

Abstract
Background:
Menstruation is a phenomenon unique to females and nearly universal experience in women's lives and is poorly understood. This study has been done to assess menstrual pattern and associated factors.
Materials and Methods:
A total of 194 girl students aged 18 to 27 years were selected and asked to complete a questionnaire anonymously. Data regarding demographic features, menarche age, menstrual pattern, severity of dysmenorrhea and associated symptoms, and impact of menstrual pain on working ability were obtained. Source for information about menarche and menstruation the participants depend was also elicited.
Results:
Mean age of the subjects at menarche was 13.36 ± 1.25 years with a range being 10 to 17 years. Mean duration of menstrual flow was 4.77 ± 1.06 days. The most prevalent menstrual symptoms were tiredness (47.9%), backache (38.3%), and anger (34.5%). Prevalence of menstrual irregularity and dysmenorrhea was 11.9 and 78.2%. 6.7% of the participants had severe dysmenorrhea. 76.6% of the dysmenorrheic girls reported that their working ability was affected. 60.4% of the girls were aware of menstruation prior to menarche. Mothers and friends were the main sources of information (47.8%).
Conclusion:
In conclusion, it can be mentioned that prevalence of dysmenorrhea and menstrual irregularity among young females is high. Working ability is reported to be affected by menstrual pain. It could be possible to improve menstrual discomforts management by including awareness programs.
Keywords: Flow, menarche, menstrual pain, menstrual symptoms
INTRODUCTION
Menstrual cycle is the cyclical shedding of endometrium every 28 ± 7 days in response to hormones. It is a natural phenomenon that occurs throughout the reproductive years of every woman's life during which blood loss per cycle is not greater than 50 ± 30 ml with or without discomfort.[1] A woman on an average undergo 400 menstrual cycles prior to menopause. The average menstrual cycle lasts for about 5 days, which accounts to approximately 67 months of menstrual bleeding over a lifetime.[2]
The adult pattern of ovulatory cycles is 21 to 34 days long, while the young females experience irregular pattern.[3] 75% of adolescent girls are reported to have menstrual dysfunction and is known to affect the normal daily chores. Delayed, irregular, painful, and heavy menstrual bleeding are common occurrence among younger age and are the leading reasons for physician office visits by adolescents.[4] Dysmenorrhea is yet another major cause of activity restriction and school absenteeism in adolescent girls. However, the condition is often considered as physiological pain and generally ignored. A few of the adolescents consult physician for the problem and many adopt self-medication with over-the-counter medicines or home remedies.[5] Therefore, statistics about prevalence of menstrual problems or dysmenorrhea and their causes are poorly available due to under-reporting.
Menstrual patterns are influenced by a number of host and environmental factors.[6] Knowledge regarding the factors influencing menstrual symptoms are important in order to manage it effectively and help women make up the days less troublesome and tolerable. Very few studies are available from India discussing menstrual pattern.
A cross-sectional study was therefore conducted to determine patterns of menstrual cycles among young girls and its related problems, discomfort and working ability of girls during the period. Also to infer the extent of awareness and sources for information regarding menstruation possessed by Indian girls before attaining puberty.
MATERIALS AND METHODS
Participants of the present study were 194 unmarried female students studying in various degrees level classes from undergraduate and postgraduate institutions from Mysore city. Purposive sampling was adopted to select the subjects; those women who cooperated to provide correct and complete information and fitted into the study criteria were included for the study.
Criteria for selection
Inclusion criteria - aged between 18 to 27 years, menstruating, and unmarried; Exclusion criteria - age less than 18 and more than 27 years, married, and those with known secondary dysmenorrhea and other metabolic disorders. The study was conducted during the academic years 2008 – 2009. The selected women were requested to complete the questionnaires to elicit information relating to demographic features, menarche age, and menstrual pattern. Severity of dysmenorrhea was measured using the Visual Analogue Scale developed by Revill et al.[7] Impact of menstrual disorder on working ability, the source of knowledge about menarche, and menstruation was also obtained using a pretested questionnaire developed for the purpose. Information regarding menstrual bleeding was obtained by interview method using a pictorial chart to describe the degree to which the sanitary wear was soiled, as suggested by Higham et al.[8]
Statistical analysis
The data were analyzed using SPSS for Windows version 16.0. Descriptive statistics was used to determine mean age of the subjects, age at menarche, frequency of menstrual disorders, prevalence of dysmenorrheal, and activities affected by this condition. The categorical data were analyzed using Chi Sq. or Fisher's exact test.
RESULTS
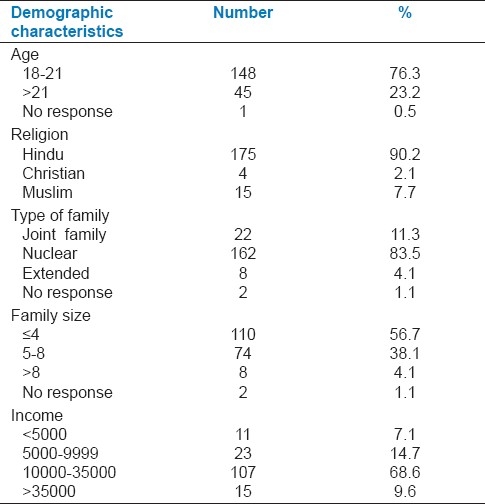
Demographic characteristics of the subjects are presented in Table 1. It is evident that the participants were young adults aged more than 18 years (18 - 27 years) with a mean age being 20.6 ± 1.32 years. The major religion of the subjects was found to be Hinduism (90.2%). Muslims and Christians were 7.7% and 2.1%, respectively. Nuclear family system was predominant followed by joint families. Higher percentage of the participants belonged to families with ≤4 members (56.7%) and 5 to 8 members (38.1%). Income is a most important variable affecting health and wellbeing of individuals; the selected subjects had family income varying from Rs. <5 000 to >35 000 per month. Nearly 70% of the subjects had a family income between Rs. 10 000 to 35 000.
Table 1.
Demographic characteristics of young adult women in Mysore, India
The menstrual pattern of the selected subjects is presented in Table 2, it can be seen that the mean age of menarche was 13.36 ± 1.25 years exhibiting wide variations, i.e., 10 to 17 years among the participants. Sixty percent of participants were aware of menstruation before attaining menarche. Source for information varied from mothers and friends to TV, magazines, and newspaper; nevertheless, the major sources were mothers and friends (47.8%). The mean duration of experience of menstruation among the selected subjects was 7.25 ± 1.95 years, having a range between 3.05 to 14.26 years. Also, frequency of the cycle length and duration of flow is presented in the Table. Menstrual characteristics as indicated by the selected subjects are presented in Table 3. It is evident from our results that 42 to 53% of the participants in the two age categories, i.e., <21 and >21 years, respectively, experienced excessive bleeding (scores >80) as per the pictorial chart and 77 to 80% were found to have dysmenorrhea. Menstrual irregularity however was of less occurrence, 13.5% of subjects in the younger age group (18 to 21 years) experienced frequent irregular menstruation than those of older age (6.6%). It is further interesting to mention that menarche age was found to exert an effect on blood loss per menstrual cycle and occurrence of dysmenorrhea. Excessive blood loss was found to be associated to menarche age; it can be perused from the Table that frequency of excessive blood loss was higher in females with early menarche. The inverse relation between age of menarche and blood loss was found to have statistically significant association (P = 0.029). It is also evident that higher percentage of girls who encompassed menarche at an earlier age experienced dysmenorrhea more than those who had late menarche (P = 0.001). However, menstrual irregularity was found to be independent to age of menarche (P = 0.138).
Table 2.
Menstrual pattern and menarche age among the selected girls
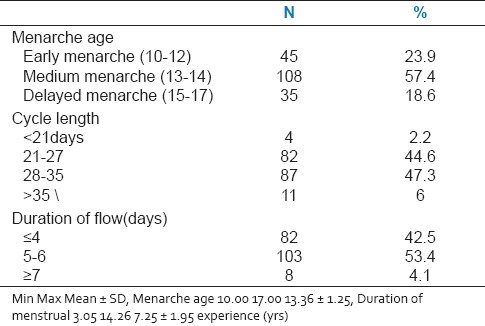
Table 3.
Menstrual characteristics of young adult women in Mysore, India, P<0.05
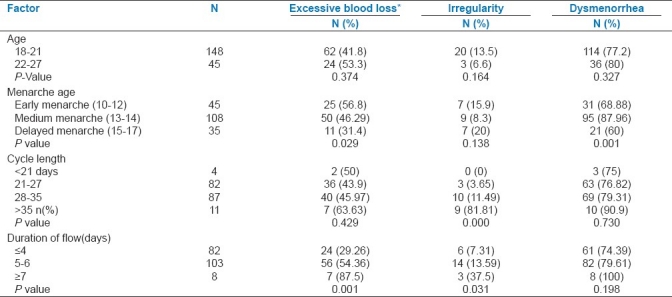
We also found an extremely significant association between cycle length and frequency of irregularity. Irregular menstrual cycles were frequent among girls who had cycle length >35 days. Although occurrence of dysmenorrhea was independent to cycle length, all those who had cycle length >35 days were dysmenorrheic. It could be possible that females with longer cycles suffer from dysmenorrhea. The Table also presents data regarding duration of menstrual flow and menstrual problems; it is plausible that with longer duration of flow, total loss of blood tends to be higher. It is also obvious that females with longer duration of flow experienced irregular menstrual pattern and statistically mildly significant; nevertheless, the actual number of subjects in this category were very small.
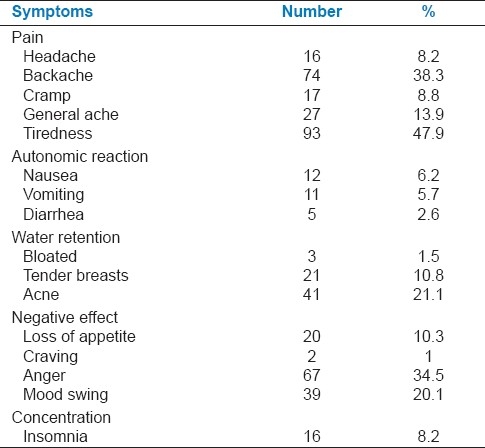
Prevalence of menstrual symptoms is listed in Table 4; most prevalent symptoms were tiredness (47.9%), backache (38.3%), and anger (34.5%).
Table 4.
Prevalence of menstrual symptoms
The pain characteristics observed among the dysmenorrheic females are presented in Table 5. It can be perused that 78.2% of the participants suffered from pain. Different locations for pain were revealed by the subjects, the most frequent pain location was lower abdomen followed by low back and a co-occurrence of abdominal and low back pain. The characteristic of pain experienced was revealed as twisting or stinging sharp pain by majority of the participants. Nearly 50% of the participants mentioned to have experienced pain after one year of the menarche, while 39% experienced pain from the first period. It is worthwhile mentioning that dysmenorrheic females also experienced painless menstrual cycles though less frequently. The proportion of participants who experienced painful and painless menstruation was as follows: 68% of girls experienced every cycle to be painful, 10.4% had painful menstruation less frequently, i.e., on an average pain once in 3 months, and 21.6% experienced pain rarely, i.e., once in 6 months.
Table 5.
Characteristics of dysmenorrhea
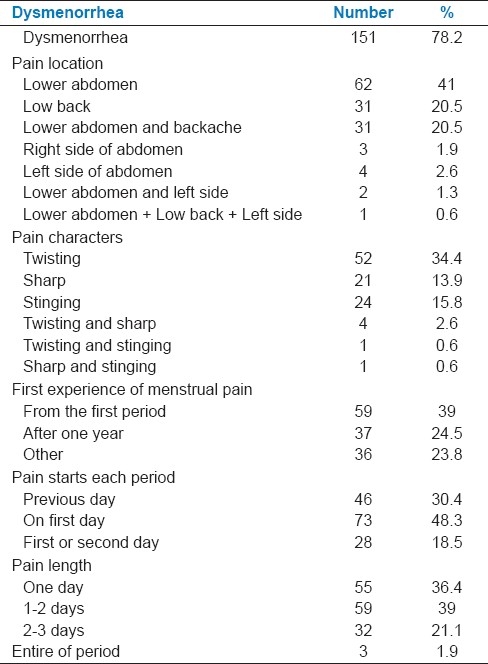
Furthermore, majority of the females with dysmenorrhea mentioned that the pain commenced from first or second day of the menstruation. The duration of pain varied from one day to the entire period, higher percentage of subjects experienced pain for one to two days.
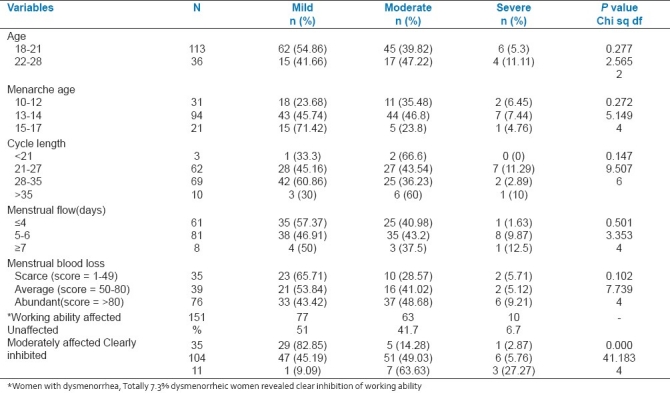
It was proposed to identify the association between certain menstrual characteristics and severity of dysmenorrhea. The Chi Sq analysis indicated its independence to all the selected variables except for work ability. It is apparent from Table 6 that percent distribution of females from two different age categories into severity was essentially similar; pattern of distribution for other variables was analogous to this. The severity of pain related to dysmenorrhea could probably restrict movement affecting working ability since 48 and 49% of the participants from mild and moderate dysmenorrheal, respectively, reported to be affected moderately during the menstrual time; therefore, a significant dependency was exhibited according to Chi Sq analysis.
Table 6.
Comparison of certain factors according to dysmenorrhea status
DISCUSSION
Regional and racial differences have been reported to affect menarche age,[9,10] various factors such as heredity, environmental conditions, body stature, socioeconomic status, nutritional and health status, family size, level of education, and psychological well being are known to influence menarche age.[10,11] The mean age for menarche observed in the present study from Mysore urban was 13.36 ± 1.25 years; this is inconsistent with studies reported from other parts of India. Although small differences are obvious between the reported ages, varying from 13.06 ± 1.43 years in West Bengal[12] to 13.4, 13.5, and 13.6 years in Goa, Chennai, and East Delhi, respectively.[13–16] Recent reports from many countries of the world indicate a decline in the mean age; the current age as per reports from European and North American countries is 12.5 years, while 12.8 ± 1.3 years is from Turkey.[5,9,10]
Variations have been encountered in population for cycle duration and extent of flow, inter- and intra-individual variations are also common. A few studies from south India indicated that 1 and 12% of women encountered shorter (<21 days) and longer cycles (>35 days), respectively.[17] In accordance to these reports, we observed 2.2% and 4.1% of the participants to encompass short and long menstrual periods, respectively. However, higher percentages (7-24%) of occurrence are reported from Turkey and Nigeria.[18] Similarly, reports have indicated variations in duration of flow, the mean duration being 5.3 ± 1.32 days and stretched to more than 7 days for Indians. One to four percent of women population is reported to have long duration of flow.[18] We found a mean duration of 4.77 ± 1.06 days as the normal period of menstrual flow, with 4.1% of participants having more than 7 days. Furthermore, it is evident that a major proportion of the females experience abundant discharge during the menstruation. Studies indicate occurrence of large variations in menstrual loss among women population, 23.5% women from West Bengal;[15] 8 to 9% women from India and neighboring countries were reported to encounter heavy discharge.[19] In contrast to other reports from India, our study observed a larger proportion (44.5%) of the participants to have experienced abundant discharge. The reason for such an observation is not known whether the age or other environmental factors exert the influence. Differences in the method of evaluation could also possibly affect the results.
Irregularity in the monthly shedding is also indicated in different studies, percent occurrence from Bangladesh,[19] Lebanon,[20] and Gambia[21] varied from 3 to 16%, whereas studies from India presents a figure of 5 to 9%.[22] In the present study, prevalence of irregular cycles was 11.9%. It could be possible that the increase in the incidence of irregularity is due to changes in lifestyle that is being introduced in different spheres of life.
Dysmenorrhea is an important menstrual disorder in adolescence, and common in young women with ovulatory cycles. Recently, it has become an important public health problem among the female population; prevalence rate reported from different states of India appears to be as follows: Delhi, 63.75% and[12] Chennai, 61%.[13] In certain regions, prevalence rate are as high as 71 to 93%; these variations can be due to difference in region-specific environment, age of participants, and study protocol.[23–25] Prevalence of dysmenorrhea among the selected group was 78.2%, and it was associated to early menarche age; similar observation is reported among Moroccan girls.[26] Probably early onset of menarche leads to earlier ovulatory cycles and an earlier experience of dysmenorrhea.
Occurrence of severe pain during menstrual period accounts to 3-20% in most population[26–28]; our results coincide with these reports (6.7%). It is also evident from these studies that severity of pain decrease with increase in age, and older women experience severe pain less frequently.[29] Our results exhibited a small effect of age on severity of pain; however, it was statistically not significant. Also, 46.5% of the dysmenorrheic girls opined that pain continued to be as severe as at that experienced on the first incidence of menstrual pain.
Immobility (clearly inhibited) due to pain during menstrual period was seen in 7.3% of the dysmenorrheic girls including the various intensity of dysmenorrhea. 68.8% of the participants mentioned that their working ability was affected to moderate extent, the association between severity of pain and limited work ability was statistically significant (P = 0.000). Other studies indicate 3 to 18%[21] girls to be affected severely and 52% to be moderately or mildly affected.[30] Especially, the college and university students (46%) had absenteeism due to menstrual pain and were highly associated statistically. Similar results have been reported from other regions.[25,29] It is important to know the health problems of the general population so that corrective measures can be incorporated in the health intervention programs; our study has contributed to the current health-related problems of women which curtails their productivity. Although the problem faced by the women is for a short duration, the repetitiveness makes it a serious concern and requires a corrective measure.
Awareness regarding menarche is common among young girls before encompassing it, ranging from 42.5% in rural areas to 66.1% among urban counterparts. The major source for information was mothers, friends, or the information media, such results were also reported by other works.[5,14,12,31]
In conclusion, dysmenorrhea and menstrual irregularity are more prevalent among young females. Common symptoms of dysmenorrhea are tiredness, anger, and backache; the pain that is characteristic to dysmenorrhea varies in intensity. Those females who experienced severe pain suffered with abdominal cramps, vomiting, and loss of appetite including immobility. It appears that occurrence of dysmenorrhea is increasing in population; such sufferings would affect the productivity among females. Therefore, it can be stated that a comprehensive school education program on menarche and menstrual problems may help girls to cope better and seek proper medical assistance.
The limitation of the present study is that it consists only of College and University students, and may not represent the frequency of dysmenorrhea and other menstrual disorders among young women in the general population.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Beek, Jonathan S. Novak's Gynecology. 14th ed. London: Williams and Wilkins publication Inc; 2006. “Puberty and dysmenorrhea treatment”; p. 1696. [Google Scholar]
- 2.Chiou MH, Wang HH, Yang YH. Effect of systematic of menstrual health education on dysmenorrheic female adolescents’ knowledge, attitudes, and self-care behavior. Kaohsiung J Med Sci. 2007;23:183–90. doi: 10.1016/S1607-551X(09)70395-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hickey M, Balen A. Menstrual disorders in adolescence investigation and management. Hum Reprod Update. 2003;9:493–504. doi: 10.1093/humupd/dmg038. [DOI] [PubMed] [Google Scholar]
- 4.Ziv A, Boulet JR, Slap GB. Utilization of physician offices by adolescents in the United States. Pediatrics. 1999;104:35–42. doi: 10.1542/peds.104.1.35. [DOI] [PubMed] [Google Scholar]
- 5.Cakir M, Mungan I, Karakas T, Girisken L, Okten A. Menstrual pattern and common menstrual disorders among university students in Turkey. Pediatrics Int. 2007;49:938–42. doi: 10.1111/j.1442-200X.2007.02489.x. [DOI] [PubMed] [Google Scholar]
- 6.Siddiqui N, Pi Tking J. Menstrual disturbances. Obstet, Gynecol and Reprod Med 2007. 2007;17(5):154–62. [Google Scholar]
- 7.Revill SI, Robinson JO, Rosen M, Hogg MI. The reliability of a linear analogue for evaluating pain. Anesthesia. 1976;31:1191–8. doi: 10.1111/j.1365-2044.1976.tb11971.x. [DOI] [PubMed] [Google Scholar]
- 8.Higham J, O’Brien PM, Shaw RW. Assessment of menstrual blood loss using a pictorial chart. Br J Obstet Gynaecol. 1990;97:734–9. doi: 10.1111/j.1471-0528.1990.tb16249.x. [DOI] [PubMed] [Google Scholar]
- 9.The museum of Menstruation and women's health. Average age at menarche in various cultures. [Last accessed on 2003 Jul]. Available from: http://www.mom.org .
- 10.Ayatollahi SM, Dawlatabadi E, Ayatollahi SA. Age at menarche and its correlates in Shiraz, Southern Iran. Iranian J Med Sci. 1999;24:20–5. [Google Scholar]
- 11.Koo MM, Rohan TE, Jain M, McLaughlin JR, Corey PN. A cohort study of dietary fiber intake and menarche. Public Health Nutr. 2002;5:353–60. doi: 10.1079/PHN2002261. [DOI] [PubMed] [Google Scholar]
- 12.Nair P, Grover VL, Kannan AT. Awareness and practices of menstruation and pubertal changes amongst unmarried female adolescents in a rural area of East Dehi. Indian J Community Med. 2007;32:156–7. [Google Scholar]
- 13.Sheila W, Malathy K, Premila S. Menstrual and gynecological disorders in 500 school girls in Madras city. J Obstet Gynecol India. 1993;43:940–5. [Google Scholar]
- 14.Grover VL. Final report on a study of reproductive health awareness and sexual behavior among adolescents in Delhi: Report submitted to ICMR: Delhi. 1998 [Google Scholar]
- 15.Sanyal S, Ray S. Variation in the menstrual characteristics in adolescents of West Bengal. Singapore Med J. 2008;49:542–50. [PubMed] [Google Scholar]
- 16.Patel V, Tanksale V, Sahasrabhojanee M, Gupte S, Nevrekar P. The burden and determinants of dysmenorrhoea: a population-based survey of 2262 women in Goa, India. BJOG. 2006;113:453–63. doi: 10.1111/j.1471-0528.2006.00874.x. [DOI] [PubMed] [Google Scholar]
- 17.Jeyaseelan L, Rao PS. Effect of occupation on menstrual cycle length: causal model. Hum Biol. 1995;67:283–90. [PubMed] [Google Scholar]
- 18.Fakeye O, Adegoke A. The characteristics of the menstrual cycle in Nigerian school girls and the implications for school health programmes. Afr J Med Med Sci. 1994;23:13–7. [PubMed] [Google Scholar]
- 19.Harlow SD, Campbell OM. Epidemilogy of menstrual disorders in developing countries: a systematic review. BJOG. 2004;111:6–16. doi: 10.1111/j.1471-0528.2004.00012.x. [DOI] [PubMed] [Google Scholar]
- 20.Deeb M, Ghorayeb F, Kabakian-Khasholian T, Yeretzian J, Aswad N. Measuring gynencological morbidity:evaluating two different data sources from Beirut. Health Care Women Int. 2003;24:254–65. doi: 10.1080/07399330390183561. [DOI] [PubMed] [Google Scholar]
- 21.Walraven G, Ekpo G, Coleman R, Scherf C, Morison L, Harlow SD. Menstrual disorders in rural Gambia. Stud Fam Plann. 2002;33:261–8. doi: 10.1111/j.1728-4465.2002.00261.x. [DOI] [PubMed] [Google Scholar]
- 22.Bhatia JC, Cleland J, Bhagavan L, Rao NS. Levels and determinants of gynecological morbidity in a district in south India. Stud Fam Plann. 1997;28:95–103. [PubMed] [Google Scholar]
- 23.Campbell MA, McGrath PJ. Non-pharmacologic strategies used by adolescents for the management of menstrual discomfort. Clin J Pain. 1999;15:313–20. doi: 10.1097/00002508-199912000-00008. [DOI] [PubMed] [Google Scholar]
- 24.Banikarim C, Chacko MR, Kelder SH. Prevalence and impact of dysmenorrhea on Hispanic female adolescents. Arch Pediatr Adolesc Med. 2000;154:1226–9. doi: 10.1001/archpedi.154.12.1226. [DOI] [PubMed] [Google Scholar]
- 25.Poureslami M, Osati-Ashtiani F. Assessing knowledge, attitude, and behavior of adolescent girls suburban districts of Tehran about dysmenorrhea and menstrual hygiene. J Int Womens Studies. 2002;3:1–11. [Google Scholar]
- 26.Montero P, Bernis C, Loukid M, Hilali K, Baali A. Characteristics of menstrual cycles in Moroccan girls: prevalence of dysfunctions and associated behaviours. Ann Hum Biol. 1999;26:243–9. doi: 10.1080/030144699282741. [DOI] [PubMed] [Google Scholar]
- 27.Aggarwal K, Kannan AT, Puri A, Sharama S. Dysmenorrhea in adolescent girls in a rural area of Delhi: a community – based survey. Indian J Public Health. 1997;41:84–5. [Google Scholar]
- 28.Vaidya RA, Shringi MS, Bhatt MA, Gajjar M, Joshi JV, Galvankar P, Sankari P. Menstrual pattern and growthof school girls in Mumbai. J Fam Welf. 1998;44:66–72. [Google Scholar]
- 29.Weissman AM, Hartz AJ, Hansen MD, Johnson SR. The natural history of primary dysmenorrhoea: a longitudinal study. BJOG. 2004;111:345–52. doi: 10.1111/j.1471-0528.2004.00090.x. [DOI] [PubMed] [Google Scholar]
- 30.Hillen TI, Grbavac SL, Johnston PJ, Straton JA, Keogh JM. Primary dysmenorrhoea in young Western Australian women: prevalence, impact, and knowledge of treatment. J Adolesc Health. 1999;25:40–5. doi: 10.1016/s1054-139x(98)00147-5. [DOI] [PubMed] [Google Scholar]
- 31.Deo DS, Ghattargi CH. Perceptions and practices regarding menstruation: A comparative study in urban and rural adolescent girls. Indian J Community Med. 2005;30:33–4. [Google Scholar]