arthritis, did not bring about any improvement in arthritis [30]. Arthritis of anti-type II collagen antibody-induced arthritis (CAIA) is another arthritis model, but, in this model, the priming phase of T cell dependent antibody generation is skipped. Although IL-6 is also elevated in this model, CAIA was profoundly suppressed in TNF−/− mice but not in IL-6−/− mice [31], indicating that TNF may play a more significant role in the development of CAIA than IL-6. These observations suggest that in the priming phase IL-6 is a required factor for the activation of T cell response and production of antibodies specific for joint components and that in the effector phase TNF is the main generator of arthritis [32]. We found that tocilizumab was not effective for clinical improvement in the condition of two patients with psoriatic arthritis, for whose development immune activation does not appear to be required [33]. The clinical antiarthritic effect of tocilizumab is slower than that of TNF inhibitors, which may be due to the different pathological roles of IL-6 and TNF in the development of RA (Figure 1).
Figure 1.
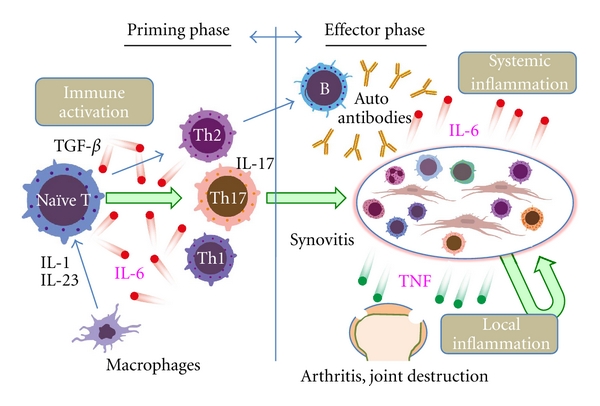
Pathological role of IL-6 in rheumatoid arthritis. IL-6 is important for development of Th17 and induction of autoantibodies such as rheumatoid factor. Activated Th17 cells and autoantibodies generate pannus in combination with activated fibroblastic synoviocytes, macrophages, and lymphocytes. Inflamed synovitis such as pannus is a major source of inflammatory cytokines including IL-6, and systemic inflammation (resulting in production of acute phase protein, anemia, and fatigue) is mainly mediated by IL-6. Tumor necrosis factor (TNF) plays a major role in the progression of local types of inflammation (arthritis) such as arthralgia, swelling, and joint destruction but plays a minor role during the priming phase.
2.2. Efficacy of Tocilizumab in Randomized Controlled Trials
As shown in Table 1, seven phase III clinical trials of tocilizumab subsequent to phase I and II studies demonstrated its efficacy either as monotherapy or in combination with disease-modifying antirheumatic drugs (DMARDs) for adult patients with moderate to severe RA [34–40]. A Cochrane database systematic review concluded that tocilizumab-treated patients taking concomitant methotrexate were four times more likely to achieve American College of Rheumatology (ACR) 50 improvement (absolute %, 38.8% versus 9.6%) and 11 times more likely to achieve Disease Activity Score (DAS) remission (30.5% versus 2.7%) than patients taking a placebo [41]. Furthermore, the SAMURAI [34] and LITHE studies [40] proved that radiological damage of joints was significantly inhibited by the treatment. The findings of the RADIATE trial showed that, among RA patients who had previously discontinued TNF inhibitors 50% achieved ACR20, 28.8% ACR50, and 12.4% ACR70 responses [36]. The ACR improvement and DAS remission criteria include an acute-phase reactant component, so that there was concern that the effect of tocilizumab evaluated with these criteria might be overestimated. However, it was found that, even when criteria such as the Simplified Disease Activity Index (SDAI) and Clinical Disease Activity Index (CDAI) were used, remission rates for patients treated with tocilizumab were in the same range as those for patients treated with TNF inhibitors [42, 43].
Table 1.
Phase III randomized controlled trials of tocilizumab for RA patients. Summary of the results of seven phase III randomized controlled trials of tocilizumab. DMARDs: disease modifying antirheumatic drugs, IR: inadequate response, TCZ: tocilizumab, anti-TNF: anti-tumor necrosis factor inhibitor, MTX: methotrexate.
| Study | Reported year | Population | Week at evaluation | Treatment arms | Patient (n) | Response rates (%) | Remission rate (%) | Radiological progression | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ACR20 | ACR50 | ACR70 | DAS28<2.6 | TSS: Total Sharp score |
ES: Erosion score |
JSNS: Joint space narrowing score |
||||||
| SAMURAI | 2007 | DMARDs IR | 52 W | TCZ (8) | 157 | 78 | 64 | 44 | 59 | 2.3 | 0.9 | 1.5 |
| DMARDs | 145 | 34 | 13 | 6 | 3 | 6.1 | 3.2 | 2.9 | ||||
|
| ||||||||||||
| TOWARD | 2008 | DMARDs IR | 24 W | TCZ (8) + DMARDs | 803 | 61 | 38 | 21 | 30 | |||
| DMARDs | 413 | 25 | 9 | 3 | 3 | |||||||
|
| ||||||||||||
| RADIATE | 2008 | Anti-TNF IR | 24 W | TCZ (4) + MTX | 161 | 30 | 17 | 5 | 8 | |||
| TCZ (8) + MTX | 170 | 50 | 29 | 12 | 30 | |||||||
| placebo + MTX | 158 | 10 | 4 | 1 | 2 | |||||||
|
| ||||||||||||
| OPTION | 2008 | MTX IR | 24 W | TCZ (4) + MTX | 186 | 48 | 31 | 12 | 13 | |||
| TCZ (8) + MTX | 191 | 59 | 44 | 22 | 27 | |||||||
| placebo + MTX | 189 | 26 | 11 | 2 | 1 | |||||||
|
| ||||||||||||
| SATORI | 2009 | MTX IR | 24 W | TCZ (8) | 61 | 80 | 49 | 30 | 43 | |||
| MTX | 64 | 25 | 11 | 6 | 2 | |||||||
|
| ||||||||||||
| AMBITION | 2010 | MTX, anti-TNF naïve |
24 W | TCZ (8) | 286 | 70 | 44 | 28 | 34 | |||
| MTX | 284 | 53 | 34 | 15 | 12 | |||||||
|
| ||||||||||||
| LITHE | 2011 | MTX IR | 52 W | TCZ (4) + MTX | 394 | 47 | 29 | 16 | 30 | 0.34 | 0.21 | 0.13 |
| TCZ (8) + MTX | 398 | 56 | 30 | 20 | 47 | 0.29 | 0.17 | 0.12 | ||||
| MTX | 393 | 25 | 10 | 4 | 8 | 1.13 | 0.71 | 0.42 | ||||
2.3. Efficacy of Tocilizumab in Actual Medical Practice
On the basis of the excellent results obtained for the efficacy of tocilizumab, it was approved in April 2008 for the treatment of RA in Japan. The recommended posology of tocilizumab (proprietary name, Actemra) is 8 mg/kg, every 4 weeks. Subsequently, the European Medicines Agency approved tocilizumab (proprietary name, RoACTEMRA) for RA in January 2009 at a recommended dose of 8 mg/kg. In the United States, it was approved for RA in January 2010, but the recommended starting dose is 4 mg/kg administered once every 4 weeks followed by an increase to 8 mg/kg depending on clinical response. While the dosage differs among countries, tocilizumab has now been approved for the treatment of RA in more than 90 countries worldwide [14].
In addition to clinical trials, the efficacy of tocilizumab was reconfirmed in actual medical practice. The finding by the three recent studies, the German phase IIIb real-life study (TAMARA study) [44, 45], the Danish nationwide cohorts of RA patients (DANBIO registry) study [46], and the multicenter retrospective real-life study (REACTION study) [47, 48] are shown in Table 2. In the TAMARA study, 286 patients were registered for an analysis of the effectiveness and safety [44, 45], 41.6% of whom had previously been treated with TNF inhibitors. ACR50 and ACR70 response rates at week 24 were 50.7% and 33.9%, respectively, while 47.6% of the patients achieved DAS remission and 54.9% the European League Against Rheumatism (EULAR) good response. Remission rates with the new ACR/EULAR Boolean-based criteria for clinical studies were 15.0% after 12 weeks and 20.3% after 24 weeks, and CDAI and SDAI remission rates were 24.1% and 25.2%, respectively. For the DANBIO registry in Denmark, 178 patients with RA treated with tocilizumab were identified [46]. The disease activity decreased at all-time points, with remission rates for tocilizumab treatment of 39% after 24 weeks and 58% after 48 weeks. EULAR good or moderate response rates were 88% and 84%, respectively. These response rates were comparable to those found for patients switching to their second TNF inhibitors and to the response rates previously observed in phase III clinical trials. In Japan, 229 patients were registered in the REACTION study for an analysis of the effectiveness of tocilizumab [47, 48]. Clinical remission at week 52 was observed in 43.7% of the patients, radiographic non-progression in 62.8%, and functional remission in 26.4%. The retention rates at 24 and 52 weeks were 79.5% and 71.1%, respectively, and were the same for those with or without previous anti-TNF treatment. These results indeed show the efficacy of tocilizumab for the treatment of RA in actual medical practice.
Table 2.
Reevaluation of antirheumatic effects of tocilizumab in actual medical practice. Summary of the contents of the three actual medical practice of tocilizumab for rheumatoid arthritis.
| Study | Country | Patient number | Registry | Evaluation |
|---|---|---|---|---|
| TAMARA | Germany | 286 | Sep. 2008~Sep. 2009 | Disease activity |
| EULAR response | ||||
| ACR response | ||||
| Adverse events | ||||
| 2011 ACR/EULAR remission | ||||
|
| ||||
| DAMBIO | Denmark | 178 | ~April 2010 | Disease activity |
| EULAR response | ||||
| Drug survival | ||||
|
| ||||
| REACTION | Japan | 229 | April 2008~March 2009 | Disease activity |
| EULAR response | ||||
| Adverse events | ||||
| Drug survival | ||||
2.4. Safety Profile of Tocilizumab
The safety and tolerability profiles of tocilizumab monotherapy for Japanese RA patients obtained from six initial trials and five long-term extensions have been published [49]. For these studies, 601 patients with a total exposure to tocilizumab of 2,188 patient-years (pt-yr) were enrolled. The medial treatment duration was 3.8 years. The incidence of adverse events (AEs), including abnormal laboratory test findings, was calculated as 465/100 pt-yr, with infections being the most common serious AEs (6.2/100 pt-yr). Of the patients treated more than 5 years, 59.7% met the DAS28 remission criteria at 5 years, which demonstrates the excellent tolerability and high efficacy of tocilizumab. In addition, a systemic literature review to assess the risk of AEs for RA patients treated with tocilizumab reported that pooled odds ratios (ORs) indicated statistical significance for an increased risk of AEs for patients treated with 8 mg/kg of tocilizumab plus methotrexate compared with controls (OR = 1.53; 95%CI = 1.26–1.86), as well as a heightened risk of infection (OR = 1.30; 95%CI = 1.07–1.58) [50]. However, no increases in the incidence of malignancy or hepatitis were detected.
The results of an interim analysis of a postmarketing surveillance of all patients treated with tocilizumab in Japan were recently reported [51]. This analysis comprised 3,881 patients who received 8 mg/kg of tocilizumab every 4 weeks, and was observed for 28 weeks. Occurrence of a total of 3,004 AEs in 1,641 patients (167/100 pt-yr) and 490 serious AEs in 361 patients (27/100 pt-yr) was reported. The most frequent AE and serious AE were infection at 31/100 pt-yr and 9/100 pt-yr, respectively, with the majority of infections being pneumonia and cellulitis. Cardiovascular events were observed in 0.9% (myocardial infarction in 4 patients or 0.1%). Abnormalities in laboratory test findings, such as increases in lipid and liver function parameters were common, and total and serious AEs associated with laboratory test abnormalities were 35/100 pt-yr and 2/100 pt-yr, respectively. The increased lipid level resulting from tocilizumab administration is perhaps mediated by its effecting on lipoprotein receptor expression, since it was recently shown that overproduction of IL-6 reduces blood lipid levels via upregulation of very-low-density lipoprotein receptors [52]. In contrast, we and others observed that HbA1c levels and insulin sensitivity improved as a result of tocilizumab treatment [53, 54]. While white blood cell and neutrophil counts usually decreased just after tocilizumab injection, this was not related to the incidence of infection. Twenty-five patients died for a standardized mortality ratio of 1.66, which was similar to the results reported for a Japanese cohort study of RA. The results of this analysis thus demonstrated that tocilizumab is acceptable in the actual clinical setting.
Seven cases of gastrointestinal (GI) perforation in six patients were reported in this postmarketing surveillance. In the worldwide Roche clinical trials, 26 (0.65%) cases of GI perforation were found among patients with RA treated with tocilizumab for a rate of 1.9/1,000 pt-yr and most cases appeared to be complications of diverticulitis [55]. This rate is intermediate between the rates of GI perforations of 3.9/1,000 pt-yr for corticosteroids and 1.3/1,000 pt-yr for anti-TNFα agents reported in the United Health Care database.
The reactivation of tuberculosis is a major concern during anti-TNF treatment [56], but there is no medical consensus regarding the effect of IL-6 blockade on tuberculosis. Okada et al. examined the effects of IL-6 and TNFα blockade on the development of tuberculosis infection in mice and observed that there was less tuberculosis infection for anti-IL-6R Ab than for anti-TNFα Ab [57]. In addition, we showed that tuberculosis antigens-induced interferon (IFN)-γ production was suppressed by the addition of TNF inhibitors (infliximab and etanercept) but not of tocilizumab [58]. Although it seems likely that the incidence of reactivation of tuberculosis is lower during tocilizumab treatment than that during anti-TNF treatment, further detailed studies will be needed to clarify this point.
2.5. The Place of Tocilizumab in Rheumatoid Arthritis Treatment
A number of biologics are available for the treatment of RA. These include anti-TNF blockers (infliximab, etanercept, adalimumab, golimumab, and certolizumab), an IL-1 antagonist (anakinra), a B-cell depletor (rituximab), an IL-6 receptor inhibitor (tocilizumab), and a T-cell activation blocker (abatacept). These biological modifiers target different molecules and B cells, leading to different clinical effects and causing different adverse effects. Since no head-to-head comparative studies have been made of the efficacy of these various agents, it has not yet been determined which of these biologics should be selected for a given patient. Currently, one of the anti-TNF drugs is chosen as a first-line biologic, but between 14 and 38% of patients show no or little response to anti-TNF treatment, with as many as 40% of patients discontinuing these drugs within a year and 50% within 2 years. The findings of the RADIATE trial showed that RA patients who had previously discontinued TNF inhibitors, mainly due to their inefficacy, achieved ACR20/50/70 responses of 50%, 28.8%, and 12.4%, respectively, when tocilizumab was administered at 8 mg/kg every four weeks [36]. At present, tocilizumab is likely to be prescribed as a second-line biologic therapy but will have to overcome significant competition from established anti-TNF therapies.
It is anticipated that tocilizumab will be selected as a first-line biologic for moderately to severely active RA patients with certain complications. AA amyloidosis is a serious complication of RA, and amyloid fibril deposition causes progressive deterioration in various organs [59, 60]. Since the gene activation of serum amyloid A, a precursor protein of amyloid A fibril, depends primarily on IL-6 [61, 62], tocilizumab administration was found to promptly reduce serum concentrations of SAA, just as in the case of CRP [60]. Three case reports showed the clinical ameliorative effect of tocilizumab on gastrointestinal symptoms due to intestinal amyloidosis [63–65], and amyloid A fibril deposits were found to have disappeared in two cases after three injections of tocilizumab [63, 65]. This suggests that tocilizumab may be suitable as a first-line drug for RA patients who are complicated with or are at high risk of developing AA amyloidosis.
2.6. Drug-Free Remission Rate
Remission induction is the current goal for RA, and with the development of biological modifiers, a growing number of RA patients has been able to achieve this goal [66]. The long-term efficacy after cessation of tocilizumab followed by DAS28 remission was demonstrated in the DREAM (drug-free remission after cessation of actemra monotherapy) study [67]. The continuous rate of tocilizumab-free efficacy was 35.1% at 24 weeks and 13.4% at 52 weeks. Serum levels of IL-6 and MMP-3 are useful markers for identifying patients who may be able to discontinue tocilizumab without risk of recurrence. In addition, the RESTORE study (retreatment efficacy and safety to tocilizumab in patients with rheumatoid arthritis at recurrence) demonstrated that retreatment of all relapsed patients with tocilizumab resulted in re-remission [68].
3. Therapeutic Implications of Tocilizumab for Other Systemic Autoimmune Diseases
3.1. Systemic Lupus Erythematosus
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disorder with a broad spectrum of clinical presentations of unknown etiology that mainly affects young women [69]. The pathogenesis of SLE remains unclear, but the concept of apoptosis goes some way towards explaining how the immune system may recognize mainly intracellular antigens. Defects in the clearance of apoptotic cells have been recognized in SLE patients, leading to aberrant uptake by macrophages, which then present intracellular antigens to T and B cells, thus driving the autoimmune process [70]. Cytokine dysregulation is pervasive, and its expression profiles may serve as a marker of disease activity and severity. Recent findings have highlighted type I interferon pathway [71] or Th17 cell activation [72] in the pathogenesis of SLE.
Levels of CRP have been shown to rise in acute illness but not in SLE flares, indicating that IL-6, a major regulator of CRP production, has a minor role in SLE development. However, recent findings suggest that CRP dysregulation also plays a part in the pathogenesis of SLE [73] and SLE may well be a potential target for IL-6 blockade [74]. Serum IL-6 levels of SLE patients were elevated [75–77]. Urinary excretion and renal expression of IL-6 was elevated in SLE patients with active proliferating lupus nephritis [76, 78–81], as were IL-6 levels in the cerebrospinal fluid of SLE patients with central nervous system involvement [82]. Compared to healthy controls, SLE patients had significantly more IL-6 secreting peripheral blood mononuclear cells [83, 84]. Lymphoblastoid cells isolated from SLE patients produced higher levels of IL-6 and blocking of IL-6 inhibited anti-double-stranded DNA (dsDNA) Ab production in vitro [85, 86], indicating that IL-6 is involved in autoantibody production. In murine SLE models, age-associated increases in serum IL-6, soluble IL-6R, and abnormal expression of IL-6R have been detected in MRL/lpr mice [87–89]. In old NZB/W mice, anti-IL-6 Ab reduced and exogenous IL-6 increased production of IgG dsDNA Ab by B cells [90, 91]. Furthermore, IL-6 administration exacerbated glomerulonephritis [92, 93], while IL-6 blockade by means of anti-IL-6R or anti-IL-6 Ab prevented the onset and progression of the disease [94, 95]. Mice with epidermal loss of JunB reportedly developed an SLE phenotype linked to increased epidermal IL-6 secretion, and facial skin biopsies of SLE patients displayed low levels of JunB protein expression, high IL-6, and activated STAT3 levels within lupus lesions [96]. These findings led to an open-label phase I dosage-escalation study of tocilizumab (2 mg/kg, 4 mg/kg or 8 mg/kg, every 2 weeks for 12 weeks) with an enrollment of 16 SLE patients with mild-to-moderate disease activity [97]. Significant improvement in the modified Safety of Estrogens in Lupus Erythematosus National Assessment version of the Systemic Lupus Erythematosus Disease Activity Index score was observed in 8 of the 15 evaluable patients, accompanied by a median reduction in anti-dsDNA Ab levels of 47%. The percentage of CD38highCD19lowIgDnegative plasma cells in the peripheral blood, which was higher for SLE patients than for normal controls (mean 5.3% versus 1.2%), was significantly reduced to 3.1% at 6 weeks. These results indicate that tocilizumab represents a promising therapeutic biologic for SLE.
3.2. Systemic Sclerosis
Systemic sclerosis (SSc) is a connective tissue disease, characterized by fibrosis of the skin and internal organs, vasculopathy, and immune abnormalities [98]. IL-6 is a definite therapeutic target in SSc [99]. IL-6 in the serum of SSc patients was reportedly elevated and the level correlated with the skin severity score [100–104]. Moreover, the culture supernatants of peripheral blood mononuclear cells and skin tissues from SSc patients contained higher concentrations of IL-6 than those from controls [105–109]. In vitro studies demonstrated that IL-6 may contribute to fibrosis by inducing collagen production [110] and induce α-smooth muscle actin (α-SMA) expression by dermal fibroblasts [111], leading to their differentiation into myofibroblasts. On the other hand, anti-IL-6 Ab suppressed procollagen type 1 production in fibroblasts derived from SSc patients in vitro [112]. SSc serum mediated largely by IL-6 was found to induce endothelial cell activation and apoptosis in endothelial cell-neutrophil cocultures [113]. IL-6 is also associated with humoral and cellular immunological abnormalities in SSc [98, 99]. IL-6 is thus thought to play a significant role in producing the characteristics of SSc. Moreover, in a SSc model mouse, induced by immunization with topoisomerase I and complete Freund's adjuvant, loss of IL-6 expression could ameliorate skin and lung fibrosis [114]. We also examined the clinical effect of tocilizumab on two diffuse SSc patients who had been resistant to conventional treatment regimens [115]. Six months after the treatment, both patients showed softening of the skin with reductions of 50.7% and 55.7% for the total z-score determined with the Vesmeter, a novel device for measuring the physical properties of the skin [116], and of 51.9% and 23% for the modified Rodnan total skin score. Histological examination showed thinning of the collagen fiber bundles and reduction of the number of α-SMA positive cells in the dermis. Since there are few therapeutic drugs for SSc at the present time [117], these improvements suggest that tocilizumab appears to be a promising biologic for the treatment of SSc.
3.3. Polymyositis
The inflammatory myopathies encompass a group of heterogenous muscle diseases which share the common clinical features of slowly progressive symmetrical muscle weakness, decreased muscle endurance, and fatigue [118]. They include polymyositis (PM), dermatomyositis, and inclusion body myositis, but are generally considered to be distinct diseases with different pathophysiological mechanisms. Muscles produce IL-6 [119], and IL-6 has been also shown to play a regulatory role in muscle wasting [120]. Among these inflammatory myopathies, PM appears to be another suitable target disease for tocilizumab. Excessive IL-6 expression has been found in the sera and infiltrating mononuclear cells in the muscles of PM patients [121–123]. Infiltrating cytotoxic T cells are thought to be involved in muscle fiber damage, and IL-6 functions as a helper factor in the induction of cytotoxic T cells [124]. Moreover, in a model of myosin-induced experimental myositis it was shown that control mice developed clinically manifest muscle damage, whereas IL-6-deficient mice showed no clinical or histological signs of muscle damage [125]. In another model of PM, known as C-protein-induced myositis, intraperitoneal administration of anti-IL-6R Ab suppressed the severity of myositis preventatively as well as therapeutically [126]. We tested the efficacy of tocilizumab in two PM patients who had been refractory to corticosteroids and immunosuppressive drugs [127]. Creatine phosphokinase levels of both patients normalized and MR images showed the disappearance of high-intensity zones in the thigh muscles. These findings suggest that tocilizumab may also be effective as a novel drug for refractory PM.
Dermatomyositis is a complement-mediated microangiopathy associated with destruction of capillaries, hypoperfusion, and inflammatory stress on the perifascicular regions, so that the pathology is different from that of PM [118]. Production of IL-6 and type I interferon signature genes was recently proposed as a biomarker for disease activity in childhood dermatomyositis [128], which thus may be another disorder suitable for tocilizumab targeting.
3.4. Takayasu's Arteritis and Giant Cell Arteritis
Vasculitis refers to inflammation where blood vessels are the primary site of inflammation. The pathological consequence of such inflammation is destruction of the vessel wall, which is histologically detected as fibrinoid necrosis. Takayasu's arteritis (TA) and giant cell arteritis (GCA) belong to an entity designated vasculitis syndrome, and involve both large and medium-sized arteries [129, 130]. The pathogenesis of TA and GCA remains unclear, but it is clear that IL-6 is involved in their development [129–133]. Tocilizumab treatment for a 20-year-old woman with refractory active TA improved the clinical manifestations and abnormal laboratory findings [134], and subsequent studies reported that tocilizumab treatment induced a rapid remission in 2 patients with TA and 5 patients with GCA [135]. Surprisingly, two of the patients with GCA went into remission without concomitant use of corticosteroids. Moreover, tocilizumab was also shown to be effective as rescue treatment for three GCA patients for whom the prednisone dose could not be tapered to less than 30 mg/day [136]. Positron emission tomography/CT scans revealed that in two patients generalized large-vessel vasculitis was detected during the active phase, which completely resolved upon a 6-month course of tocilizumab therapy. These reports strongly imply that IL-6 inhibition may serve as an innovative strategy for the treatment of both TA and GCA. However, several studies have suggested that GCA patients with a lesser inflammatory response without an increase in IL-6 expression were at a higher risk of developing ischemic manifestations than were other patients [137], since the angiogenic activity of IL-6 offers protection against ischemia in such GCA patients [138]. These findings indicate that further clinical studies are required to evaluate the efficacy and safety of tocilizumab for GCA and TA.
It is worthy of note that IL-6 has been also implicated in the development of other types of vasculitis syndrome such as polyarteritis nodosa (PAN) and antineutrophil-cytoplasmic-antibody- (ANCA) associated vasculitis [139–142]. However, so far there have been no reports about off-label use of tocilizumab for PAN or ANCA-associated vasculitis.
4. Therapeutic Implications for Other Autoimmune and Inflammatory Diseases
On the basis of excellent results of the efficacy of tocilizumab for Castleman's disease [143, 144] and systemic juvenile idiopathic arthritis [145–147], it has been approved and used as the first-line biologic in Japan. Pilot studies and case reports with off-label use of tocilizumab also indicate the potential indications of this biologic for various other organ-specific autoimmune and chronic inflammatory diseases. These include relapsing polychondritis [148], acquired hemophilia A [149], autoimmune hemolytic anemia [150], adult-onset Still's disease [151–165], Crohn's disease [166], Bechet's disease with posterior uveitis [167], polymyalgia rheumatica [135, 168], remitting seronegative, symmetrical synovitis with pitting edema [169], spondyloarthritides [170–175], graft-versus-host disease [176, 177], TNF-receptor-associated periodic syndrome [178], and pulmonary arterial hypertension complicated with Castleman's disease or mixed connective tissue disease [179–181]. Further clinical trials are essential, however, to evaluate the efficacy and safety of tocilizumab for these diseases.
5. Conclusion
Acute IL-6 synthesis provides a warning signal and protects the host from environmental stress, while its prolonged production causes the onset and progression of various autoimmune diseases. Several clinical trials have verified the efficacy and safety of tocilizumab for RA, systemic juvenile idiopathic arthritis and Castleman's disease, resulting in approval of this innovative biologic for the treatment of these diseases. Case reports of off-label use or pilot studies have also raised the possibility that tocilizumab could become the biological drug of choice for other systemic autoimmune diseases including SLE, systemic sclerosis, polymyositis and large vessel vasculitis. At present, the mechanisms through which tocilizumab exerts its clinical ameliorative effects on phenotypically different autoimmune diseases are not completely understood. IL-6 blockade may suppress autoantibody production or correct the imbalance of autoantigen-specific Th17 and/or Th1 versus Treg. Thus, clarification of the mechanisms as well as further clinical trials to evaluate the efficacy and safety of tocilizumab for these diseases are important issues.
Conflict of Interests
Toshio Tanaka declares no conflict of interests.
Acknowledgments
The authors thank Professor Tadamitsu Kishimoto, Professor Atsushi Kumanogoh, and Professor Kazuyuki Yoshizaki for valuable discussions, and Dr. Masashi Narazaki, Dr. Yoshihito Shima, Dr. Keisuke Hagihara, Dr. Toru Hirano, Dr. Junsuke Arimitsu, Dr. Sumiyuki Nishida, Dr. Mari Kawai, Dr. Taeko Ishii, Dr. Yusuke Kuwahara, Dr. Atsuyoshi Morishima, Dr. Yoshihiro Hishitani, Dr. Yuji Yoshida, and Dr. Akihiko Nakabayashi for their collaboration with off-label use of tocilizumab for various disorders at Osaka University Hospital. The clinical studies of tocilizumab were supported by a research grant of the Program of Fundamental Studies in Health Sciences of the National Institute of Biomedical Innovation. Atsushi Ogata has received a consulting fee as a medical adviser from Chugai Pharmaceutical Co., Ltd.
References
- 1.Hirano T, Yasukawa K, Harada H, et al. Complementary DNA for a novel human interleukin (BSF-2) that induces B lymphocytes to produce immunoglobulin. Nature. 1986;324(6092):73–76. doi: 10.1038/324073a0. [DOI] [PubMed] [Google Scholar]
- 2.Kishimoto T. The biology of interleukin-6. Blood. 1989;74(1):1–10. [PubMed] [Google Scholar]
- 3.Akira S, Taga T, Kishimoto T. Interleukin-6 in biology and medicine. Advances in Immunology. 1993;54:1–78. doi: 10.1016/s0065-2776(08)60532-5. [DOI] [PubMed] [Google Scholar]
- 4.Kishimoto T. Interleukin-6: from basic science to medicine-40 Years in immunology. Annual Review of Immunology. 2005;23:1–21. doi: 10.1146/annurev.immunol.23.021704.115806. [DOI] [PubMed] [Google Scholar]
- 5.Korn T, Bettelli E, Oukka M, Kuchroo VK. IL-17 and Th17 cells. Annual Review of Immunology. 2009;27:485–517. doi: 10.1146/annurev.immunol.021908.132710. [DOI] [PubMed] [Google Scholar]
- 6.Kimura A, Kishimoto T. IL-6: regulator of Treg/Th17 balance. European Journal of Immunology. 2010;40(7):1830–1835. doi: 10.1002/eji.201040391. [DOI] [PubMed] [Google Scholar]
- 7.Yamasaki K, Taga T, Hirata Y, et al. Cloning and expression of the human interleukin-6 (BSF-2/IFNβ 2) receptor. Science. 1988;241(4867):825–828. doi: 10.1126/science.3136546. [DOI] [PubMed] [Google Scholar]
- 8.Narazaki M, Yasukawa K, Saito T, et al. Soluble forms of the interleukin-6 signal-transducing receptor component gp130 in human serum possessing a potential to inhibit signals through membrane-anchored gp130. Blood. 1993;82(4):1120–1126. [PubMed] [Google Scholar]
- 9.Hibi M, Murakami M, Saito M, Hirano T, Taga T, Kishimoto T. Molecular cloning and expression of an IL-6 signal transducer, gp130. Cell. 1990;63(6):1149–1157. doi: 10.1016/0092-8674(90)90411-7. [DOI] [PubMed] [Google Scholar]
- 10.Hirano T, Taga T, Yasukawa K. Human B-cell differentiation factor defined by an anti-peptide antibody and its possible role in autoantibody production. Proceedings of the National Academy of Sciences of the United States of America. 1987;84(1):228–231. doi: 10.1073/pnas.84.1.228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yoshizaki K, Matsuda T, Nishimoto N, et al. Pathogenic significance of interleukin-6 (IL-6/BSF-2) in Castleman’s disease. Blood. 1989;74(4):1360–1367. [PubMed] [Google Scholar]
- 12.Hirano T, Matsuda T, Turner M, et al. Excessive production of interleukin 6/B cell stimulatory factor-2 in rheumatoid arthritis. European Journal of Immunology. 1988;18(11):1797–1801. doi: 10.1002/eji.1830181122. [DOI] [PubMed] [Google Scholar]
- 13.Nishimoto N, Kishimoto T. Interleukin 6: from bench to bedside. Nature Clinical Practice Rheumatology. 2006;2(11):619–626. doi: 10.1038/ncprheum0338. [DOI] [PubMed] [Google Scholar]
- 14.Tanaka T, Ogata A, Narazaki M. Tocilizumab for the treatment of rheumatoid arthritis. Expert Review of Clinical Immunology. 2010;6(6):843–854. doi: 10.1586/eci.10.70. [DOI] [PubMed] [Google Scholar]
- 15.Tanaka T, Narazaki M, Kishimoto T. Therapeutic targeting of the interleukin-6 receptor. Annual Review of Pharmacology and Toxicology. 2012;52:199–219. doi: 10.1146/annurev-pharmtox-010611-134715. [DOI] [PubMed] [Google Scholar]
- 16.Smolen JS, Aletaha D, Koeller M, Weisman MH, Emery P. New therapies for treatment of rheumatoid arthritis. The Lancet. 2007;370(9602):1861–1874. doi: 10.1016/S0140-6736(07)60784-3. [DOI] [PubMed] [Google Scholar]
- 17.Kotake S, Sato K, Kim KJ, et al. Interleukin-6 and soluble interleukin-6 receptors in the synovial fluids from rheumatoid arthritis patients are responsible for osteoclast-like cell formation. Journal of Bone and Mineral Research. 1996;11(1):88–95. doi: 10.1002/jbmr.5650110113. [DOI] [PubMed] [Google Scholar]
- 18.Palmqvist P, Persson E, Conaway HH, Lerner UH. IL-6, leukemia inhibitory factor, and oncostatin M stimulate bone resorption and regulate the expression of receptor activator of NF-κB ligand, osteoprotegerin, and receptor activator of NF-κB in mouse calvariae. Journal of Immunology. 2002;169(6):3353–3362. doi: 10.4049/jimmunol.169.6.3353. [DOI] [PubMed] [Google Scholar]
- 19.Hashizume M, Hayakawa N, Mihara M. IL-6 trans-signalling directly induces RANKL on fibroblast-like synovial cells and is involved in RANKL induction by TNF-α and IL-17. Rheumatology. 2008;47(11):1635–1640. doi: 10.1093/rheumatology/ken363. [DOI] [PubMed] [Google Scholar]
- 20.Nakahara H, Song J, Sugimoto M, et al. Anti-interleukin-6 receptor antibody therapy reduces vascular endothelial growth factor production in rheumatoid arthritis. Arthritis & Rheumatism. 2003;48(6):1521–1529. doi: 10.1002/art.11143. [DOI] [PubMed] [Google Scholar]
- 21.Houssiau FA, Devogelaer JP, Van Damme J, de Deuxchaisnes CN, Van Snick J. Interleukin-6 in synovial fluid and serum of patients with rheumatoid arthritis and other inflammatory arthritides. Arthritis & Rheumatism. 1988;31(6):784–788. doi: 10.1002/art.1780310614. [DOI] [PubMed] [Google Scholar]
- 22.Madhok R, Crilly A, Watson J, Capell HA. Serum interleukin 6 levels in rheumatoid arthritis: correlations with clinical and laboratory indices of disease activity. Annals of the Rheumatic Diseases. 1993;52(3):232–234. doi: 10.1136/ard.52.3.232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Alonzi T, Fattori E, Lazzaro D, et al. Interleukin 6 is required for the development of collagen-induced arthritis. Journal of Experimental Medicine. 1998;187(4):461–468. doi: 10.1084/jem.187.4.461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ohshima S, Saeki Y, Mima T, et al. Interleukin 6 plays a key role in the development of antigen-induced arthritis. Proceedings of the National Academy of Sciences of the United States of America. 1998;95(14):8222–8226. doi: 10.1073/pnas.95.14.8222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Takagi N, Mihara M, Moriya Y, et al. Blockage of interleukin-6 receptor ameliorates joint disease in murine collagen-induced arthritis. Arthritis & Rheumatism. 1998;41(12):2117–2121. doi: 10.1002/1529-0131(199812)41:12<2117::AID-ART6>3.0.CO;2-P. [DOI] [PubMed] [Google Scholar]
- 26.Sasai M, Saeki Y, Ohshima S, et al. Delayed onset and reduced severity of collagen-induced arthritis in interleukin-6-deficient mice. Arthritis & Rheumatism. 1999;42(8):1635–1643. doi: 10.1002/1529-0131(199908)42:8<1635::AID-ANR11>3.0.CO;2-Q. [DOI] [PubMed] [Google Scholar]
- 27.Mihara M, Kotoh M, Nishimoto N, et al. Humanized antibody to human interleukin-6 receptor inhibits the development of collagen arthritis in cynomolgus monkeys. Clinical Immunology. 2001;98(3):319–326. doi: 10.1006/clim.2000.4989. [DOI] [PubMed] [Google Scholar]
- 28.Uchiyama Y, Yorozu K, Hashizume M, Moriya Y, Mihara M. Tocilizumab, a humanized anti-interleukin-6 receptor antibody, ameliorates joint swelling in established monkey collagen-induced arthritis. Biological & Pharmaceutical Bulletin. 2008;31(6):1159–1163. doi: 10.1248/bpb.31.1159. [DOI] [PubMed] [Google Scholar]
- 29.Fujimoto M, Serada S, Mihara M, et al. Interleukin-6 blockade suppresses autoimmune arthritis in mice by the inhibition of inflammatory Th17 responses. Arthritis & Rheumatism. 2008;58(12):3710–3719. doi: 10.1002/art.24126. [DOI] [PubMed] [Google Scholar]
- 30.Iwanami K, Matsumoto I, Tanaka-Watanabe Y, et al. Crucial role of the interleukin-6/interleukin-17 cytokine axis in the induction of arthritis by glucose-6-phosphate isomerase. Arthritis & Rheumatism. 2008;58(3):754–763. doi: 10.1002/art.23222. [DOI] [PubMed] [Google Scholar]
- 31.Kagari T, Doi H, Shimozato T. The importance of IL-1β and TNF-α, and the noninvolvement of IL-6, in the development of monoclonal antibody-induced arthritis. Journal of Immunology. 2002;169(3):1459–1466. doi: 10.4049/jimmunol.169.3.1459. [DOI] [PubMed] [Google Scholar]
- 32.Iwakura Y, Nakae S, Saijo S, Ishigame H. The roles of IL-17A in inflammatory immune responses and host defense against pathogens. Immunological Reviews. 2008;226(1):57–79. doi: 10.1111/j.1600-065X.2008.00699.x. [DOI] [PubMed] [Google Scholar]
- 33.Ogata A, Umegaki N, Katayama I, Kumanogoh A, Tanaka T. Psoriatic arthritis in two patients with an inadequate response to treatment with tocilizumab. doi: 10.1016/j.jbspin.2011.06.011. Joint Bone Spine. In press. [DOI] [PubMed] [Google Scholar]
- 34.Nishimoto N, Hashimoto J, Miyasaka N, et al. Study of active controlled monotherapy used for rheumatoid arthritis, an IL-6 inhibitor (SAMURAI): evidence of clinical and radiographic benefit from an x-ray reader-blinded randomised controlled trial of tocilizumab. Annals of the Rheumatic Diseases. 2007;66(9):1162–1167. doi: 10.1136/ard.2006.068064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Genovese MC, McKay JD, Nasonov EL, et al. Interleukin-6 receptor inhibition with tocilizumab reduces disease activity in rheumatoid arthritis with inadequate response to disease-modifying antirheumatic drugs: the tocilizumab in combination with traditional disease-modifying antirheumatic drug therapy study. Arthritis & Rheumatism. 2008;58(10):2968–2980. doi: 10.1002/art.23940. [DOI] [PubMed] [Google Scholar]
- 36.Emery P, Keystone E, Tony HP, et al. IL-6 receptor inhibition with tocilizumab improves treatment outcomes in patients with rheumatoid arthritis refractory to anti-tumour necrosis factor biologicals: results from a 24-week multicentre randomised placebo-controlled trial. Annals of the Rheumatic Diseases. 2008;67(11):1516–1523. doi: 10.1136/ard.2008.092932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Smolen JS, Beaulieu A, Rubbert-Roth A, et al. Effect of interleukin-6 receptor inhibition with tocilizumab in patients with rheumatoid arthritis (OPTION study): a double-blind, placebo-controlled, randomised trial. The Lancet. 2008;371(9617):987–997. doi: 10.1016/S0140-6736(08)60453-5. [DOI] [PubMed] [Google Scholar]
- 38.Nishimoto N, Miyasaka N, Yamamoto K, et al. Study of active controlled tocilizumab monotherapy for rheumatoid arthritis patients with an inadequate response to methotrexate (SATORI): significant reduction in disease activity and serum vascular endothelial growth factor by IL-6 receptor inhibition therapy. Modern Rheumatology. 2009;19(1):12–19. doi: 10.1007/s10165-008-0125-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Jones G, Sebba A, Gu J, et al. Comparison of tocilizumab monotherapy versus methotrexate monotherapy in patients with moderate to severe rheumatoid arthritis: the AMBITION study. Annals of the Rheumatic Diseases. 2010;69(1):88–96. doi: 10.1136/ard.2008.105197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.M. Kremer J, Blanco R, Brzosko M, et al. Tocilizumab inhibits structural joint damage in rheumatoid arthritis patients with inadequate responses to methotrexate: results from the double-blind treatment phase of a randomized placebo-controlled trial of tocilizumab safety and prevention of structural joint damage at one year. Arthritis & Rheumatism. 2011;63(3):609–621. doi: 10.1002/art.30158. [DOI] [PubMed] [Google Scholar]
- 41.Singh JA, Beg S, Lopez-Olivo MA. Tocilizumab for rheumatoid arthritis. Cochrane Database of Systematic Reviews. 2010;7:p. CD008331. doi: 10.1002/14651858.CD008331.pub2. [DOI] [PubMed] [Google Scholar]
- 42.Nishimoto N, Takagi N. Assessment of the validity of the 28-joint disease activity score using erythrocyte sedimentation rate (DAS28-ESR) as a disease activity index of rheumatoid arthritis in the efficacy evaluation of 24-week treatment with tocilizumab: subanalysis of the SATORI study. Modern Rheumatology. 2010;20(6):539–547. doi: 10.1007/s10165-010-0328-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Smolen JS, Aletaha D. Interleukin-6 receptor inhibition with tocilizumab and attainment of disease remission in rheumatoid arthritis: the role of acute-phase reactants. Arthritis & Rheumatism. 2011;63(1):43–52. doi: 10.1002/art.27740. [DOI] [PubMed] [Google Scholar]
- 44.Burmester GR, Feist E, Kellner H, Braun J, Iking-Konert C, Rubbert-Roth A. Effectiveness and safety of the interleukin 6-receptor antagonist tocilizumab after 4 and 24 weeks in patients with active rheumatoid arthritis: the first phase IIIb real-life study (TAMARA) Annals of the Rheumatic Diseases. 2010;70(5):755–759. doi: 10.1136/ard.2010.139725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Iking-Konert C, Aringer M, Wollenhaupt J, et al. Performance of the new 2011 ACR/EULAR remission criteria with tocilizumab using the phase IIIb study TAMARA as an example and their comparison with traditional remission criteria. Annals of Rheumatic Diseases. 2011;70(11):1986–1990. doi: 10.1136/ard.2011.152678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.C. Leffers H, Ostergaard M, Glintborg B, et al. Efficacy of abatacept and tocilizumab in patients with rheumatoid arthritis treated in clinical practice: results from the nationwide Danish DANBIO registry. Annals of the Rheumatic Diseases. 2011;70(7):1216–1222. doi: 10.1136/ard.2010.140129. [DOI] [PubMed] [Google Scholar]
- 47.Yamanaka H, Tanaka Y, Inoue E, et al. Efficacy and tolerability of tocilizumab in rheumatoid arthritis patients seen in daily clinical practice in Japan: results from a retrospective study (REACTION study) Modern Rheumatology. 2010;21(2):122–133. doi: 10.1007/s10165-010-0366-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Takeuchi T, Tanaka Y, Amano K, et al. Clinical, radiographic and functional effectiveness of tocilizumab for rheumatoid arthritis patients-REACTION 52-week study. Rheumatology. 2011;50(10):1908–1915. doi: 10.1093/rheumatology/ker221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Nishimoto N, Ito K, Takagi N. Safety and efficacy profiles of tocilizumab monotherapy in Japanese patients with rheumatoid arthritis: meta-analysis of six initial trials and five long-term extensions. Modern Rheumatology. 2010;20(3):222–232. doi: 10.1007/s10165-010-0279-5. [DOI] [PubMed] [Google Scholar]
- 50.Campbell L, Chen C, Bhagat SS, Parker RA, Ostor AJ. Risk of adverse events including serious infections in rheumatoid arthritis patients treated with tocilizumab: a systemic literature review and meta-analysis of randomized controlled trials. Rheumatology. 2011;50(3):552–562. doi: 10.1093/rheumatology/keq343. [DOI] [PubMed] [Google Scholar]
- 51.Koike T, Harigai M, Inokuma S. Postmarketing surveillance of tocilizumab for rheumatoid arthritis in Japan: interim analysis of 3881 patients. Annals of the Rheumatic Diseases. 2011;70(12):2148–2151. doi: 10.1136/ard.2011.151092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Hashizume M, Yoshida H, Koike N, Suzuki M, Mihara M. Overproduced interleukin 6 decreases blood lipid levels via upregulation of very-low-density lipoprotein receptor. Annals of the Rheumatic Diseases. 2010;69(4):741–746. doi: 10.1136/ard.2008.104844. [DOI] [PubMed] [Google Scholar]
- 53.Ogata A, Morishima A, Hirano T, et al. Improvement of HbA1c during treatment with humanised anti-interleukin 6 receptor antibody, tocilizumab. Annals of the Rheumatic Diseases. 2011;70(6):1164–1165. doi: 10.1136/ard.2010.132845. [DOI] [PubMed] [Google Scholar]
- 54.Schultz O, Oberhauser F, Saech J, et al. Effects of inhibition of interleukin-6 signalling on insulin sensitivity and lipoprotein (A) levels in human subjects with rheumatoid diseases. PLoS One. 2010;5(12) doi: 10.1371/journal.pone.0014328. Article ID e14328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gout T, Ostör AJ, Nisar MK. Lower gastrointestinal perforation in rheumatoid arthritis patients treated with conventional DMARDs or tocilizumab: a systematic literature review. Clinical Rheumatology. 2011;30(11):1471–1474. doi: 10.1007/s10067-011-1827-x. [DOI] [PubMed] [Google Scholar]
- 56.Gomez-Reino JJ, Carmona L, Valverde VR, Mola EM, Montero MD. Treatment of rheumatoid arthritis with tumor necrosis factor inhibitors may predispose to significant increase in tuberculosis risk: a multicenter active-surveillance report. Arthritis & Rheumatism. 2003;48(8):2122–2127. doi: 10.1002/art.11137. [DOI] [PubMed] [Google Scholar]
- 57.Okada M, Kita Y, Kanamaru N, et al. Anti-IL-6 receptor antibody causes less promotion of tuberculosis infection than anti-TNF-α antibody in mice. Clinical and Developmental Immunology. 2011;2011:9 pages. doi: 10.1155/2011/404929. Article ID 404929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Ogata A, Mori M, Hashimoto S, et al. Minimal influence of tocilizumab on IFN-γ synthesis by tuberculosis antigens. Modern Rheumatology. 2010;20(2):130–133. doi: 10.1007/s10165-009-0243-4. [DOI] [PubMed] [Google Scholar]
- 59.Perfetto F, Moggi-Pignone A, Livi R, Tempestini A, Bergesio F, Matucci-Cerinic M. Systemic amyloidosis: a challenge for the rheumatologist. Nature Reviews Rheumatology. 2010;6(7):417–429. doi: 10.1038/nrrheum.2010.84. [DOI] [PubMed] [Google Scholar]
- 60.Tanaka T, Hagihara K, Hishitani Y, Ogata A. In: Amyloidosis—An Insight to Disease Systems and Novel Therapies. chapter 11. Guvenc IA, editor. Croatia: INTECH Open Access Publisher; 2011. [Google Scholar]
- 61.Hagihara K, Nishikawa T, Isobe T, Song J, Sugamata Y, Yoshizaki K. IL-6 plays a critical role in the synergistic induction of human serum amyloid a (SAA) gene when stimulated with proinflammatory cytokines as analyzed with an SAA isoform real-time quantitative RT-PCR assay system. Biochemical and Biophysical Research Communications. 2004;314(2):363–369. doi: 10.1016/j.bbrc.2003.12.096. [DOI] [PubMed] [Google Scholar]
- 62.Hagihara K, Nishikawa T, Sugamata Y, et al. Essential role of STAT3 in cytokine-driven NF-κB-mediated serum amyloid A gene expression. Genes to Cells. 2005;10(11):1051–1063. doi: 10.1111/j.1365-2443.2005.00900.x. [DOI] [PubMed] [Google Scholar]
- 63.Nishida S, Hagihara K, Shima Y, et al. Rapid improvement of AA amyloidosis with humanised anti-interleukin 6 receptor antibody treatment. Annals of the Rheumatic Diseases. 2009;68(7):1235–1236. doi: 10.1136/ard.2008.099267. [DOI] [PubMed] [Google Scholar]
- 64.Sato H, Sakai T, Sugaya T, et al. Tocilizumab dramatically ameliorated life-threatening diarrhea due to secondary amyloidosis associated with rheumatoid arthritis. Clinical Rheumatology. 2009;28(9):1113–1116. doi: 10.1007/s10067-009-1185-0. [DOI] [PubMed] [Google Scholar]
- 65.Inoue D, Arima H, Kawanami C, et al. Excellent therapeutic effect of tocilizumab on intestinal amyloid a deposition secondary to active rheumatoid arthritis. Clinical Rheumatology. 2010;29(10):1195–1197. doi: 10.1007/s10067-010-1422-6. [DOI] [PubMed] [Google Scholar]
- 66.van den Broek M, Huizinga TW, Dijkmans BA, Allaart CF. Drug-free remission: is it already possible? Current Opinion in Rheumatology. 2011;23(3):266–272. doi: 10.1097/BOR.0b013e32834563e3. [DOI] [PubMed] [Google Scholar]
- 67.Nishimoto N, Japanese MRA study group for RA Drug free remission after cessation of actemra monotherapy (DREAM Study). In: Proceedings of the Annual European League Against Rheumatism Conference (EULAR '10); Rome, Italy. [Google Scholar]
- 68.Nishimoto N, Japanese MRA study group for RA Retreatment efficacy and safety to tocilizumab in patients with rheumatoid arthritis at recurrence (RESTORE study). In: Proceedings of the Annual European League Against Rheumatism Conference (EULAR '10); Rome, Italy. [Google Scholar]
- 69.Ruiz-Irastorza G, Khamashta MA, Castellino G, Hughes GRV. Systemic lupus erythematosus. The Lancet. 2001;357(9261):1027–1032. doi: 10.1016/S0140-6736(00)04239-2. [DOI] [PubMed] [Google Scholar]
- 70.Munoz LE, Lauber K, Schiller M, Manfredi AA, Herrmann M. The role of defective clearance of apoptotic cells in systemic autoimmunity. Nature Reviews Rheumatology. 2010;6(5):280–289. doi: 10.1038/nrrheum.2010.46. [DOI] [PubMed] [Google Scholar]
- 71.Obermoser G, Pascual V. The interferon-α signature of systemic lupus erythematosus. Lupus. 2010;19(9):1012–1019. doi: 10.1177/0961203310371161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Shin MS, Lee N, Kang I. Effector T-cell subsets in systemic lupus erythematosus: update focusing on Th17 cells. Current Opinion in Rheumatology. 2011;23(5):444–448. doi: 10.1097/BOR.0b013e328349a255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Rhodes B, Furnrohr BG, Vyse TJ. C-reactive protein in rheumatology: biology and genetics. Nature Reviews Rheumatology. 2011;7(5):282–289. doi: 10.1038/nrrheum.2011.37. [DOI] [PubMed] [Google Scholar]
- 74.Tackey E, Lipsky PE, Illei GG. Rationale for interleukin-6 blockade in systemic lupus erythematosus. Lupus. 2004;13(5):339–343. doi: 10.1191/0961203304lu1023oa. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Linker-Israeli M, Deans RJ, Wallace DJ, Prehn J, Ozeri-Chen T, Klinenberg JR. Elevated levels of endogenous IL-6 in systemic lupus erythematosus: a putative role in pathogenesis. Journal of Immunology. 1991;147(1):117–123. [PubMed] [Google Scholar]
- 76.Peterson E, Robertson AD, Emlen W. Serum and urinary interleukin-6 in systemic lupus erythematosus. Lupus. 1996;5(6):571–575. doi: 10.1177/096120339600500603. [DOI] [PubMed] [Google Scholar]
- 77.Grondal G, Gunnarsson I, Ronnelid J, Rogberg S, Klareskog L, Lundberg I. Cytokine production, serum levels and disease activity in systemic lupus erythematosus. Clinical and Experimental Rheumatology. 2000;18(5):565–570. [PubMed] [Google Scholar]
- 78.Iwano M, Dohi K, Hirata E, et al. Urinary levels of IL-6 in patients with active lupus nephritis. Clinical Nephrology. 1993;40(1):16–21. [PubMed] [Google Scholar]
- 79.Malide D, Russo P, Bendayan M. Presence of tumor necrosis factor alpha and interleukin-6 in renal mesangial cells of lupus nephritis patients. Human Pathology. 1995;26(5):558–564. doi: 10.1016/0046-8177(95)90253-8. [DOI] [PubMed] [Google Scholar]
- 80.Herrera-Esparza R, Barbosa-Cisneros O, Villalobos-Hurtado R, Avalos-Díaz E. Renal expression of IL-6 and TNFα genes in lupus nephritis. Lupus. 1998;7(3):154–158. doi: 10.1191/096120398678919949. [DOI] [PubMed] [Google Scholar]
- 81.Tsai CY, Wu TH, Yu CL, Lu JY, Tsai YY. Increased excretions of β2-microglobulin, IL-6, and IL-8 and decreased excretion of Tamm-Horsfall glycoprotein in urine of patients with active lupus nephritis. Nephron. 2000;85(3):207–214. doi: 10.1159/000045663. [DOI] [PubMed] [Google Scholar]
- 82.Hirohata S, Miyamoto T. Elevated levels of interleukin-6 in cerebrospinal fluid from patients with systemic lupus erythematosus and central nervous system involvement. Arthritis & Rheumatism. 1990;33(5):644–649. doi: 10.1002/art.1780330506. [DOI] [PubMed] [Google Scholar]
- 83.Hagiwara E, Gourley MF, Lee S, Klinman DM. Disease severity in patients with systemic lupus erythematosus correlates with an increased ratio of interleukin-10: interferon-γ-secreting cells in the peripheral blood. Arthritis & Rheumatism. 1996;39(3):379–385. doi: 10.1002/art.1780390305. [DOI] [PubMed] [Google Scholar]
- 84.Swaak AJG, van den Brink HG, Aarden LA. Cytokine production (IL-6 and TNFα) in whole blood cell cultures of patients with systemic lupus erythematosus. Scandinavian Journal of Rheumatology. 1996;25(4):233–238. doi: 10.3109/03009749609069992. [DOI] [PubMed] [Google Scholar]
- 85.Klashman DJ, Martin RA, Martinez-Maza O, Stevens RH. In vitro regulation of B cell differentiation by interleukin-6 and soluble CD23 in systemic lupus erythematosus B cell subpopulations and antigen-induced normal B cells. Arthritis & Rheumatism. 1991;34(3):276–286. doi: 10.1002/art.1780340305. [DOI] [PubMed] [Google Scholar]
- 86.Kitani A, Hara M, Hirose T, et al. Autostimulatory effects of IL-6 on excessive B cell differentiation in patients with systemic lupus erythematosus: analysis of IL-6 production and IL-6R expression. Clinical and Experimental Immunology. 1992;88(1):75–83. doi: 10.1111/j.1365-2249.1992.tb03042.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Suzuki H, Yasukawa K, Saito T, et al. Serum soluble interleukin-6 receptor in MRL/lpr mice is elevated with age and mediates the interleukin-6 signal. European Journal of Immunology. 1993;23(5):1078–1082. doi: 10.1002/eji.1830230515. [DOI] [PubMed] [Google Scholar]
- 88.Tang B, Matsuda T, Akira S, et al. Age-associated increase in interleukin 6 in MRL/lpr mice. International Immunology. 1991;3(3):273–278. doi: 10.1093/intimm/3.3.273. [DOI] [PubMed] [Google Scholar]
- 89.Alarcon-Riquelme ME, Moller G, Fernandez C. Age-dependent responsiveness to interleukin-6 in B lymphocytes from a systemic lupus erythematosus-prone (NZB x NZW)F1 hybrid. Clinical Immunology and Immunopathology. 1992;62(3):264–269. doi: 10.1016/0090-1229(92)90101-s. [DOI] [PubMed] [Google Scholar]
- 90.Mihara M, Fukui H, Koishihara Y, Saito M, Ohsugi Y. Immunologic abnormality in NZB/W F1 mice. Thymus-independent expansion of B cells responding to interleukin-6. Clinical & Experimental Immunology. 1990;82(3):533–537. doi: 10.1111/j.1365-2249.1990.tb05485.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Mihara M, Ohsugi Y. Possible role of IL-6 in pathogenesis of immune complex-mediated glomerulonephritis in NZB/W F1 mice: induction of IgG class anti-DNA autoantibody production. International Archives of Allergy & Applied Immunology. 1990;93(1):89–92. doi: 10.1159/000235285. [DOI] [PubMed] [Google Scholar]
- 92.Ryffel B, Car BD, Gunn H, Roman D, Hiestand P, Mihatsch MJ. Interleukin-6 exacerbates glomerulonephritis in (NZBxNZW)F1 mice. American Journal of Pathology. 1994;144(5):927–937. [PMC free article] [PubMed] [Google Scholar]
- 93.Finck BK, Chan B, Wofsy D. Interleukin 6 promotes murine lupus in NZB/NZW F1 mice. Journal of Clinical Investigation. 1994;94(2):585–591. doi: 10.1172/JCI117373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Mihara M, Takagi N, Takeda Y, Ohsugi Y. IL-6 receptor blockage inhibits the onset of autoimmune kidney disease in NZB/WF1 mice. Clinical and Experimental Immunology. 1998;112(3):397–402. doi: 10.1046/j.1365-2249.1998.00612.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Liang B, Gardner DB, Griswold DE, Bugelski PJ, Song XYR. Anti-interleukin-6 monoclonal antibody inhibits autoimmune responses in a murine model of systemic lupus erythematosus. Immunology. 2006;119(3):296–305. doi: 10.1111/j.1365-2567.2006.02433.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Pflegerl P, Vesely P, Hantusch B, et al. Epidermal loss of JunB leads to a SLE phenotype due to hyper IL-6 signaling. Proceedings of the National Academy of Sciences of the United States of America. 2009;106(48):20423–20428. doi: 10.1073/pnas.0910371106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Illei GG, Shirota Y, Yarboro CH, et al. Tocilizumab in systemic lupus erythematosus: data on safety, preliminary efficacy, and impact on circulating plasma cells from an open-label phase I dosage-escalation study. Arthritis & Rheumatism. 2010;62(2):542–552. doi: 10.1002/art.27221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Gabrielli A, Avvedimento EV, Krieg T. Mechanisms of disease: Scleroderma. New England Journal of Medicine. 2009;360(19):1989–2003. doi: 10.1056/NEJMra0806188. [DOI] [PubMed] [Google Scholar]
- 99.Barnes TC, Anderson ME, Moots RJ. The many faces of interleukin-6 (IL-6): the role of IL-6 in inflammation, vasculopathy and fibrosis in systemic sclerosis. International Journal of Rheumatology. 2011;2011:6 pages. doi: 10.1155/2011/721608. Article ID 721608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Hasegawa M, Sato S, Fujimoto M, Ihn H, Kikuchi K, Takehara K. Serum levels of interleukin 6 (IL-6), oncostatin M, soluble IL-6 receptor, and soluble gp130 in patients with systemic sclerosis. Journal of Rheumatology. 1998;25(2):308–313. [PubMed] [Google Scholar]
- 101.Sato S, Hasegawa M, Takehara K. Serum levels of interleukin-6 and interleukin-10 correlate with total skin thickness score in patients with systemic sclerosis. Journal of Dermatological Science. 2001;27(2):140–146. doi: 10.1016/s0923-1811(01)00128-1. [DOI] [PubMed] [Google Scholar]
- 102.Scala E, Pallotta S, Frezzolini A, et al. Cytokine and chemokine levels in systemic sclerosis: relationship with cutaneous and internal organ involvement. Clinical & Experimental Immunology. 2004;138(3):540–546. doi: 10.1111/j.1365-2249.2004.02642.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Matsushita T, Hasegawa M, Hamaguchi Y, Takehara K, Sato S. Longitudinal analysis of serum cytokine concentrations in systemic sclerosis: association of interleukin 12 elevation with spontaneous regression of skin sclerosis. Journal of Rheumatology. 2006;33(2):275–284. [PubMed] [Google Scholar]
- 104.Gourh P, Arnett FC, Assassi S, et al. Plasma cytokine profiles in systemic sclerosis: associations with autoantibody subsets and clinical manifestations. Arthritis Research & Therapy. 2009;11(5):p. R147. doi: 10.1186/ar2821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Feghali CA, Bost KL, Boulware DW, Levy LS. Mechanisms of pathogenesis in scleroderma. I. Overproduction of interleukin 6 by fibroblasts cultured from affected skin sites of patients with scleroderma. Journal of Rheumatology. 1992;19(8):1207–1211. [PubMed] [Google Scholar]
- 106.Koch AE, Kronfeld-Harrington LB, Szekanecz Z, et al. In situ expression of cytokines and cellular adhesion molecules in the skin of patients with systemic sclerosis. Their role in early and late disease. Pathobiology. 1993;61(5-6):239–246. doi: 10.1159/000163802. [DOI] [PubMed] [Google Scholar]
- 107.Gurram M, Pahwa S, Frieri M. Augmented interleukin-6 secretion in collagen-stimulated peripheral blood mononuclear cells from patients with systemic sclerosis. Annals of Allergy Asthma & Immunology. 1994;73(6):493–496. [PubMed] [Google Scholar]
- 108.Zurita-Salinas CS, Richaud-Patin Y, Krotzsch-Gomez E, et al. Spontaneous cytokine gene expression by cultured skin fibroblasts of systemic sclerosis. Correlation with collagen synthesis. Revista de Investigacion Clinics. 1998;50(2):97–104. [PubMed] [Google Scholar]
- 109.Kadono T, Kikuchi K, Ihn H, Takehara K, Tamaki K. Increased production of interleukin 6 and interleukin 8 in scleroderma fibroblasts. Journal of Rheumatology. 1998;25(2):296–301. [PubMed] [Google Scholar]
- 110.Duncan MR, Berman B. Stimulation of collagen and glycosaminoglycan production in cultured human adult dermal fibroblasts by recombinant human interleukin 6. Journal of Investigative Dermatology. 1991;97(4):686–692. doi: 10.1111/1523-1747.ep12483971. [DOI] [PubMed] [Google Scholar]
- 111.Gallucci RM, Lee EG, Tomasek JJ. IL-6 modulates alpha-smooth muscle actin expression in dermal fibroblasts from IL-6-deficient mice. Journal of Investigative Dermatology. 2006;126(3):561–568. doi: 10.1038/sj.jid.5700109. [DOI] [PubMed] [Google Scholar]
- 112.Kawaguchi Y, Hara M, Wright TM. Endogenous IL-1α from systemic sclerosis fibroblasts induces IL-6 and PDGF-A. Journal of Clinical Investigation. 1999;103(9):1253–1260. doi: 10.1172/JCI4304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Barnes TC, Spiller DG, Anderson ME, Edwards SW, Moots RJ. Endothelial activation and apoptosis mediated by neutrophil-dependent interleukin 6 trans-signalling: a novel target for systemic sclerosis? Annals of the Rheumatic Diseases. 2010;70(2):366–372. doi: 10.1136/ard.2010.133587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Yoshizaki A, Yanaba K, Ogawa A, Asano Y, Kadono T, Sato S. Immunization with DNA topoisomerase I and complete Freund’s adjuvant induces skin and lung fibrosis and autoimmunity via interleukin-6 signaling. Arthritis & Rheumatism. 2011;63(11):3575–3585. doi: 10.1002/art.30539. [DOI] [PubMed] [Google Scholar]
- 115.Shima Y, Kuwahara Y, Murota H, et al. The skin of patients with systemic sclerosis softened during the treatment with anti-IL-6 receptor antibody tocilizumab. Rheumatology. 2010;49(12):2408–2412. doi: 10.1093/rheumatology/keq275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Kuwahara Y, Shima Y, Shirayama D, et al. Quantification of hardness, elasticity and viscosity of the skin of patients with systemic sclerosis using a novel sensing device (Vesmeter): a proposal for a new outcome measurement procedure. Rheumatology. 2008;47(7):1018–1024. doi: 10.1093/rheumatology/ken145. [DOI] [PubMed] [Google Scholar]
- 117.Kowal-Bielecka O, Landewe R, Chwiesko S, et al. EULAR recommendations for the treatment of systemic sclerosis: a report from the EULAR scleroderma trials and research group (EUSTAR) Annals of the Rheumatic Diseases. 2009;68(5):620–628. doi: 10.1136/ard.2008.096677. [DOI] [PubMed] [Google Scholar]
- 118.Dalakas MC. Immunotherapy of myositis: issues, concerns and future prospects. Nature Reviews Rheumatology. 2010;6(3):129–137. doi: 10.1038/nrrheum.2010.2. [DOI] [PubMed] [Google Scholar]
- 119.Pedersen BK, Febbraio MA. Muscle as an endocrine organ: focus on muscle-derived interleukin-6. Physiological Reviews. 2008;88(4):1379–1406. doi: 10.1152/physrev.90100.2007. [DOI] [PubMed] [Google Scholar]
- 120.Carson JA, Baltgalvis KA. Interleukin 6 as a key regulator of muscle mass during cachexia. Exercise and Sport Sciences Reviews. 2010;38(4):168–176. doi: 10.1097/JES.0b013e3181f44f11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Gabay C, Gay-Croisier F, Roux-Lombard P, et al. Elevated serum levels of interleukin-1 receptor antagonist in polymyositis/dermatomyositis: a biologic marker of disease activity with a possible role in the lack of acute-phase protein response. Arthritis & Rheumatism. 1994;37(12):1744–1751. doi: 10.1002/art.1780371206. [DOI] [PubMed] [Google Scholar]
- 122.Lundberg I, Ulfgren AK, Nyberg P, Andersson U, Klareskog L. Cytokine production in muscle tissue of patients with idiopathic inflammatory myopathies. Arthritis & Rheumatism. 1997;40(5):865–874. doi: 10.1002/art.1780400514. [DOI] [PubMed] [Google Scholar]
- 123.Lepidi H, Frances V, Figarella-Branger D, Bartoli C, Machado-Baeta A, Pellissier JF. Local expression of cytokines in idiopathic inflammatory myopathies. Neuropathology and Applied Neurobiology. 1998;24(1):73–79. doi: 10.1046/j.1365-2990.1998.00092.x. [DOI] [PubMed] [Google Scholar]
- 124.Okada M, Kitahara M, Kishimoto S, Matsuda T, Hirano T, Kishimoto T. IL-6/BSF-2 functions as a killer helper factor in the in vitro induction of cytotoxic T cells. Journal of Immunology. 1988;141(5):1543–1549. [PubMed] [Google Scholar]
- 125.Scuderi F, Mannella F, Marino M, Provenzano C, Bartoccioni E. IL-6-deficient mice show impaired inflammatory response in a model of myosin-induced experimental myositis. Journal of Neuroimmunology. 2006;176(1-2):9–15. doi: 10.1016/j.jneuroim.2006.03.026. [DOI] [PubMed] [Google Scholar]
- 126.Okiyama N, Sugihara T, Iwakura Y, Yokozeki H, Miyasaka N, Kohsaka H. Therapeutic effects of interleukin-6 blockade in a murine model of polymyositis that does not require interleukin-17A. Arthritis & Rheumatism. 2009;60(8):2505–2512. doi: 10.1002/art.24689. [DOI] [PubMed] [Google Scholar]
- 127.Narazaki M, Hagihara K, Shima Y, et al. Therapeutic effect of tocilizumab on two patients with polymyositis. Rheumatology. 2011;50(7):1344–1346. doi: 10.1093/rheumatology/ker152. [DOI] [PubMed] [Google Scholar]
- 128.Bilgic H, Ytterberg SR, Amin S, et al. Interleukin-6 and type I interferon-regulated genes and chemokines Mark disease activity in dermatomyositis. Arthritis & Rheumatism. 2009;60(11):3436–3446. doi: 10.1002/art.24936. [DOI] [PubMed] [Google Scholar]
- 129.Mason JC. Takayasu arteritis—advances in diagnosis and management. Nature Reviews Rheumatology. 2010;6(7):406–415. doi: 10.1038/nrrheum.2010.82. [DOI] [PubMed] [Google Scholar]
- 130.Salvarani C, Cantini F, Hunder GG. Polymyalgia rheumatica and giant-cell arteritis. The Lancet. 2008;372(9634):234–245. doi: 10.1016/S0140-6736(08)61077-6. [DOI] [PubMed] [Google Scholar]
- 131.Seko Y, Sato O, Takag A. Restricted usage of T-cell receptor Valpha-Vbeta genes in infiltrating cells in aortic tissue of patients with Takayasu’s arteritis. Circulation. 1996;93(10):1788–1790. doi: 10.1161/01.cir.93.10.1788. [DOI] [PubMed] [Google Scholar]
- 132.Noris M, Daina E, Gamba S, Bonazzola S, Remuzzi G. Interleukin-6 and RANTES in Takayasu arteritis a guide for therapeutic decisions? Circulation. 1999;100(1):55–60. doi: 10.1161/01.cir.100.1.55. [DOI] [PubMed] [Google Scholar]
- 133.Park MC, Lee SW, Park YB, Lee SK. Serum cytokine profiles and their correlations with disease activity in Takayasu’s arteritis. Rheumatology. 2006;45(5):545–548. doi: 10.1093/rheumatology/kei266. [DOI] [PubMed] [Google Scholar]
- 134.Nishimoto N, Nakahara H, Yoshio-Hoshino N, Mima T. Successful treatment of a patient with Takayasu arteritis using a humanized anti-interleukin-6 receptor antibody. Arthritis & Rheumatism. 2008;58(4):1197–1200. doi: 10.1002/art.23373. [DOI] [PubMed] [Google Scholar]
- 135.Seitz M, Reichenbach S, M. Bonel H, et al. Rapid induction of remission in large vessel vasculitis by IL-6 blockade. A case series. Swiss Medical Weekly. 2011;141 doi: 10.4414/smw.2011.13156. Article ID w13156. [DOI] [PubMed] [Google Scholar]
- 136.Beyer C, Axmann R, Sahinbegovic E. Anti-interleukin 6 receptor therapy as rescue treatment for giant cell arteritis. Annals of the Rheumatic Diseases. 2011;70(10):1874–1875. doi: 10.1136/ard.2010.149351. [DOI] [PubMed] [Google Scholar]
- 137.Cid MC, Hernandez-Rodriquez J, Esteban MJ, et al. Tissue and serum angiogenic activity is associated with low prevalence of ischemic complications in patients with giant-cell arteritis. Circulation. 2002;106(13):1664–1671. doi: 10.1161/01.cir.0000030185.67510.c0. [DOI] [PubMed] [Google Scholar]
- 138.Hernandez-Rodriquez J, Segarra M, Vilardell C, et al. Elevated production of interleukin-6 is associated with a lower incidence of disease-related ischemic events in patients with giant-cell arteritis: angiogenic activity of interleukin-6 as a potential protective mechanism. Circulation. 2003;107(19):2428–2434. doi: 10.1161/01.CIR.0000066907.83923.32. [DOI] [PubMed] [Google Scholar]
- 139.Nakahama H, Okada M, Miyazaki M, Imai N, Yokokawa T, Kubori S. Distinct responses of interleukin-6 and other laboratory parameters to treatment in a patient with polyarteritis nodosa: a case report. Angiology. 1992;43(6):512–516. doi: 10.1177/000331979204300610. [DOI] [PubMed] [Google Scholar]
- 140.Muller Kobold AC, Van Wijk RT, Franssen CFM, Molema G, Kallenberg CGM, Cohen Tervaert JW. In vitro up-regulation of E-selectin and induction of interleukin-6 in endothelial cells by autoantibodies in Wegener’s granulomatosis and microscopic polyangiitis. Clinical and Experimental Rheumatology. 1999;17(4):433–440. [PubMed] [Google Scholar]
- 141.Popa ER, Franssen CFM, Limburg PC, Huitema MG, Kallenberg CGM, Cohen Tervaert JW. In vitro cytokine production and proliferation of T cells from patients with anti-proteinase 3- and antimyeloperoxidase-associated vasculitis, in response to proteinase 3 and myeloperoxidase. Arthritis & Rheumatism. 2002;46(7):1894–1904. doi: 10.1002/art.10384. [DOI] [PubMed] [Google Scholar]
- 142.Ohlsson S, Bakoush O, Tencer J, Torffvit O, Segelmark M. Monocyte chemoattractant protein 1 is a prognostic marker in ANCA-associated small vessel vasculitis. Mediators of Inflammation. 2009;2009 doi: 10.1155/2009/584916. Article ID 584916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Nishimoto N, Sasai M, Shima Y, et al. Improvement in Castleman’s disease by humanized anti-interleukin-6 receptor antibody therapy. Blood. 2000;95(1):56–61. [PubMed] [Google Scholar]
- 144.Nishimoto N, Kanakura Y, Aozasa K, et al. Humanized anti-interleukin-6 receptor antibody treatment of multicentric Castleman disease. Blood. 2005;106(8):2627–2632. doi: 10.1182/blood-2004-12-4602. [DOI] [PubMed] [Google Scholar]
- 145.Yokota S, Miyamae T, Imagawa T, et al. Therapeutic efficacy of humanized recombinant anti-interleukin-6 receptor antibody in children with systemic-onset juvenile idiopathic arthritis. Arthritis & Rheumatism. 2005;52(3):818–825. doi: 10.1002/art.20944. [DOI] [PubMed] [Google Scholar]
- 146.Yokota S, Imagawa T, Mori M, et al. Efficacy and safety of tocilizumab in patients with systemic-onset juvenile idiopathic arthritis: a randomised, double-blind, placebo-controlled, withdrawal phase III trial. The Lancet. 2008;371(9617):998–1006. doi: 10.1016/S0140-6736(08)60454-7. [DOI] [PubMed] [Google Scholar]
- 147.De Benedetti F, Brunner H, Ruperto N, et al. From biology to classification and targeted therapy in juvenile idiopathic arthritis. Annals of the Rheumatic Diseases. 2010;69(supplement 3):p. 146. [Google Scholar]
- 148.Kawai M, Hagihara K, Hirano T, et al. Sustained response to tocilizumab, anti-interleukin-6 receptor antibody, in two patients with refractory relapsing polychondritis. Rheumatology. 2009;48(3):318–319. doi: 10.1093/rheumatology/ken468. [DOI] [PubMed] [Google Scholar]
- 149.Nishida S, Kawasaki T, Kashiwagi H, et al. Successful treatment of acquired hemophilia A, complicated by chronic GVHD, with tocilizumab. Modern Rheumatology. 2011;21(4):420–422. doi: 10.1007/s10165-010-0411-6. [DOI] [PubMed] [Google Scholar]
- 150.Yuzuriha A, Saitoh T, Koiso H, et al. Successful treatment of autoimmune hemolytic anemia associated with multicentric Castleman disease by anti-interleukin-6 receptor antibody (tocilizumab) therapy. Acta Haematologica. 2011;126(3):147–150. doi: 10.1159/000328426. [DOI] [PubMed] [Google Scholar]
- 151.Iwamoto M, Nara H, Hirata D, Minota S, Nishimoto N, Yoshizaki K. Humanized monoclonal anti-interleukin-6 receptor antibody for treatment of intractable adult-onset Still’s disease. Arthritis & Rheumatism. 2002;46(12):3388–3389. doi: 10.1002/art.10620. [DOI] [PubMed] [Google Scholar]
- 152.Nakahara H, Mima T, Yoshio-Hoshino N, Matsushita M, Hashimoto J, Nishimoto N. A case report of a patient with refractory adult-onset Still’s disease who was successfully treated with tocilizumab over 6 years. Modern Rheumatology. 2009;19(1):69–72. doi: 10.1007/s10165-008-0116-2. [DOI] [PubMed] [Google Scholar]
- 153.De Bandt M, Saint-Marcoux B. Tocilizumab for multirefractory adult-onset Still’s disease. Annals of the Rheumatic Diseases. 2009;68(1):153–154. doi: 10.1136/ard.2008.088179. [DOI] [PubMed] [Google Scholar]
- 154.Matsumoto K, Nagashima T, Takatori S, et al. Glucocorticoid and cyclosporine refractory adult onset Still’s disease successfully treated with tocilizumab. Clinical Rheumatology. 2009;28(4):485–487. doi: 10.1007/s10067-009-1097-z. [DOI] [PubMed] [Google Scholar]
- 155.Cunha ML, Wagner J, Osawa A, Scheinberg M. The effect of tocilizumab on the uptake of 18FDG-PET imaging in patients with adult-onset Still’s disease. Rheumatology. 2010;49(5):1014–1016. doi: 10.1093/rheumatology/kep441. [DOI] [PubMed] [Google Scholar]
- 156.Sumida K, Ubara Y, Hoshino J, et al. Etanercept-refractory adult-onset Still’s disease with thrombotic thrombocytopenic purpura successfully treated with tocilizumab. Clinical Rheumatology. 2010;29(10):1191–1194. doi: 10.1007/s10067-010-1418-2. [DOI] [PubMed] [Google Scholar]
- 157.Yoshimura M, Makiyama J, Koga T, et al. Successful treatment with tocilizumab in a patient with refractory adult-onset Still’s disease (AOSD) Clinical and Experimental Rheumatology. 2010;28(1):141–142. [PubMed] [Google Scholar]
- 158.Perdan-Pirkmajer K, Praprotnik S, Tomšič M. A case of refractory adult-onset Still’s disease successfully controlled with tocilizumab and a review of the literature. Clinical Rheumatology. 2010;29(12):1465–1467. doi: 10.1007/s10067-010-1553-9. [DOI] [PubMed] [Google Scholar]
- 159.Naniwa T, Ito R, Watanabe M, et al. Case report: successful use of short-term add-on tocilizumab for multirefractory systemic flare of adult-onset Still’s disease. doi: 10.1007/s10067-010-1562-8. Clinical Rheumatology. In press. [DOI] [PubMed] [Google Scholar]
- 160.Kishida D, Okuda Y, Onishi M, et al. Successful tocilizumab treatment in a patient with adult-onset Still’s disease complicated by chronic active hepatitis B and amyloid A amyloidosis. Modern Rheumatology. 2010;21(2):215–218. doi: 10.1007/s10165-010-0365-8. [DOI] [PubMed] [Google Scholar]
- 161.Thonhofer R, Hiller M, Just H, Trummer M, Siegel C, Dejaco C. Treatment of refractory adult-onset Still’s disease with tocilizumab: report of two cases and review of the literature. Rheumatology International. 2011;31(12):1653–1656. doi: 10.1007/s00296-010-1631-y. [DOI] [PubMed] [Google Scholar]
- 162.Kobayashi M, Takahashi Y, Yamashita H, Kaneko H, Mimori A. Benefit and a possible risk of tocilizumab therapy for adult-onset Still’s disease accompanied by macrophage-activation syndrome. Modern Rheumatology. 2010;21(1):92–96. doi: 10.1007/s10165-010-0348-9. [DOI] [PubMed] [Google Scholar]
- 163.Pechal X, DeBandt M, Berthelot JM. Tocilizumab in refractory adult Still’s disease. Arthritis Care & Research. 2011;63(1):155–159. doi: 10.1002/acr.20319. [DOI] [PubMed] [Google Scholar]
- 164.Sabnis GR, Gokhale YA, Kulkarni UP. Tocilizumab in refractory adult-onset Still’s disease with aseptic meningitis-efficacy of interleukin-6 blockade and review of the literature. Seminars in Arthritis & Rheumatism. 2010;40(4):365–368. doi: 10.1016/j.semarthrit.2010.05.003. [DOI] [PubMed] [Google Scholar]
- 165.Rech J, Ronneberger M, Englbrecht M, et al. Successful treatment of adult-onset Still’s disease refractory to TNF and IL-1 blockade by IL-6 receptor blockade. Annals of the Rheumatic Diseases. 2011;70(2):390–392. doi: 10.1136/ard.2010.129403. [DOI] [PubMed] [Google Scholar]
- 166.Ito H, Takazoe M, Fukuda Y, et al. A pilot randomized trial of a human anti-interleukin-6 receptor monoclonal antibody in active Crohn’s disease. Gastroenterology. 2004;126(4):989–996. doi: 10.1053/j.gastro.2004.01.012. [DOI] [PubMed] [Google Scholar]
- 167.Hirano T, Ohguro N, Hohki S, et al. A case of Behcet’s disease treated with a humanized anti-interleukin-6 receptor antibody, tocilizumab. doi: 10.1007/s10165-011-0497-5. Modern Rheumatology. In press. [DOI] [PubMed] [Google Scholar]
- 168.Hagihara K, Kawase I, Tanaka T, Kishimoto T. Tocilizumab ameliorates clinical symptoms in polymyalgia rheumatica. Journal of Rheumatology. 2010;37(5):1075–1076. doi: 10.3899/jrheum.091185. [DOI] [PubMed] [Google Scholar]
- 169.Tanaka T, Hagihara K, Shima Y, et al. Treatment of a patient with remitting seronegative, symmetrical synovitis with pitting oedema with a humanized anti-interleukin-6 receptor antibody, tocilizumab. Rheumatology. 2010;49(4):824–826. doi: 10.1093/rheumatology/kep412. [DOI] [PubMed] [Google Scholar]
- 170.Tanaka T, Kuwahara Y, Shima Y, et al. Successful treatment of reactive arthritis with a humanized anti-interleukin-6 receptor antibody, tocilizumab. Arthritis Care & Research. 2009;61(12):1762–1764. doi: 10.1002/art.24899. [DOI] [PubMed] [Google Scholar]
- 171.Henes JC, Horger M, Guenaydin I, Kanz L, Koetter I. Mixed response to tocilizumab for ankylosing spondylitis. Annals of the Rheumatic Diseases. 2010;69(12):2217–2218. doi: 10.1136/ard.2009.126706. [DOI] [PubMed] [Google Scholar]
- 172.Wendling D, Bossert M, Prati C. Short-term effect of IL-6 inhibition in spondylarthritis. Joint Bone Spine. 2010;77(6):624–625. doi: 10.1016/j.jbspin.2010.09.011. [DOI] [PubMed] [Google Scholar]
- 173.Brulhart L, Nissen MJ, Chevallier P, Gabay C. Tocilizumab in a patient with ankylosing spondylitis and Crohn’s disease refractory to TNF antagonists. Joint Bone Spine. 2010;77(6):625–626. doi: 10.1016/j.jbspin.2010.08.004. [DOI] [PubMed] [Google Scholar]
- 174.Shima Y, Tomita T, Ishii T, et al. Tocilizumab, a humanized anti-interleukin-6 receptor antibody, ameliorated clinical symptoms and MRI findings of a patient with ankylosing spondylitis. Modern Rheumatology. 2011;21(4):436–439. doi: 10.1007/s10165-011-0416-9. [DOI] [PubMed] [Google Scholar]
- 175.Cohen JD, Ferreira R, Jorgensen C. Ankylosing spondylitis refractory to tumor necrosis factor blockade responds to tocilizumab. The Journal of Rheumatology. 2011;38(7):p. 1527. doi: 10.3899/jrheum.110265. [DOI] [PubMed] [Google Scholar]
- 176.Gergis U, Arnason J, Yantiss R, et al. Effectiveness and safety of tocilizumab, an anti-interleukin-6 receptor monoclonal antibody, in a patient with refractory GI graft-versus-host disease. Journal of Clinical Oncology. 2010;28(30):e602–e604. doi: 10.1200/JCO.2010.29.1682. [DOI] [PubMed] [Google Scholar]
- 177.Drobyski WR, Pasquini M, Kovatovic K, et al. Tocilizumab for the treatment of steroid refractory graft versus host disease. Biology of Blood and Marrow Transplantation. 2011;17(12):1862–1868. doi: 10.1016/j.bbmt.2011.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178.Vaitla PM, Radford PM, Tighe PJ, et al. Role of interleukin-6 in a patient with tumor necrosis factor receptor-associated periodic syndrome: assessment of outcomes following treatment with the anti-interleukin-6 receptor monoclonal antibody tocilizumab. Arthritis & Rheumatism. 2011;63(4):1151–1155. doi: 10.1002/art.30215. [DOI] [PubMed] [Google Scholar]
- 179.Taniguchi K, Shimazaki C, Fujimoto Y, et al. Tocilizumab is effective for pulmonary hypertension associated with multicentric Castleman’s disease. International Journal of Hematology. 2009;90(1):99–102. doi: 10.1007/s12185-009-0346-x. [DOI] [PubMed] [Google Scholar]
- 180.Arita Y, Sakata Y, Sudo T, et al. The efficacy of tocilizumab in a patient with pulmonary arterial hypertension associated with Castleman’s disease. Heart and Vessels. 2010;25(5):444–447. doi: 10.1007/s00380-009-1215-5. [DOI] [PubMed] [Google Scholar]
- 181.Furuya Y, Satoh T, Kuwana M. Interelukin-6 as a potential therapeutic target for pulmonary arterial hypertension. International Journal of Rheumatology. 2010;2010:8 pages. doi: 10.1155/2010/720305. Article ID 720305. [DOI] [PMC free article] [PubMed] [Google Scholar]