

Abstract
We are presenting a rare case of bladder leiomyoma. A 61-year-old female patient was found to have a bladder mass during a work up of lower urinary tract symptoms. After full investigation, she underwent transurethral excision of the mass. The histopathology revealed typical feature of bladder leiomyoma. No recurrence was seen after a follow-up period of 12 months.
Keywords: Bladder, cystoscopy, histopatholgy, liemyoma, radiology
INTRODUCTION
Leiomyomas are benign tumors that may be found at any site in the genitourinary tract. Benign mesenchymal tumors make up 1–5% of all bladder neoplasms, with leiomyoma representing the largest subgroup (35%) of these rare benign tumors.[1]
CASE REPORT
A 61-year-old diabetic lady with history of Rheumatoid Arthritis and Sjögren's syndrome was referred to urology clinic for storage symptoms of urgency and dysurea, but no hematuria nor history of weight loss were noticed. There was no family history of malignancy. Her physical examination was unremarkable. Her blood work and urine test were within normal limits. Ultrasound of abdomen and pelvis revealed no hydronephrosis or masses of the upper tract. Although partially filled, the bladder revealed a mass [Figure 1]. Computed Tomography (CT) scan confirmed the presence of the bladder tumor without any evidence of distant metastasis [Figure 2].
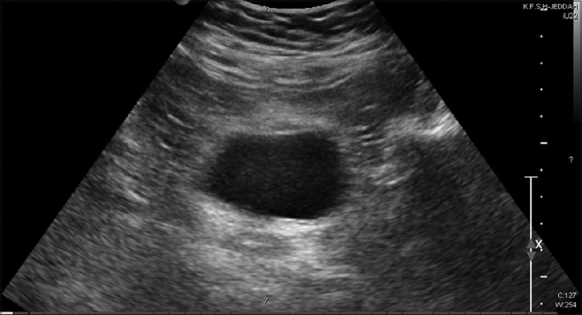
Figure 1.

Pelvic ultrasound showing a well-defined hypoechoic lesion noted at the anterior wall of the urinary bladder measuring 1.4 × 1.2 × 1.2 cm
Figure 2.

Pelvic computed tomography (CT) scans demonstrate bladder wall enhancing soft tissue mass measuring 1.8 × 1.3 × 1.3 cm, which has minimal stranding around it. No invasion to the adjacent structures
The patient underwent cystoscopy, which revealed a protruding mass from the anterior wall of the bladder, but with normal covering urothelium. It was better visualized with help of suprapubic compression. The resecting loop was used to incise the urothelium and complete enucleation of the mass was successful bluntly by using the tip of the loop, using low pressure irrigation and continuous emptying of the bladder to avoid any significant extravasations. The patient had an uneventful post-operative period and a Foley's catheter was left for 3 days. Grossly the mass measured 1.7 × 1.1 × 0.8 cm in greatest dimensions with smooth surface and hard consistency. Microscopic description revealed typical features of Leiomyoma, positive for Desmin and negative HMB45 and CD117 [Figures 3 and 4].
Figure 3.
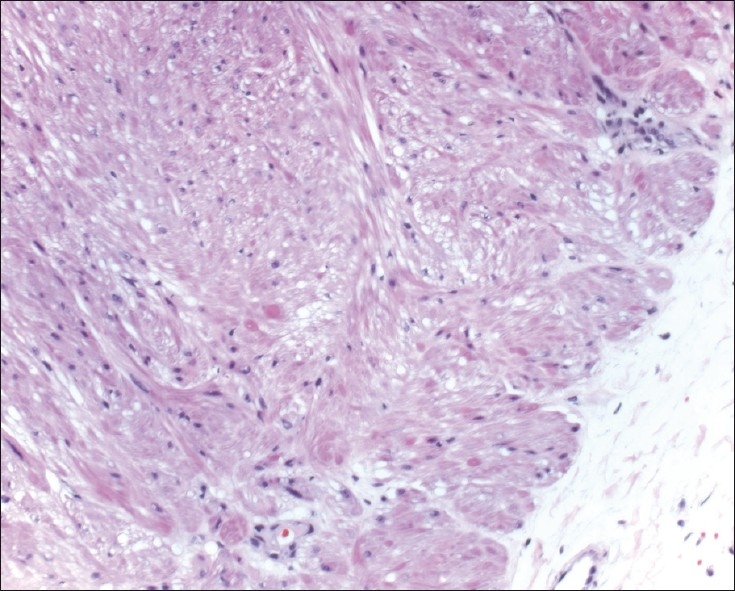
Microscopic examination of the mass showed well demarcated smooth muscle tumor
Figure 4.
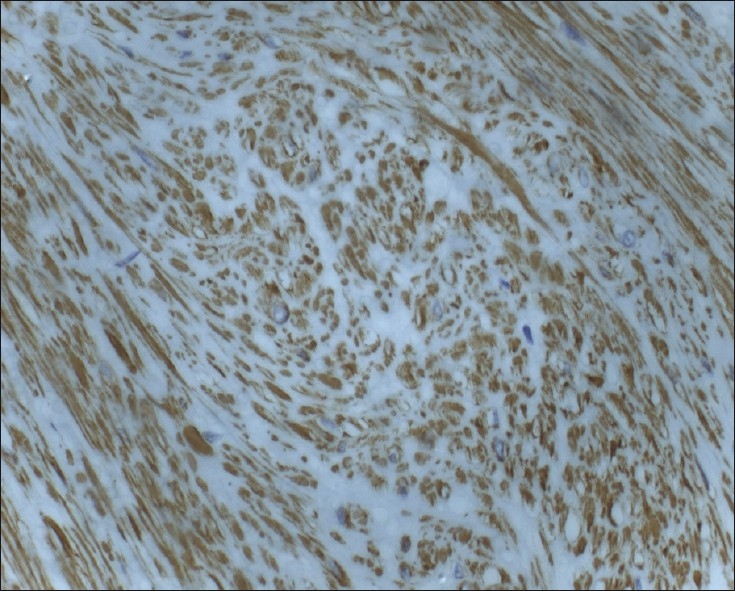
Immunohistochemical examination of the tumor was positive with Desmin immunostaining
During follow-up, the patient was free of recurrence, documented on ultrasound and CT scan done at 3 months and 12 months, respectively [Figures 5 and 6]. She continued to have urgency, which was controlled by Oxybutanin 5 mg twice a day.
Figure 5.
Pelvic ultrasound showing the urinary bladder free of any masses
Figure 6.

Pelvic CT scan reveal the urinary bladder free of any masses
DISCUSSION
Bladder leiomyoma is a rare tumor accounting for 0.43% of total bladder neoplasm.[2] It is the most common benign tumor arising from the submucosa. Its growth can be submucosal (7%), intravesical (63%), or extravesical (30%). Equal incidence in both sexes has been reported.[3]
Leiomyoma may be discovered incidentally in a symptomatic patient (19%) but usually present with obstructive symptoms (49%), irritative symptoms (38%), and hematuria (11%). It has been reported that a palpable lesion is encountered in 57% of women who undergo bimanual examination.[4]
Imaging studies can diagnose bladder leiomyoma preoperatively. They include execratory urography, ultrasound, CT, and magnetic resonance imaging (MRI). Excretory urography or cystourethrography may identify a smooth filling defect in the bladder. Pelvic ultrasound may reveal a submucosal solid mass in the bladder and it can confirm the origin of the tumor in the bladder wall and its relationship to the uterus and vagina.[5] Transvaginal ultrasound may give accurate information about localization of the mass and its relation to adjacent organs.[6] CT has been used to detect leiomyoma of the bladder since the late 1980s.[7] MRI of the bladder can differentiate mesenchymal tumors from the more common transitional cell tumors. However, MRI adds a new dimension to recognition and overall assessment of the tumor and cannot be relied on unfailingly to differentiate leiomyoma from leiomyosarcoma, because both may be enhanced after contrast media administration.[8] Thus, pathological examination of the tumor should confirm the benign nature of the tumor.
Histologically, leiomyomas have spiral smooth muscle fibers with less than two mitotic figures per high-powered field. On the other hand, leiomyosarcoma usually has a large quantity of myxoid intracellular material and invades the muscularis propria with more mitotic activity.[9]
The treatment of leiomyomas is determined primarily by their size and anatomic location.[9] The treatment options for leiomyoma of the bladder include open surgical excision and transurethral resection, with the latter being the treatment of choice for small tumors.[10] However, resection has the potential to be incomplete leaving residual tumor and carries a higher risk for bleeding and injury to adjacent tissue such as the ureter. The use of a ureteral stent should be considered if the dissection is close to the ureter.[11] Some authors suggest the use of transurethral resection for tumor size less than 2 cm.[11]
Some authors reviewed other cases, and found that 62% of the patients had open resection, while 30% underwent transurethral resection.[4] Small endovesical tumors can be resected transuretharly and only 18% have necessitated reoperation due to incomplete resection. Of the 62% who underwent open resection for large endovesical tumors, extravesical tumors or intramural lesions, none required a second procedure.
In conclusion, bladder leiomyoma is a rare benign lesion, which may occur in the urinary tract with an acceptable cure rate using minimally invasive intervention.
Footnotes
Source of Support: Nil,
Conflict of Interest: None.
REFERENCES
- 1.Campbell EW, Gislason GJ. Benign mesothelial tumors of the urinary bladder: Review of literature and a report of a case of leiomyoma. J Urol. 1953;70:733–41. doi: 10.1016/S0022-5347(17)67977-1. [DOI] [PubMed] [Google Scholar]
- 2.Cornella JL, Larson TR, Lee RA, Magrina JF, Kammerer-Doak D. Leiomyoma of female urethra and bladder: Report of twenty-three patients and review of the literature. Am J Obstet Gynecol. 1997;176:1278–85. doi: 10.1016/s0002-9378(97)70346-6. [DOI] [PubMed] [Google Scholar]
- 3.Knoll LD, Segura JW, Scheithauer BW. Leiomyoma of the bladder. J Urol. 1986;136:906–8. doi: 10.1016/s0022-5347(17)45124-x. [DOI] [PubMed] [Google Scholar]
- 4.Goluboff ET, O’Toole K, Sawczuk IS. Leiomyoma of bladder: Report of case and review of literature. Urology. 1994;43:238–41. doi: 10.1016/0090-4295(94)90053-1. [DOI] [PubMed] [Google Scholar]
- 5.Illescas FF, Baker ME, Weinerth JL. Bladder leiomyoma: Advantages of sonography over computed tomography. Urol Radiol. 1986;8:216–8. doi: 10.1007/BF02924110. [DOI] [PubMed] [Google Scholar]
- 6.Fernández Fernández A, Mayayo Dehesa T. Leiomyoma of the urinary bladder floor: Diagnosis by transvaginal ultrasound. Urol Int. 1992;48:99–101. doi: 10.1159/000282305. [DOI] [PubMed] [Google Scholar]
- 7.Brant WE, Williams JL. Computed tomography of bladder leiomyoma. J Comput Assist Tomogr. 1984;8:562–3. doi: 10.1097/00004728-198406000-00041. [DOI] [PubMed] [Google Scholar]
- 8.Sundaram CP, Rawal A, Saltzman B. Characteristics of bladder leiomyoma as noted on magnetic resonance imaging. Urology. 1998;52:1142–3. doi: 10.1016/s0090-4295(98)00333-1. [DOI] [PubMed] [Google Scholar]
- 9.Soloway D, Simon MA, Milikowski C, Soloway MS. Epithelioid leiomyoma of the bladder: An unusual cause of voiding symptoms. Urology. 1998;51:1037–9. doi: 10.1016/s0090-4295(98)00016-8. [DOI] [PubMed] [Google Scholar]
- 10.Vargas AD, Mendez R. Leiomyoma of the bladder. Urology. 1983;21:308–9. doi: 10.1016/0090-4295(83)90095-x. [DOI] [PubMed] [Google Scholar]
- 11.Ninan AC, St Luce S, Kimberl IJ, Petros JA, Issa MM. Endoscopic enucleation of leiomyoma of the bladder. Urol Int. 2005;75:8–9. doi: 10.1159/000085919. [DOI] [PubMed] [Google Scholar]