

Abstract
Background and Objectives:
Obesity and overweight are major determinants of health and quality of life. The World Health Organization (WHO) has always encouraged its member states to carry out studies on the attributable burden of these diseases at the national level, and use the study as the best guide to direct the health system policy. This study was thus undertaken in order to determine the regional burden of non-communicable diseases due to obesity and overweight.
Setting and Design:
Counterfactual analysis of the death registration data in Markazi province of Iran was carried out.
Materials and Methods:
We calculated the Years of Life Lost (YLL) according to the WHO's comparative risk assessment approach. Moreover, the attributable burden of obesity and overweight was determined by multiplying the impact fraction of risk factors with the YLL of major diseases, and the counterfactual analysis method was used.
Results:
A total of 7,176 deaths were registered contributing to 252,214 YLL, due to premature mortality. The total YLL due to premature mortality among females and males were 102,245 and 149,969 years, respectively. The most important causes of the YLL were associated with obesity and overweight in cardiovascular diseases for females, and overweight in cardiovascular diseases for males (12,826, 8,755 and 7,375 years, respectively).
Conclusion:
In this study, the importance and necessity of the recognition of overweight and obesity as the major risk factors for non-communicable diseases was shown. Hence, it is necessary to develop and apply comprehensive interventions to reduce the effect of overweight and obesity, especially in females.
Keywords: Attributable risk, burden of diseases, non-communicable diseases, obesity, overweight
INTRODUCTION
In many countries of the Middle East region, the incidence of Non-Communicable Diseases (NCDs) is ever increasing as a result of prolonged life spans, increasingly longer exposures to risk factors and changing patterns of life styles.[1] NCDs mortalities were, in fact, three times greater than those due to infectious diseases in this region about two decades ago.[2] Obesity and overweight are two of the most important determinants of health and the quality of life in the global burden of disease (GBD) epidemics.[3,4] These are the third most likely (7.2%) risk factors associated with NCDs and injuries leading to the loss of healthy life among rich nations.[5] For instance, cardiovascular diseases (CVDs) are the leading cause of death among NCDs, and their annual mortality rate among the population over 40-years old is estimated as 1.4% in Iran.[6] The traditional metrics’ system had numerous shortcomings in determining the health status of the community and could not properly supply to the needs of a community study.[7] Therefore, in the second half of the 20th century, it was deemed as necessary to adopt a correct decision making system and strengthen the heakth policies. This would even enable obtaining precise data on mortalities, injuries, diseases, incidence rates, and their outcomes, causes and trends. Therefore, a set of metrics was required with which damages due to premature mortality and morbidity from different diseases could be expressed in the context of a common metric, such that, both the health status of individuals and the community distribution of the disease conditions could be manifested in a limited number of quantitative metrics.[7,8] The application of new summary metrics such as life expectancy, disability-free life expectancy, and Disability Adjusted life Years (DALY) would also be effective in such a system.[9] In order to the help managers and policy-makers of the community, these metrics should be able to express – in terms of priority and funding – the burden of mortality and morbidity from diseases and injuries in a conceivable way, so that appropriate actions could b taken accordingly.[8]
DALY expands the concept of Years of Life Lost (YLL) due to premature mortality to the years of life lost due to morbidity due to health problems. DALY is the sum of the YLL due to premature mortality and Years of Life lived with Disability (YLD), due to nonfatal outcomes of diseases and injuries in the community.[10] WHO encourages member states to estimate the burden of diseases at the national level as the best guide to the correct policy-making of health systems.[11] The main aim of this study was to determine the regional burden of NCDs attributable to obesity and overweight in Markazi province, Iran.
MATERIALS AND METHODS
Study area
This study was carried out in Markazi province, Iran during 2006-2007. The surface area of this province is 29,530 km2 which represents only 1.82% of the whole country. It is an industrialized region located 293 km southwest of Tehran, the capital. In the latest census which was carried out in 2006, a sum of 1,351,257 people lived in this province with 682,367 males (50.49%) and 668,890 females (49.51%).[12] The average life expectancy in this province was 72.6 years for females and 68.86 years for males based on the death registration system data in 2004.[13]
Data collection
The mortality data provided in this study was collected by referring to the death registration system run by the Provincial Health Authority (PHA). All sources of diagnosis, detection, recording and collection of data including hospitals, forensic medicine centers, cemetery, and provincial or local health authorities were used to complete the data. In this system, intersectional cooperation ensured that all mortality data were gathered in each district and were dispatched to the PHA. A standard questionnaire, which included questions pertaining to the cause of the death of the individual – as per the findings of the death certificate, or if no certificate was present, as per findings of oral autopsy – was completed by a relative under the supervision of a health investigator. The questionnaire was then encoded according to the International Classification of Diseases (ICD10) guidelines at the PHA, was and was registered in the computer.Calculation of the attributable burden was performed in three consecutive stages. First, the YLL was computed[14] according to the Comparative Risk Assessment (CRA) method of the World Health Organization. This involved a standardized life table in which life expectancy at birth was considered to be 82.5 years for females, and 80 years for males. In the second stage, the generalized impact factor (GIF) was calculated based on the percentage of the risk factors in the following formula.[15–17] For all diseases, the minimum counterfactual risk scenario was taken to be zero.[17]
GIF formula:

In the above formula, RR is the estimate of the relative risk and P reflects the prevalence of the exposure in the population. Finally, after calculating the YLL and GIF based on the counterfactual analysis with the CRA approach, these parameters were multiplied to obtain the attributable burden of obesity and overweight of some NCDs including CVDs such as hypertension, stroke, diabetes (Type 1 and 2), and some cancers (stomach, lung, liver, leukemia, esophageal, colon, breast, and Renal). Obesity is defined as the Body Mass Index (BMI) equal to 30 kg/m2 or more. Besides, overweight is considered as the BMI between 25 and 30 kg/m2.[18] All calculations were conducted in the Statistical package for Social Sciences (SPSS) statistical software (version 11.5) and the Microsoft Office Excel 2007.
RESULTS
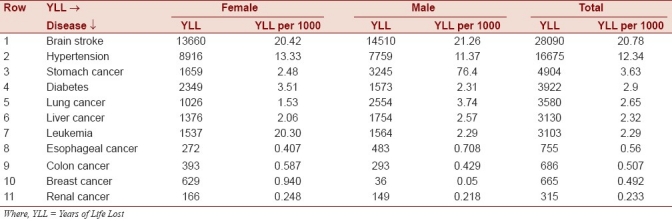
A total of 7,176 deaths were registered in Markazi province in 2006. This caused 252,214 YLL among all the people of this region. 39.6% percent (2,837 deaths) of these deaths were seen in females. The total YLL for premature deaths in females and males were 102,245 (40.5%) and 149,969 (59.5%) years, respectively. Thus, the ratio of male YLL to female YLL was around 1.47. The ten major causes of YLL due to premature deaths in this province in the order of importance were: CVDs (40.89%); injuries and accidents (17.61%); cancers (10.46%); respiratory system diseases (6.48%); geriatric conditions (4.09%); congenital defects and peri-natal diseases (3.46%); genitourinary diseases (2.46%); endocrine and metabolic diseases (2.05%); nervous system disorders (1.86%); and, gastrointestinal diseases (1.59%). Altogether, these accounted for 90.98% of the total YLL due to premature death in this province. These causes of the YLL were sorted with respect to their priority on the 17 causes of disease categorization in GBD [Table 1]. The YLL and YLL per thousand values in males and females for twelve under-study diseases, which were ranked based on their importance in the YLL, were tabulated separately [Table 2]. According to these results, brain stroke got the highest rank, while renal cancer was on the bottom.
Table 1.
Estimated years of life lost of non-communicable disease in Markazi province of I.R. Iran
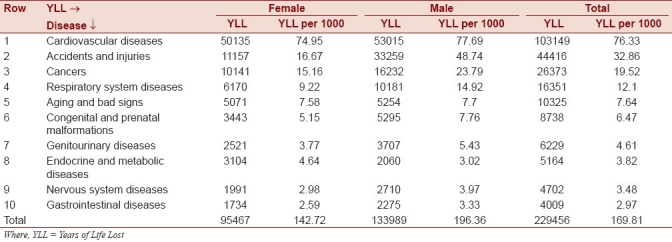
Table 2.
Years of life lost due to premature death for diseases under the study
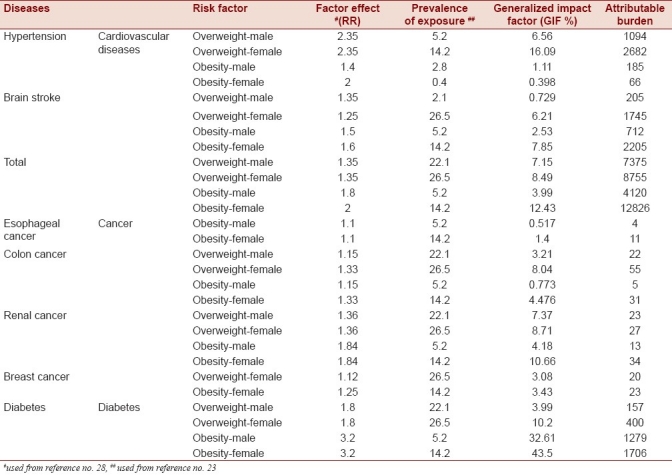
The attributable burden of overweight and obesity in diseases under the study is shown in Table 3. According to these findings, the three main factors involved in YLL due to premature death were obesity and overweight in coronary artery disease among females (12,826 and 8,755), and overweight in coronary artery disease among males (7,375). These results indicated that the attributable burden of obesity and overweight in cancers was less than that in CVD, hypertension, stroke, and diabetes. The minimum attributable burden was related to obesity, and esophageal and colon cancers in males.
Table 3.
Attributable burden of overweight and obesity for diseases under the study
DISCUSSION
This study showed that nearly 91% of the total burden of diseases was related to ten main causes. and that the highest burden of the YLL due to premature death was related to coronary heart diseases, cancer, and accidents. Mousavi et al.[11] conducted a study in Zanjan province, in the northwest of Iran, and obtained similar results. In their study, cardiovascular diseases, unintentional injuries, and malignancies were listed as three major causes of the premature death. Our study showed that the YLL in males is approximately 1.5 times higher than that of females, but this ratio was calculated as 1.8 in Mousavi's study. In a study on global and regional burden of diseases in 2001, heart diseases were ranked as the third leading causes of GBD. Moreover, prenatal birth conditions and lower respiratory system infections held the first and second positions, respectively.[5] Also, in the study performed by Ezzati et al., hypertension had the third rank among the causes of the GBD that contributed to 4.4% of the total burden of diseases.[19]
In the study by Lopez et al. on the measurement of GBD and epidemiological transition of diseases, heart diseases and stroke held the sixth and seventh positions, respectively. Based on a forecast of 2030, heart diseases will become the first cause.[20] However, the NCDs were ranked as the 15th in 1990.[1] Therefore, according to the results of the current study, it seems that the severity and the extent of CVD in reducing the useful years of life is faster in Markazi Province than the global forecast. Our results showed that the major factors of the YLL among males and females are overweight attributed to CVD and obesity attributed to CVD, respectively. Also, regarding the role of overweight, there is not much difference between males and females; however, the role of obesity among females is highlighted. These results might be due to the high prevalence of obesity and overweight in females compared to males in Markazi province[21] or other places.[22]
In the population attributable risk study about the effect of the body mass index (BMI) higher than 25 on the cancer mortality among 30 European countries in 2002, this risk was estimated to be 2.5% for males and 4.1% for females. According to the estimations made in 2008, the population attributable risk for cancer mortality from this risk factor was also calculated to be 3.2% and 8.6% for males and females, respectively.[23] This is consistent with our results; in a way that the role of overweight and obesity among females was higher in increasing the attributable burden. The overall burden of breast cancer due to the early death in Yazd province[24] was obtained as 461 years. This was based on the study population – equal to 0.97 YLL per 1000 people. However, in our study, these measures were equal to 665 years and 0.492, respectively. It indicated that among Yazd population, the YLL due to the breast cancer was twice as much as our community. However in a study in the Eastern Mediterranean,[25] this risk was calculated as 0.488 which was similar to our results. Therefore, it is noteworthy that the YLL in the population under our study is more than the amount calculated for the whole country in 2003. Abolhassani et al.[8] calculated this ratio as 0.25. However, these differences between the two studies, on Markazi and Yazd provinces, may be the results of different methods employed in order to obtain the YLL. Vakili did not state how he calculated the YLL in his study. Also, as mentioned, this difference can be justified since the age standardized incidence ratio in Yazd province is higher than the whole country.
Our study had limitations. First, due to the availability and the need for more valid data on YLL, we decided to use only premature death data, and thus we could not contribute to YLD in the burden of diseases. Also, in calculating the GIF, the hypothetical scenario was set as zero which can lead to the overestimation of the attributable burden.
CONCLUSION
Based on the results of recent studies,[8,13] the attributable burden of overweight and obesity related to CVD is more prominent than other diseases. Moreover, the calculated burden in Markazi province is higher than other provinces. Females are at greater risk from obesity. Therefore, the prevention and the control of obesity – as a major health risk factor, particularly among females – is essential.[26] These findings support the need for development and implementation of comprehensive interventions to reduce the effect of overweight and obesity.
ACKNOWLEDGMENTS
The authors are grateful to all the health workers and the forensic medicine staff, who helped in gathering the data for the Markazi province. We are indebted to the vice-chancellor for permitting us to use the research and technology facilities at Shiraz University of Medical Sciences for our study. Also, we are deeply grateful to the Research Improvement Center and Ms. A. Keivanshekouh for preparing the English edition of this manuscript.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Talebizadeh N, Haghdoost A, Mirzazadeh A. Age at natural menopause, An epidemiological model (Markov Chain) of cardiovascular disease in Iran. Payesh, J Iran Inst Health Sci Res. 2009;2:163–70. [Google Scholar]
- 2.Murray CJ, Lopez AD. Evidence-based health policy lessons from the Global Burden of Disease Study. Science. 1996;274:740–3. doi: 10.1126/science.274.5288.740. [DOI] [PubMed] [Google Scholar]
- 3.Barlocher A, Vetter W, Suter PM. Prevalence of overweight and obesity in Swiss adolescents. Praxis (Bern 1994) 2008;97:119–28. doi: 10.1024/1661-8157.97.3.119. [DOI] [PubMed] [Google Scholar]
- 4.Bener A. Prevalence of obesity, overweight, and underweight in Qatari adolescents. Food Nutr Bull. 2006;27:39–45. doi: 10.1177/156482650602700106. [DOI] [PubMed] [Google Scholar]
- 5.Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet. 2006;367:1747–57. doi: 10.1016/S0140-6736(06)68770-9. [DOI] [PubMed] [Google Scholar]
- 6.Naghavi M. Tehran: Ministry of health, treatment and medical education publication; 1384. Mortality view in 23 providences of Iran. 1382. [Google Scholar]
- 7.Murray CJL, Acharya AK. Understanding DALYs. J Health Econ. 1997;16:703–30. doi: 10.1016/s0167-6296(97)00004-0. [DOI] [PubMed] [Google Scholar]
- 8.Abolhassani F, Khayamzadeh M, Moradi Lake M, Jamali A, Salmanian R, Naghavi M. Estimation of breast cancer burden in Iran in 2003 and its comparison with Eastern Mediterranean region and the World in 2002. Payesh, J Iran Inst Health Sci Res. 2007;3:233–41. [Google Scholar]
- 9.Ministry of health, treatment and medical education. Health vicechancellor. National burden of diseases and injuries in I.R Iran. 1386 [Google Scholar]
- 10.Ayatollahi SM, Hassanzadeh J, Ramezani AA. The burden of traffic accidents in South Khorasan Province, Iran in 2005. Iran J Epidemiol. 2009;3-4:51–7. [Google Scholar]
- 11.Mousavi Nasab N, Shoghli AR, Alizadeh M. Estimating burden of early mortality among people living in Zanjan, 2003. J Zanjan Univ Med Sci Health Serv. 2004;47:41–9. [Google Scholar]
- 12.Statistical Center of Iran. General Population and Housing Census. 1385. [Last accessed on 2011 Oct 25]. Available from: http://www.amar.org.ir/Upload/Modules/Contents/asset23/ostani/markazi1.pdf .
- 13.Khosravi A, Taylor R, Naghavi M, Lopez AD. Differential mortality in Iran. Popul Health Metr. 2007;5:7. doi: 10.1186/1478-7954-5-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.2nd ed 2001. Oct, World health organization Global program on Evidence for health policy: National burden of diseases: A practical Guide. [Google Scholar]
- 15.Ezzati M, Lopez AD, Rodgers A, Murray CJ. Geneva: WHO; 2004. Comparative quantification of health risks, global and regional burden of disease attributable to selected major risk factors. [Google Scholar]
- 16.Lopez AD, Murray CD, Ezzati M, Jamison DT, Murray CJ. Washington: 2006. Global burden of disease and risk factors. Ch 4. [PubMed] [Google Scholar]
- 17.Murray CJ, Lopez AD. On the comparable quantification of health risks: Lessons from the Global Burden of Disease Study. Epidemiology. 1999;10:594–605. [PubMed] [Google Scholar]
- 18.Seidell JC, Flegal KM. Assessing obesity: Classification and epidemiology. Br Med Bull. 1997;53:238. doi: 10.1093/oxfordjournals.bmb.a011611. [DOI] [PubMed] [Google Scholar]
- 19.Ezzati M, Lopez AD, Rodgers A, Vander hoorn S, Murray CJ. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360:1347–60. doi: 10.1016/S0140-6736(02)11403-6. [DOI] [PubMed] [Google Scholar]
- 20.Lopez AD, Mathers CD. Measuring the global burden of disease and epidemiological transitions: 2002-2030. Ann trop med parasitol. 2006;100:481–99. doi: 10.1179/136485906X97417. [DOI] [PubMed] [Google Scholar]
- 21.Mohammad Beigi A, Mohammad Salehi N, Hajian M, Eshrati B, Mansouri A. Sannandaj-Iran: 5th Iranian congress of epidemiology; 2008. Oct 7-9, Prevalence of obesity in Markazi province 1386. 5th Iranian congress of epidemiology; p. 178. [Google Scholar]
- 22.Kazem M, Norbala AA. Study of health and diseases in Iran. Ministry of health, treatment and medical education, research vice-chancellor and national center of medical sciences research. 1380 [Google Scholar]
- 23.Renehan AG, Soerjomataram I, Tyson M, Egger M, Zwahlen M, Coebergh JW, et al. Incident cancer burden attributable to excess body mass index in 30 European countries. Int J Cancer. 2010;126:692–702. doi: 10.1002/ijc.24803. [DOI] [PubMed] [Google Scholar]
- 24.Vakili N, Jafarizadeh M, Sadeghian MR, Mirrezaie M, Norishadkam M, Lotfi MH, et al. Burden of breast cancer in females of Yazd province, 2006. Feyz, Kashan Univ Med Sci Health Serv. 2009;1:31–6. [Google Scholar]
- 25.Bove K, Lincoln DW, Wood PA, Hrushesky WJ. Fertility cycle influence on surgical breast cancer cure. Breast Cancer Res Treat. 2002;75:65–72. doi: 10.1023/a:1016543222323. [DOI] [PubMed] [Google Scholar]
- 26.Ezzati M, Lopez AD, Rodgers A, Murray CJ. Geneva: WHO; 2004. Comparative quantification of health Risks. Chapter 8. [DOI] [PMC free article] [PubMed] [Google Scholar]