

Abstract
Myxofibrosarcoma is a common connective tissue neoplasm of malignant fibrocytes in a myxoid matrix favoring the extremities. Like many other tumors of connective tissue, soft tissue sarcoma exhibits high recurrence rates but is rarely known to metastasize. We present a patient with myxofibrosarcoma of the hand with metastases to the lungs, pleura, and mediastinum. The mediastinal metastasis presented clinically with gastrointestinal symptoms due to compression of the gastroesophageal junction. To our knowledge, this is the first report of metastatic myxofibrosarcoma of the hand and also the first report of metastatic myxofibrosarcoma to mediastinal lymph nodes at the level of the gastroesophageal junction. We also performed a comprehensive literature review of metastatic myxofibrosarcoma.
Keywords: Myxofibrosarcoma, soft tissue sarcoma
Introduction
Myxofibrosarcoma is a connective tissue neoplasm of fibroblastic origin set in a myxoid matrix and has been classified by some as a myxoid variant of malignant fibrous histiocytoma [1, 2]. Fibrocyte proliferation yields stellate and spindle shaped cells with eosinophilic cytoplasm, indistinct borders, and elongated hyperchromatic, pleomorphic nuclei [1, 3-5]. The tumor is highly vascularized with distinct curvilinear thin walled capillaries [1, 3, 5]. Some tumors exhibit mucin-producing vacuoles resembling pseudolipoblasts [1, 3-5]. Apart from these general histologic parameters, myxofibrosarcomas demonstrate wide histologic variability based on the grade of the neoplasm [4, 6, 7]. Low grade tumors are hypocellular and composed mainly of myxoid tissue [1, 4, 6, 8]. High grade tumors, however, are hypercellular, malignant fibrous histiocytoma-like tumors with less myxoid tissue than their lower grade counterparts and present with multinucleated giants cells, increased mitotic activity, and areas of necrosis [4, 5, 7, 9]. These tumors stain positive for vimentin, CD34, and occasionally actin [3, 7, 8]. Gross presentation is most often of a slow-growing, painless, palpable and ill-defined subcutaneous mass [1, 4]. Tumors are glistening, gelatinous, gray to white lesions upon resection [3, 10].
Myxofibrosarcoma is a common soft-tissue sarcoma in elderly patients, presenting in the extremities (77%), trunk (12%), retroperitoneum or mediastinum (8%) and head (3%) [1]. Myxofibrosarcoma is, in fact, one of the most common neoplasms of the limbs of elderly patients [3, 7]. The majority of acral myxofibrosarcomas are observed in the leg rather than the arm, often attributed to the fact that the leg contains a greater volume of connective tissue and thus has a greater chance for malignant development [3, 7, 11]. Cases arising in the hand are rare but have been reported [12].
Case report
We present a 62 year-old African-American female with a past medical history significant for pulmonary embolism and a giant cell tumor of the right hand 16 years previously, treated at an outside facility. The patient presented to Tulane University Medical Center with a left hand mass which was subsequently widely excised and diagnosed as myxofibrosarcoma. The patient had also been complaining of some pleuritic chest pain as well as back pain and increased episodes of belching, weight loss, and changes in appetite. The patient was found on a Positron Emission Tomography (PET) exam to have bilateral metastatic pleural and pulmonary nodules as well as hypermetabolism with surgical correction in the left hand. A mediastinal mass was subsequently found on the patient and the patient was admitted for an endoscopic ultrasound and fine needle aspiration (FNA) of this mediastinal mass (Figure 1). Her mediastinal mass was adjacent to the gastroesophageal junction. The patient's FNA of the mass was diagnosed as myxofibrosarcoma metastatic from her left hand (Figure 2).
Figure 1.
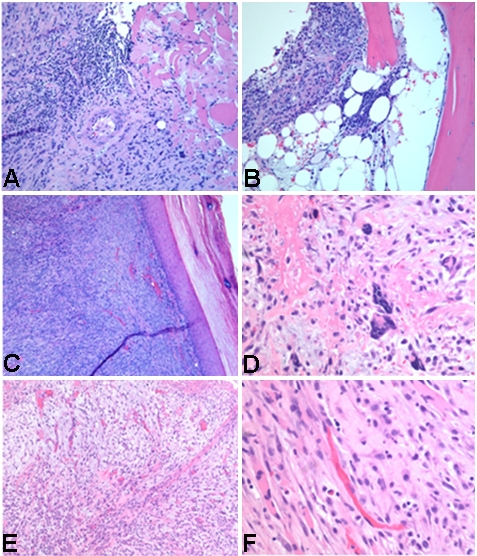
Pathologic images from the primary tumor (left hand mass) of the presented case. (a) Tumor is infiltrating the muscle and demonstrates vascular invasion. (b) Tumor is invading and destructing the bone. (c) Tumor is present within the superficial and deep dermis. (d) Areas with high grade tumor display pleomorphism with increased mitosis, more cellular-ity and multinucleated giant cells. (e, f) Characteristic elongated and curvilinear vascular pattern with spindle or satellite-shaped cells deposited in a myxoid matrix typically seen in myxofibrosarcoma.
Figure 2.

Chest CT with contrast of our patient demonstrates a metastatic lesion adjacent to the gastroesophageal junction.
Surgery for the metastatic disease was considered but ultimately not performed due to the diffuse metastatic disease. The patient followed up with her medical oncologist 6 days after discharge from the hospital and was advised about the fatal nature of her illness and recommended palliative chemotherapy. The patient moved out of state to be closer to her family and was subsequently lost to follow-up.
Discussion
Myxofibrosarcomas exhibit a multinodular growth pattern and are most often superficial lesions, distinguishing them from most other sarcomas which present as deeper tumors [1, 3, 5]. Masses are most commonly found in the subcutaneous tissue, sometimes with dermal involvement [1, 4, 8]. Rarely, myxofibrosarcomas originate in deep fascial or intramuscular tissue [1, 3, 4]. Despite their normally superficial derivation, myxofibrosarcomas display highly infiltrative growth patterns and spread extensively along fascial planes, making surgical resection especially difficult [2, 4]. Possibly related to this detail is the notoriously high rate of recurrence in myxofibrosarcoma cases, which does not correlate to tumor grade or size [3, 4, 12]. Merck et al found recurrence is more likely in more superficial tumors, however, there is not a general agreement in the literature regarding relationship between tumor depth and likelihood of recurrence [10]. Various papers have reported myxofibrosarcoma recurrence rates between 16-54%, most reporting on the higher end of the spectrum [2, 5, 6, 9, 12]. Myxofibrosarcoma has consistently demonstrated evolution into a higher grade lesion following recurrence [4, 6]. Patients with close surgical margins should therefore be considered for radiation therapy, and recurring masses should be widely excised, including the scar from the previous surgery [13].
Though recurrence rate for myxofibrosarcoma is high irrespective of tumor grade, metastasis is quite rare and occurs almost exclusively in higher grade tumors [3, 6, 7, 9]. As a general rule, the vast majority of upper extremity connective tissue neoplasms are benign; metastasis from this region is extremely rare [14]. Many papers claim favored sites of myxofibrosarcoma metastases to be the lung, pleura, lymph nodes, and skeleton, but specific examples are sparse [1, 11]. Some papers report cases of metastases without specifying site of tumor origin: authors Mentzel et al report 6 cases of myxofibrosarcoma with metastasis to the lung, 5 cases with metastases to the lymph nodes, 2 cases with metastases to skin and soft tissue and 1 case with metastasis to the bone, and authors Merck et al report cases of myxofibrosarcoma metastases to the lung, pleura, lymph nodes, and skeleton [6, 12]. Authors Huang et al report cases of primary myxofibrosarcoma of the arm, axilla, back, inguinal area, leg, and shoulder with 6 metastases to the lungs, 2 metastases to the pleura, 1 metastasis to the pelvic bone, and 1 metastasis to the axillary lymph nodes, but it is unclear which primary tumor produced which incidence of metastasis [15]. The only specific examples of reported cases of metastatic myxofibrosarcoma found in a literature search using PubMed are exhibited in Table 1. Our search yielded only 6 specific cases of metastatic myxofibrosarcoma from lower extremities, 2 specific cases of metastatic myxofibrosarcoma from upper extremities, and 6 specific cases of myxofibrosarcoma of any origin with metastases to the lung.
Table 1.
Reported cases in the literature of metastatic myxofibrosarcoma
| Tumor site of origin | Site of metastasis | Reference |
|---|---|---|
| Thoracic wall | Lung | Kaya et al, 2008[4] |
| Scapula | Bone and buttocks | Angervall et al, 1977[10] |
| Buttocks | Lung, mesentery, pancreas | Angervall et al, 1977 [10] |
| Thigh | Paravertebral tissue | Angervall et al, 1977[10] |
| Popliteal fossa | Inguinal lymph nodes | Angervall et al, 1977[10] |
| Knee | Inguinal lymph nodes | Angervallet al, 1977[10] |
| Lower leg | Lung and liver | Kaya et al, 2008[4] |
| Ankle | Upper lip, pancreas, lung, kidney | Angervall et al, 1977[10] |
| Upper arm | Lung | Kaya et al, 2008[4] |
| Forearm | Lung | Kaya et al, 2008[4] |
Though myxofibrosarcoma has a low metastasis rate, this case and the others we found in our literature search show that myxofibrosarcoma does in fact metastasize and can be fatal. These cases demonstrate the importance of wide surgical margins during initial tumor resection and aggressive follow-up, including thorough search for metastatic disease and consideration of radiation therapy in case with close surgical margins, measures which can drastically improve outcome in patients with myxofibrosarcoma.
Conclusion
We are reporting what we believe to be the first case of metastatic myxofibrosarcoma of the hand, and also the first case of myxofibrosarcoma metastatic to the mediastinum or the lymph nodes at the level of the gastroesophageal junction. Myxofibrosarcoma is a common tumor in the geriatric patient population, traditionally thought to be a non-metastatic lesion. These tumors do, however, have the potential to metastasize and can be fatal. It is important to search for metastatic disease and ensure wide surgical margins to provide the best possible outcome.
Acknowledgments
This work was fully supported by Tulane University and Tulane University Hospital.
References
- 1.Mansoor A, White CR. Myxofibrosarcoma presenting in the skin: clinicopathological features and differential diagnosis with cutaneous myxoid neoplasms. Am J Dermatopathol. 2003;25:281–286. doi: 10.1097/00000372-200308000-00001. [DOI] [PubMed] [Google Scholar]
- 2.Wada T, Hasegawa T, Nagoya S, Kawaguchi S, Kaya M, Ishii S. Myxofibrosarcoma with an infiltrative growth pattern: a case report. Jpn J Clin Oncol. 2000;30:458–462. doi: 10.1093/jjco/hyd115. [DOI] [PubMed] [Google Scholar]
- 3.Hollowood K, Fletcher CD. Soft tissue sarcomas that mimic benign lesions. Semin Diagn Pathol. 1995;12:87–97. [PubMed] [Google Scholar]
- 4.Kaya M, Wada T, Nagoya S, Sasaki M, Matsumura T, Yamaguchi T, Hasegawa T, Yamashita T. MRI and histological evaluation of the infiltrative growth pattern of myxofibrosarcoma. Skeletal Radiol. 2008;37:1085–1090. doi: 10.1007/s00256-008-0542-4. [DOI] [PubMed] [Google Scholar]
- 5.Zelger B. Connective tissue tumors. Recent Results Cancer Res. 2002;160:343–350. doi: 10.1007/978-3-642-59410-6_39. [DOI] [PubMed] [Google Scholar]
- 6.Mentzel T, Calonje E, Wadden C, Camplejohn RS, Beham A, Smith MA, Fletcher CD. Myxofibrosarcoma. Clinicopathologic analysis of 75 cases with emphasis on the low-grade variant. Am J Surg Pathol. 1996;20:391–405. doi: 10.1097/00000478-199604000-00001. [DOI] [PubMed] [Google Scholar]
- 7.Ninfo V, Montesco MC. Myxoid tumors of soft tissues: a challenging pathological diagnosis. Adv Clin Path. 1998;2:101–115. [PubMed] [Google Scholar]
- 8.Motoda N, Akiyama M, Aoyagi S, Sawamura D, Shimizu H. Low-grade myxofibrosarcoma invaded into the underlying skeletal muscle. J Dermatol. 2007;34:561–564. doi: 10.1111/j.1346-8138.2007.00331.x. [DOI] [PubMed] [Google Scholar]
- 9.Kilpatrick SE, Ward WG. Myxofibrosarcoma of soft tissues: cytomorphologic analysis of a series. Diagn Cytopathol. 1999;20:6–9. doi: 10.1002/(sici)1097-0339(199901)20:1<6::aid-dc2>3.0.co;2-b. [DOI] [PubMed] [Google Scholar]
- 10.Angervall L, Kindblom LG, Merck C. Myxofibrosarcoma. A study of 30 cases. Acta Pathol Microbiol Scand A. 1977;85A:127–140. [PubMed] [Google Scholar]
- 11.Arenson DJ, Miceli JS, Bush WJ, Hussain A. Myxofibrosarcoma of the lower extremity. A case report. J Am Podiatr Med Assoc. 1986;76:102–105. doi: 10.7547/87507315-76-2-102. [DOI] [PubMed] [Google Scholar]
- 12.Merck C, Angervall L, Kindblom LG, Odén A. Myxofibrosarcoma. A malignant soft tissue tumor of fibroblastic-histiocytic origin. A clinicopathologic and prognostic study of 110 cases using multivariate analysis. Acta Pathol Microbiol Immunol Scand Suppl. 1983;282:1–40. [PubMed] [Google Scholar]
- 13.Mutter RW, Singer S, Zhang Z, Brennan MF, Alektiar KM. The enigma of myxofibrosarcoma of the extremity. Cancer. 2011. [DOI] [PMC free article] [PubMed]
- 14.Murray PM. Soft tissue sarcoma of the upper extremity. Hand Clin. 2004;20:325–333. doi: 10.1016/j.hcl.2004.03.007. [DOI] [PubMed] [Google Scholar]
- 15.Huang HY, Lal P, Qin J, Brennan MF, Antonescu CR. Low-grade myxofibrosarcoma: a clinicopathologic analysis of 49 cases treated at a single institution with simultaneous assessment of the efficacy of 3-tier and 4-tier grading systems. Hum Pathol. 2004;35:612–621. doi: 10.1016/j.humpath.2004.01.016. [DOI] [PubMed] [Google Scholar]
- 16.Soilleux EJ, Rous B, Love K, Vowler S, Morris LS, Fisher C, Coleman N. Myxofibrosarcomas contain large numbers of infiltrating immature dendritic cells. Am J Clin Pathol. 2003;119:540–545. doi: 10.1309/JEB7-DGHH-01J1-1VUM. [DOI] [PubMed] [Google Scholar]
- 17.Batra S, Batra M, Sakamuri R, Sinha AK, Kanvinde R. High-grade infiltrative myxofibrosarcoma in the forearm presenting as acute carpal tunnel syndrome. J Hand Surg Am. 2008;33:269–272. doi: 10.1016/j.jhsa.2007.10.019. [DOI] [PubMed] [Google Scholar]