

Abstract
Rosai Dorfman Disease is a rare disease presenting mainly as painless enlargement of cervical lymph nodes. It is a benign disorder showing unique histological features characterized by reactive proliferation of sinus histiocytes. In 40% of cases, extranodal sites may be involved. The condition has to be differentiated from certain types of B cell lymphoma showing similar features. We report here a 17 year old male presenting with nodal and extranodal involvement of Rosai Dorfman Disease.
Keywords: Rosai dorfman disease, Emperipolesis, S – 100 protein
Introduction
Rosai Dorfman Disease is a rare disease presenting mainly as painless enlargement of cervical lymph nodes. It is a benign disorder characterized by reactionary proliferation of sinus histiocytes. The proliferating sinus histiocytes show engulfment of lymphocytes, a phenomenon known as emperipolesis. The sinus histiocytes stain positive for S – 100 protein. In 40% of cases, extranodal sites may be involved. The condition has to be differentiated from certain types of B cell lymphoma showing emperipolesis. We report here a 17 year old male with Rosai Dorfman Disease with involvement of central nervous system, parotid glands, cervical, mediastinal, and para-aortic lymph nodes and left orbit.
Case History
A 17 year old male presented with swelling on the left side of the neck of 4 months duration which gradually progressed in size. There were no constitutional symptoms or symptoms suggestive of malignancy in the aerodigestive tract. There was a history of craniotomy, orbitotomy and subtotal decompression of a space occupying lesion in the left middle cranial fossa about 18 months ago. He was on corticosteroids for 4 months and then lost to follow up. He has protrusion of left eyeball since then. There were no similar swellings elsewhere else in the body.
On examination, he was moderately built and nourished, with proptosis of the left eyeball. There was no neurological deficit. The left cervical nodal mass was of the size of 14 × 12 × 6 cms involving levels 2, 3, 4 and 5. The mass was firm and mobile. No other lymph nodes were palpable. The Liver and spleen were not palpable and external genitalia were normal. ENT examination yielded no pathology. FNAC showed chronic nonspecific inflammation. A clinical diagnosis of Non Hodgkin’s Lymphoma was made. Review of previous records yielded a diagnosis of Rosai Dorfman Disease in the cranial cavity and the left orbit. CT scan of the neck, thorax, abdomen and pelvis showed enlarged cervical nodes, bilateral parotid involvement, enlargement of parapharyngeal, retropharyngeal, mediastinal, peripancreatic, and para-aortic nodes. First and second incision biopsy of the cervical nodal mass was inconclusive. The third biopsy gave a diagnosis of Rosai Dorfman Disease. Immuno histochemical analysis of the histiocytes showed positivity for S-100 protein.
The patient underwent debulking of the left cervical lymph nodal mass. The post operative period was uneventful and he was subsequently discharged. On follow up he has not had a recurrence till date.
Discussion
Rosai Dorfman Disease is a disease affecting mainly the lymph nodes of the neck. It is characterized by huge and painless cervical lymphadenopathy. It was first described by Rosai and Dorfman in 1969. It is also known as Sinus Histiocytosis with massive lymphadenopathy (SHML). The disease is rare and probably 1000 cases have been reported in literature.
The disease usually occurs in the second to third decade of life. Apart from cervical nodes; it can sometimes involve lymph node areas in other parts of the body. Extranodal involvement forms 40% of the cases [1]. The etiology is unknown; it is thought be a reactionary phenomenon to as yet unidentified viral agents. Cutaneous involvement forms the most common extranodal site, but purely extranodal presentation is rare [2]. Kong Y Y et al. presented 25 cases of cutaneous Rosai Dorfman Disease with 39 skin lesions [3].Other areas of involvement would include the upper respiratory tract, bone, central nervous system [4], orbits, maxillary alveolus [5], bone marrow, rarely the kidneys [6] and the salivary glands. Around 90 cases have been reported involving the central nervous system, mainly the meninges.
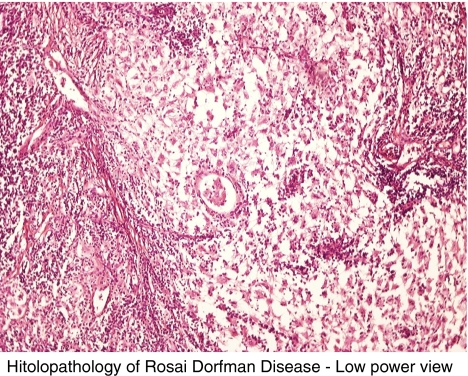
The histopathological picture is characterized by sinuses in the lymph nodes consisting of giant histiocytes which have engulfed lymphocytes, a phenomenon known as emperipolesis. On immunochemical analysis, the histiocytes stain positive for S-100 protein [7]. The presence of S-100 protein differentiates it from certain types of Non - Hodgkin’s Lymphoma which can show emperipolesis [8].
The disease follows a benign course with painless and massive lymphadenopathy. Malignant transformation of cells has not been reported. Treatment consists of debulking surgery. Chemotherapy and radiotherapy may have beneficial effects. Many a times the disease goes into remission without any intervention.
The particular case has been reported for its rarity. We believe that this is the first reported case of concomitant involvement of central nervous system with enlargement of cervical, mediastinal, peripancreatic, para-aortic nodes, and of parotid glands in a single individual. The histopathological picture is similar to lymphoma but should be differentiated from lymphoma by its positivity for S-100 protein.

Acknowledgments
Source of funding Nil
Conflict of interest Nil
Contributor Information
H. Raja, Phone: +91-958-5235534, Email: drhraja@rediffmail.com
S. G. Subramanyam, Email: drsubramanyam.sg@rediffmail.com
References
- 1.Perry BP, Gregg CM, Myers S, Lilly S, Mann KP, Prieto V. Rosai-Dorfman disease (extranodal sinus histiocytosis) in a patient with HIV. Ear Nose Throat J. 1998;77(10):855–858. [PubMed] [Google Scholar]
- 2.Kruse AL, Gengler C, Gratz KW, Obwegeser JA. Extranodal manifestation of Rosai – Dorfman disease without involvement of lymphnodes. J Craniofac Surg. 2010;21(6):1733–1736. doi: 10.1097/SCS.0b013e3181f403ad. [DOI] [PubMed] [Google Scholar]
- 3.Kong YY, Kong JC, Shi DR, Lu HF, Zhu XZ, Wang J, Chen ZW. Utaneous Rosai-Dorfman disease: a clinical and Histopathologic study of 25 cases in China. Am J Surg Pathol. 2007;31(3):341–350. doi: 10.1097/01.pas.0000213387.70783.b6. [DOI] [PubMed] [Google Scholar]
- 4.Z'Graggen WJ, Sturzenegger M, Mariani L, Keserue B, Kappeler A, Vajtai I. Isolated Rosai – Dorfman disease of intracranial menninges. Pathol Res Pract. 2006;202(3):165–170. doi: 10.1016/j.prp.2005.11.004. [DOI] [PubMed] [Google Scholar]
- 5.Kademani D, Patel SG, Prasad ML, Huvos AG, Shah JP. Intraoral presentation of Rosai-Dorfman disease: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1993;93(6):699–704. doi: 10.1067/moe.2002.123495. [DOI] [PubMed] [Google Scholar]
- 6.Krishnan A, Nassar A, Nieh PT. Rosai-Dorfman disease presenting as extranodal renal mass. Urology. 2005;66(6):1319. doi: 10.1016/j.urology.2005.06.103. [DOI] [PubMed] [Google Scholar]
- 7.Chu P. LeBoit PE Histologic features of cutaneous sinus histiocytosis (Rosai-Dorfman disease): study of cases both with and without systemic involvement. J Cutan Pathol. 1992;19(3):201–206. doi: 10.1111/j.1600-0560.1992.tb01659.x. [DOI] [PubMed] [Google Scholar]
- 8.Lopes LF, Bacchi MM, Coelho KI, Filho AA. Bacchi CE Emperipolesis in a case of B-cell lymphoma: a rare phenomenon outside of Rosai-Dorfman disease. Ann Diagn Pathol. 2003;7(5):310–313. doi: 10.1016/j.anndiagpath.2003.06.002. [DOI] [PubMed] [Google Scholar]