

Abstract
Objectives:
The objective of this study is to translate and validate the International Restless Leg Syndrome Study Group rating scale (IRLS) in Hindi language.
Materials and Methods:
Thirty one consecutive patients diagnosed of Restless Leg Syndrome (RLS) were included in the study. Control group comprised of 31 subjects not having any symptom of RLS. The scale was procured from MAPI research trust; and, permission for the translation was sought. The translation was done according to the guidelines provided by the publisher. After translation, final version of the scale was applied in both the groups to find out the reliability and clinical validity.
Results:
RLS group had a predominance of females, and they were younger than the male counterparts (Age=36.80 ± 10.46 years vs 45.18 ± 8.34 years; t=2.28; P=0.03). There was no difference in the mean age between groups (RLS=39.77 ± 10.44 years vs Non RLS=38.29 ± 11.29 years; t=-0.53; P=0.59). IRLS scores were significantly different between both groups on all items (P<0.001). Translated version showed high reliability (Cronbach's alpha=0.86). IRLS scores were significantly different between both groups on all items (P<0.001).
Conclusion:
Hindi version of IRLS is reliable and a clinically valid tool that can be applied in Hindi speaking population.
Keywords: Hindi translation, International Restless Leg Syndrome Study Group rating scale, Restless Leg Syndrome, translation, validation
Introduction
Restless leg syndrome (RLS) is primarily a neurological sleep disorder that is characterized by urge to move legs, that is usually associated with unpleasant sensations in the legs that are relieved by walking and increased by rest; with the sensations usually being worse in the evening or night.[1] Most of these patients present with the complaints of insomnia rather than RLS itself. Prevalence of RLS appears to be lower in the Asian countries as compared to their western counterparts; and, RLS has been found to substantially increase the risk of Major Depressive Disorder and Anxiety Disorders.[2] Restless leg syndrome is usually diagnosed according to the criteria proposed by International RLS Research Group.[1] This is primarily a neurobehavioral disorder; hence objectively, severity can only be assessed by using a questionnaire. International Restless Leg Syndrome Study Group rating scale (IRLS) is a valid instrument that has shown high internal consistency, test-retest reliability and clinical validity.[3] This scale is important in clinics to measure the improvement with treatment as well as for the research purpose to measure the severity of RLS.
The prevalence of RLS in India has been reported to be 2.1% in a small community sample.[4] Another study from a teaching hospital suggested that prevalence is 6.25% in non-anemic and 34% in iron deficiency anemia patients.[5] India caters to almost 20% of the world population.[6] This large population suggests the possible magnitude of RLS problem in India. Furthermore, India is majorly a Hindi speaking country with a literacy rate of 74%.[7,8] Since, the original version of the IRLS is in English, it is difficult to be use this in the Indian population. Thus, we planned to translate this scale in Hindi language.
Materials and Methods
Population
The study included thirty one consecutive subjects of RLS who had attended the sleep clinic after obtaining their written informed consent. RLS was diagnosed as per the criteria of International RLS research group.[1] Thirty one patients who were not having any symptom of RLS were included as the control group. Subjects with confounding factors as chronic kidney disease, peripheral neuropathy, those taking antipsychotics or dopamine agonists, opoid substance abusers, subjects suffering from opoid withdrawal, pregnant females, children and those not willing to provide informed consent were excluded from the study. Similarly, RLS mimics were also excluded from the study.[9] Approval from the institutional ethics committee was sought beforehand. Subjects were included irrespective of their gender, educational status and domicile (urban or rural). Each item of the scale was read aloud by the investigators and responses were recorded as mentioned in the instructions booklet provided by MAPI Research Trust.[10]
Original instrument
International Restless Leg Syndrome Research Group Rating Scale is a copyright to the MAPI Research Trust, France. Hence, publisher was approached and written permission for translation was sought. After obtaining the written permission, translation was done as per the instructions provided by the publisher.[10]
Translation procedure
Translation was done from the English version after seeking written permission from the MAPI research trust. Guidelines as provided by MAPI research trust were followed for the translation.[10] Firstly, the scale was translated into Hindi by two independent linguistic experts, and this resulted in development of versions 1 and 2 of the scale. Then both the linguistic experts discussed each item with the subject experts and version 3 was reached. This version 3 was then back-translated into English by two other linguistic experts. This step resulted in the version 4. This version 4 was then compared with the original scale and points of disagreement were discussed with subject experts. Language was again modified and a Hindi version 5 was created. This scale was applied on ten patients to assess the ease of understanding. They were encouraged to report any difficulty that they had faced in understanding any of the items. Wherever the patients reported any difficulty, the issue was discussed with the linguistic experts and appropriate change was made to keep the language closest possible to the original scale. Finally, version 6 was created. This final version was used for the present study. To assess the test-retest reliability, the scale was administered again after two weeks in 18 patients.
Statistical analysis
Analysis was done using Statistical Package for the Social Sciences (SPSS) v 17.0. Descriptive statistics (frequency, mean) was calculated for the categorical variables. To find out the correlation between various questions, Spearman's correlation was used. Same statistical test was used to assess test-retest reliability. Independent sample t test was used to find out the differences in the means of continuous variables. Reliability of the scale was measured by calculating the Croanbach's alpha. Clinical validity of scale was assessed by comparing the scores with the control group.
Results
This study included a total of thirty one subjects, out of which eleven (35.48%) were males. Females included in this study were younger than males (Age = 36.80 ± 10.46 years vs 45.18 ± 8.34 years; t = 2.28, P=0.03). However, the responses on different items of the scale did not differ between genders [Figure 1].
Figure 1.
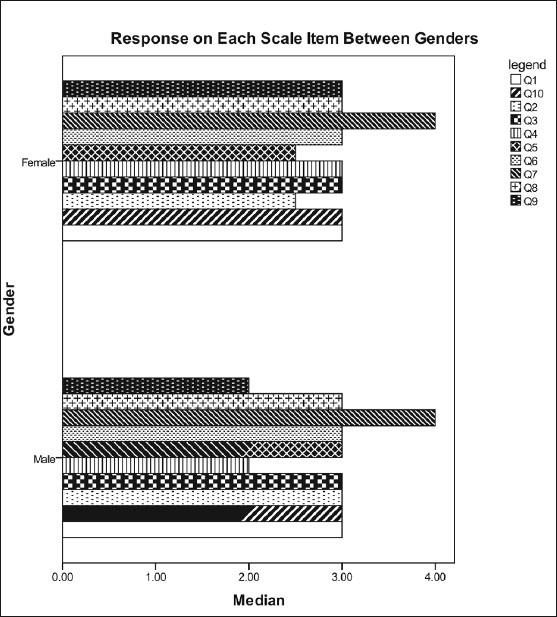
Responses on different items of the Hindi translated version of International Restless Leg Syndrome Study Group rating Scale showing that the responses did not differ between the genders
Thirty one subjects were included in the control group. This group had a predominance of males (54.83%).
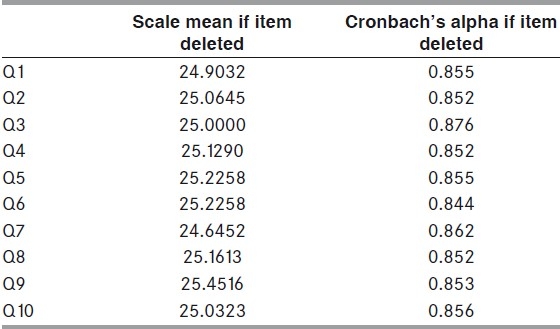
Gender distribution was not different between both the groups (X2 = 2.34; P=0.10). There was no difference in the mean age between groups (RLS = 39.77 ± 10.44 years vs Non RLS = 38.29 ± 11.29 years; t = –0.53; P=0.59). IRLS scores were significantly different between both groups on all items (P<0.001). Correlation matrix showed that most of the items were well correlated with each other [Table 1]. Reliability analysis showed that the whole scale had Cronbach's alpha of 0.86. This figure did not change even after removal of any item of the scale [Table 2]. However, there was a moderate correlation on test-retest reliability (r2 = 0.43).
Table 1.
Correlation matrix between different items of the Hindi translated version of International Restless Leg Syndrome Study Group rating scale
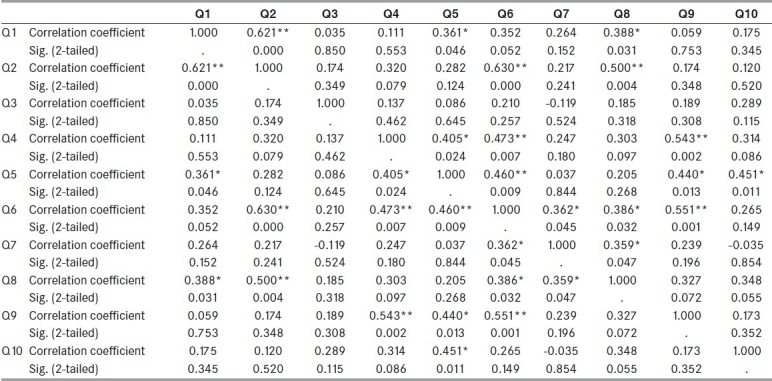
Table 2.
Reliability analysis of the Hindi translated version of International Restless Leg Syndrome Study Group rating scale
Translation of scale
There were many problems encountered during the translation as well as the cultural adaptation of the scale. The scale was translated literally to the best possible level; howver, many of the words were changed to depict the contextual meaning for cultural adaptation. For this, words were chosen from the local dialect.
We do not have any literal word in Hindi for ‘discomfort’. Hence, this was replaced by “pareshani” (disturbance) in item numbers 1 and 3. In item number 2, many patients complained that they did not ‘move around′; however, kept on moving their legs while in bed. Similarly, literal meaning of ‘move around’ was felt difficult to understand by experts. Hence, it was phrased as ‘idhar-udhar ghoomne ya paanv hilane kee zaroorat’ (need to walk here and there or to move legs)” to bring it closest to the original version. Similar changes were made in item number 3. In item number 5, ‘during the day’ was difficult to understand and was losing its contextual meaning. To make the question clearer, it was framed as ‘…agle din kitni neend ya thakaan mahssos huyi’ (…how much sleepiness or tiredness was felt next day). Similarly, Hindi language does not have any literal word for ‘severity’. Contextually, it denotes the extent of problem in quantitative terms. Hence, this word in question as well as in responses was modified accordingly, and ‘very severe’ was changed to ‘bahut jyada’ (very much); ‘severe’ to ‘jyada’ (much); moderate to ‘Thodi Bahut/madhyam (to some extent/moderate) and ‘mild’ to ‘karib-karib nahi’ (almost none) in item numbers 1, 2, 4, 5, 8, 9 and 10.
In item number 6, the response ‘moderate’ was changed to ‘ausat’ (average) and mild to ‘bahut kam’ (little) to keep them in context with the question.
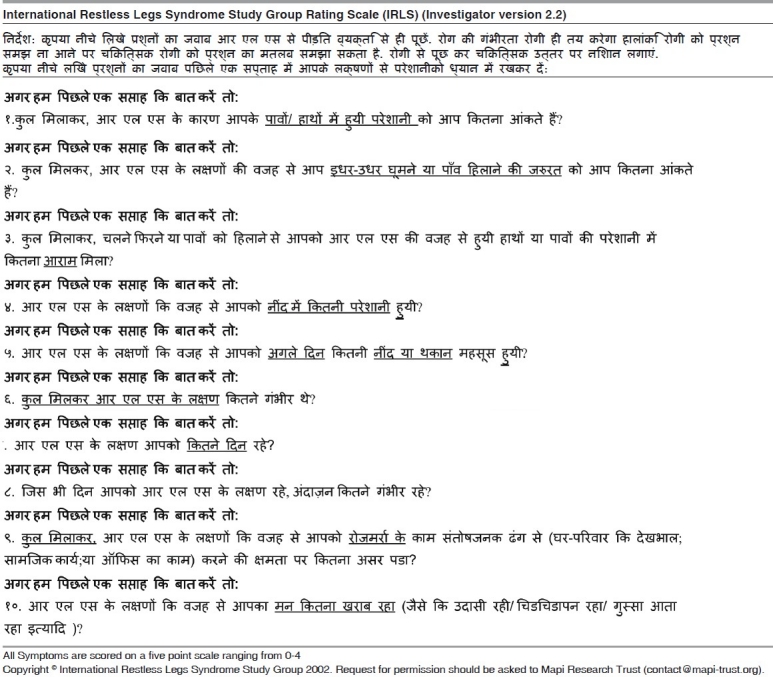
In local dialect, ‘often’ is used with reference to the frequency. Keeping with the spirit of item in the original scale, the ‘often’ was changed to ‘kitne din’ (how many days). Similarly, responses were changed to ‘bahut jyada’ (very much); ‘jyada’ (much); ‘kabhi-kabhi’ (sometimes) and ‘shaayad kabhi’ (probably sometime). Numbers of days were mentioned in the parenthesis as mentioned in the original document. Table 3 shows the Hindi version of scale.
Table 3.
Hindi translated version of International Restless Leg Syndrome Study Group rating scale©
Discussion
This study showed that Hindi version of IRLS has good internal consistency, is clinically valid, and can be used with ease in the Hindi speaking population of India. This scale is also available in English, and has been translated in Brazilian Portuguese.[3,11] Original version has shown good reliability of 0.95.[3] It has been found to have good internal consistency and reliability (alpha = 0.76) in clinical trial.[12] Brazilian Portuguese translation has shown a good reliability with the Cronbach's alpha score of 0.83.[11] Our study shows that Hindi version is also having a good reliability (Cronbach's alpha score of 0.86). Also, the scale is clinically valid and has a high discriminative ability.[3] Brazilian translation has not been tested on the control group.[11] Our results have shown that when the standard procedure is followed to administer the scale, the scores differ significantly between RLS and non-RLS subjects.[10] Non-RLS subjects score zero on all items because of the inclusion of the phrase “because of the RLS…” in all questions. However, when the scale is given to sleep disorder patients not having RLS, they marked some of the responses positively. This happened even when we explained the symptoms of RLS to all participants before asking them to fill the scale themselves.
During the translation procedure, we have changed some of the words according to the needs and understanding of the patients. Cha et al.,[13] have suggested that decentring should be applied instead of direct translation of the scale for a cross - cultural population. These translations face few common problems like vocabulary equivalence, idiomatic equivalence, grammatical - syntactical equivalence, experiential equivalence and lastly conceptual equivalence.[13] We have faced the problems related to vocabulary equivalence and conceptual equivalence. Cha et al.[13] recommend that vocabulary problems can be solved by finding closely similar words of the target language. Similarly, for better understanding, syntax of the language can be modified by deleting or adding words or phrases according to the need of the target language. Conceptual equivalence was dealt with testing the scale on ten patients (version 5) and changing the items according to local needs. Masuko et al.,[11] had also followed the same approach while translating the scale in Brazilian - Portuguese language.
We have used the scale to sequentially assess the improvement in symptoms, and the scores were consistent with the clinical symptoms (data will be published separately). However, there was a poor correlation between test and retest scores. This type of reliability testing might sometimes give spurious results.[14] There are many reasons for this problem - first, the scale measures problem in past week only; secondly, scores are affected by clinical improvement as it is a severity rating scale, rather than a diagnostic tool; thirdly, symptoms of RLS vary on day-to-day basis; and, lastly, RLS usually responds dramatically to the therapy. Translating a linguistic instrument is difficult for those places where a segment of population is illiterate. We have shown that the instrument was applicable in all strata of patients- illiterate, literate, rural as well as urban. Minor grammatical errors may be ignored for the better acceptability of the instrument.[11] Hindi version was applicable in all subjects without any additional information being given to them at the time of administration of scale.
The strength of this study is the exclusion of subjects with conditions that may mimic RLS.[9] Hence, the data reflects the applicability of scale in true RLS cases. In conclusion, we were able to translate the IRLS in Hindi successfully and the translated version has shown good reliability and clinical validity, when the instructions were followed.
Footnotes
Source of Support: Nil,
Conflict of Interest: Nil.
References
- 1.Allen RP, Picchietti D, Hening WA, Trenkwalder C, Walters AS, Montplaisi J, et al. Restless legs syndrome: Diagnostic criteria, special considerations, and epidemiology. A report from the restless legs syndrome diagnosis and epidemiology workshop at the National Institute of Health. Sleep Med. 2003;4:101–19. doi: 10.1016/s1389-9457(03)00010-8. [DOI] [PubMed] [Google Scholar]
- 2.Cho SJ, Hong JP, Hahm BJ, Jeon HJ, Chang SM, Cho MJ, et al. Restless legs syndrome in a community sample of Korean adults: Prevalence, impact on quality of life, and association with DSM-IV psychiatric disorders. Sleep. 2009;32:1069–76. [PMC free article] [PubMed] [Google Scholar]
- 3.Walters AS, LeBrocq C, Dhar A, Hening W, Rosen R, Allen RP, et al. Validation of the International Restless Legs Syndrome Study Group rating scale for restless legs syndrome. Sleep Med. 2003;4:121–32. doi: 10.1016/s1389-9457(02)00258-7. [DOI] [PubMed] [Google Scholar]
- 4.Rangarajan S, Rangarajan S, D’Souza GA. Restless legs syndrome in an Indian urban population. Sleep Med. 2007;9:88–93. doi: 10.1016/j.sleep.2006.11.004. [DOI] [PubMed] [Google Scholar]
- 5.Rangarajan S, D’Souza GA. Restless legs syndrome in Indian patients having iron deficiency anemia in a tertiary care hospital. Sleep Med. 2007;8:247–51. doi: 10.1016/j.sleep.2006.10.004. [DOI] [PubMed] [Google Scholar]
- 6.New Delhi (India): Office of Registrar General and Census Commissioner; 2011. [cited on 2011 May 19]. Provisional population totals- census 2011 [Internet] c2010-11 Available from: http://censusindia.gov.in/2011-prov-results/indiaatglance.htm . [Google Scholar]
- 7.New Delhi (India): Office of Registrar General and Census Commissioner India; [cited on 2011 May 19]. Provisional population tables and annexure [Internet] c2010-11 Available from http://www.censusindia.gov.in/2011-prov-results/data_files/india/Final%20PPT%202011_progresstables.pdf . [Google Scholar]
- 8.Washington D.C.: Central Intelligence Agency; [cited on 2011 May 19]. The World Factbook. Available from: https://www.cia.gov/library/publications/the-world-factbook/geos/in.html . [Google Scholar]
- 9.Hening WA, Allen RP, Washburn M, Leasge SR, Early CJ. The four diagnostic criteria for restless leg syndrome are unable to exclude confounding conditions (“mimics”) Sleep Med. 2009;10:976–81. doi: 10.1016/j.sleep.2008.09.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.MAPI Research Trust. France: IRLS contact information and permission to use; c2004-11. [cited on 2011 Mar 13]. Available from: http://www.mapitrust.org/
- 11.Masuko AH, Carvalho LB, Machado MA, Morais JF, Prado LB, Prado GF. Translation and validation into the Brazilian Portuguese of the restless legs syndrome rating scale of the International Restless Legs Syndrome Study Group. Arq Neuropsiquiatr. 2008;66:832–6. doi: 10.1590/s0004-282x2008000600011. [DOI] [PubMed] [Google Scholar]
- 12.Abetz L, Arbuckle R, Allen RP, Garcia-Borreguero D, Hening W, Walters AS, et al. The reliability, validity and responsiveness of the International Restless Legs Syndrome Study Group rating scale and subscales in a clinical-trial setting. Sleep Med. 2006;7:340–9. doi: 10.1016/j.sleep.2005.12.011. [DOI] [PubMed] [Google Scholar]
- 13.Cha ES, Kim KH, Erlen JA. Translation of scales in cross-cultural research: Issues and techniques. J Advanced Nursing. 2007;58:386–95. doi: 10.1111/j.1365-2648.2007.04242.x. [DOI] [PubMed] [Google Scholar]
- 14.Viswanathan M. California: Sage Publications; 2005. Measurement error and research design. [Google Scholar]