

Abstract
Background:
Although Atraumatic restorative treatment (ART) approach has been in existence for a while, the reasons for the poor performance of multisurface ART restorations are not very clear.
Aim:
The aim of this study is to investigate the effects of oral hygiene, residual caries and cervical marginal-gaps on survival of proximal ART restorations.
Settings:
Two rural divisions in Kenya were selected for the study.
Design:
A randomized clinical trial.
Material and Methods:
The 804 children in the study had their baseline- and 2-year dental plaque levels documented. Each child received one proximal restoration in a primary molar using ART approach, together with trained and pre-tested operators/assistants, three glass ionomer cements (GIC)-brands and two tooth-isolation methods. The restorations were clinically evaluated soon after placement and after 2 years. Post-restorative bite-wing radiographs taken soon after restoration were also evaluated.
Statistical analysis:
Statistical Package for Social Sciences (SPSS) version 14 computer programme was used and results tested using Pearson's correlation, Cox Proportional Hazards regression analysis and Multiple Logistic regression models tests.
Results:
At baseline and after 2 years, the mean cumulative survival and plaque index changed from 94.4% to 30.8% and 2.34 (Standard Deviation, or SD of 0.46) to 1.92 (SD 2.1) respectively, with higher plaque indices associated with higher restoration failures. Of the 507 radiographs evaluated, 48 (9.5%), 63 (12.4%) and 9 (1.8%) restorations had residual caries (RC), cervical marginal-gaps (CMG) and both RC/CMG respectively. Survival of the restorations with RC/CMG was significantly lower (p = 0.003) compared to those with RC or without RC.
Conclusion:
Low survival of proximal restorations in the study was associated with the presence of cervical marginal-gaps.
Keywords: Atraumatic restorative treatment, cervical marginal-gaps, dental plaque, primary molars, proximal restorations, residual caries
Introduction
Without a clear clinical demarcation, a carious lesion involving the dentine has an inner layer which is sensitive and partly demineralised and an outer layer that is insensitive and highly demineralised with high bacterial count.[1] Atraumatic restorative treatment (ART) approach, a technique used to manage dental caries, relies on the removal of this outer layer of the carious lesion using hand instruments and sealing the prepared cavity with an adhesive restorative material.[2,3] When removing the carious material using hand instruments, some residual carious material and/or cariogenic bacteria tend to remain behind.[4] This residual carious material can partly contribute to poor cavo-material bonding and result in marginal gap-formation. Additionally, poor application or salivary contamination of the restorative material in the case of multi-surface restorations can also result in voids- and marginal gap-formation. Such cervical marginal gaps so formed can predispose the tooth to secondary caries, due to their plaque retentive-capability, or cause the seepage of vital nutrients to the remnant bacteria under the restoration. All these factors will lead to new or to the continuation of the dental carious processes. On the other hand, if an adequate hermetic seal is present, the remnant bacteria left under the restoration may not survive during the placement of the restorative material, or may be unable to reactivate the carious process.[5,6] The hermetic-seal deprive the remnant bacteria of the needed vital nutrients for their metabolism.[7] Thus, the combined presence of residual caries and cervical gaps can cause considerable influence on the integrity of a restoration.[8,9]
ART restorations show equivalent short-term survival rates. However, the same cannot be said of the survival rates of the multi-surface ART restorations, which is very low as compared to the single surface restorations.[10–12] Failures of the ART restorations have generally been associated with poor material handling and inadequate removal of caries during the caries excavation stage.[13] Another factor affecting the success of ART restorations is poor oral hygiene.[14] The purpose of the present study was to determine what effects oral hygiene, residual caries and cervical marginal gaps have on the survival rate of proximal ART restorations placed in the primary molars when using 3 brands of GIC and 2 methods of tooth-isolation. The null hypothesis was that the survival rate of proximal ART restorations is not influenced by the oral hygiene, residual caries or cervical marginal gaps.
Materials and Methods
Subjects and settings
The present study formed part of a two-year clinical investigation on factors influencing the quality and survival rate of proximal ART restorations. The 804 children, who participated in the study, were drawn from 30 randomly selected schools out of the 142 public schools in Matungulu and Kangundo divisions, Machakos district, Kenya. Ethical approval was obtained from Nairobi University Ethical Committee and the parents/guardians provided a written informed consent for the child's participation. All the children selected were in good general health, had at least one proximal carious lesion in the primary molar and assented to the examination. The criteria for the selection of the appropriate proximal carious lesions were similar to that used by Kemoli et al.[15] with the selected proximal cavity having an occlusal access of approximately 0.5 mm to 1.0 mm in the bucco-lingual direction. This size of the cavity-access allowed for easy entry of the smallest excavator into the cavity. Where more than one cavity existed in a child, the smallest of them all was chosen. The selected tooth did not show any signs or symptoms of pain or mobility.
Demographic data and oral hygiene
The baseline ages of the study population ranged from 6 to 8 years. Using a questionnaire directed to the parent/guardian of the participants, information on family history and the oral hygiene practices of the subjects was obtained. Trained and pre-tested pediatric dentist and two final-year dental students, paired with an equal number of dental assistants, used Greene and Vermillion criteria[16] to assess and document the baseline oral hygiene (represented by plaque index) of each child. The same pediatric dentist and dental assistants, but with two postgraduate dental students who had also been trained and pre-tested, similarly repeated the process after two years.
Calibration of examiners of dental plaque
Cohen's coefficient[17] was used to calculate the examiner-agreement in the assessment of plaque. The Kappa mean values were 0.85 (n = 28) and 0.86, (n = 24) for the respective group used at baseline and after two years. The mean inter- and intra-examiner repeatability for both groups ranged from Kappa 0.80 to 1.0, n = 32 - 40.
Restoration procedure
Seven operators and 8 assistants, randomly paired to each other (one assistant resting on any day of operation) restored the 804 proximal carious lesions in the selected primary molars. Although one of the operators had had some previous experience with the ART approach, nonetheless, all the operators and the assistants underwent a thorough training in their relevant roles in applying the ART technique, as per the World Health Organization (WHO) approved ART manual.[18] After the training they were further allowed to practice with the technique, under supervision, in order to gain experience with the technique. They were all pre-tested in the use of the technique on a sample of children not included in the study, before they took part in the study. Using random numbers, the children were on each operation day assigned to an operator, an assistant, an isolation method and to glass ionomer cement (GIC) material. Two isolation methods (rubber dam or cotton wool rolls), and three brands of GIC (Fuji IX (GC Europe), Ketac Molar Easymix (3M ESPE AG, Germany) or Ketac Molar Aplicap (3M ESPE AG, Germany) were used. Only one primary molar per child was restored. No local anaesthetic injection was used during the restoration stage, except for Lidocaine (50mg/g cream) applied topically for 2 minutes on the surrounding gingiva of the tooth to be restored prior to placing the rubber dam clamp.
Using light forces and a spoon excavator, and aided by a caries-detector dye (private label based on acid red from Academic Centre for Dentistry Amsterdam (ACTA), the Netherlands) as much carious material as possible was removed from the cavity. The cavity was then cleaned and dried with cotton pellets. For the deep cavities, a small layer of calcium hydroxide (Dycal, Caulk-Dentsply, USA) was placed as a thin lining at the deepest points before restoring them. If pulpal exposure occurred during the cavity preparation, the participant was excluded from the study, but emergency dressing of the affected tooth was completed and the child was referred for definitive treatment at the local hospital. A post-operative bite-wing radiograph of the restored tooth was taken soon after placing the restoration and before releasing the child, with the advice not to chew any food within the next hour. The radiographs taken were not immediately available to the operators as it was not easy to do this in the field. They had to be transported approximately 65 Kilometres to the main city for processing, which took a considerable amount of time before the radiographs could be evaluated. As a result of the poor terrain of the study area, of the three mobile radiograph machines that were arranged to be used during the study, two broke down beyond repair. This resulted in technical difficulties that made it impossible to take other sets of radiographs after 2 years. Oral health education and any emergency dental treatments were provided by dental assistants to the study population over the two-year period of study.
Post-operative evaluation process
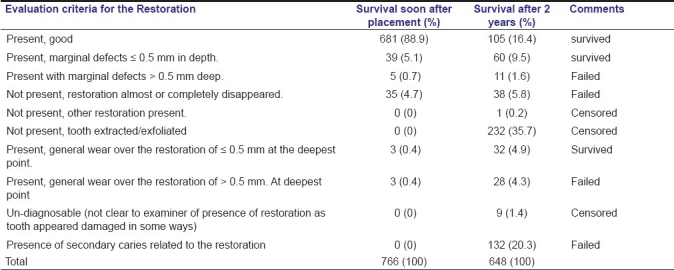
Trained and calibrated examiners, who did not have any knowledge of the previous oral health or tooth/restorations status of the children, clinically evaluated the restorations, soon after placement (within 2 hours) and after two years using the criteria by Kemoli et al.[15] Due to truancy, 38 of the 804 children in the study failed to present themselves for the initial evaluation, leaving 766 restorations to be evaluated soon after placement. The post-operative radiographs taken were evaluated by the chief investigator in accordance with the criteria that had been set [Table 1]. As a result of irregular school attendance, drop-outs, transfers to schools outside the study area and one death, only 648 restorations were clinically evaluated after 2 years using the same criteria.
Table 1.
The clinical evaluation scores for the proximal restorations soon after placement and after 2 years in the study
Calibration of the examiners of the restorations and the radiographs
The chief investigator who had established a ‘gold’ standard with an experienced dentist (Kappa 0.92, n = 20) calibrated the examiners of the restorations. The mean weekly reproducibility for the evaluation of the restoration was Kappa 0.84, n = 63 (for the examiners at the initial evaluation period) and Kappa 0.86, n = 52 (for the examiners after 2 years). Their mean inter-examiner reproducibility was Kappa 0.82 (n = 48) and 0.92 (n = 52 for the two groups respectively, with the intra-examiner agreement range on a re-examination of 10% of the restorations being Kappa 0.80 to 1.0. After calibrating with a local dental radiologist (Kappa, P = 0.88, n = 50), the chief investigator evaluated all the radiographs, and had a mean intra-examiner repeatability of kappa 1.0.
Data analysis
The data was analyzed using SPSS version 14.0 (SPSS Inc., Chicago, IL, USA) computer programme. The results of the survival rate of the proximal restorations were related to the oral hygiene status of the children, the residual caries under the restorations and cervical marginal gaps related to the restorations. The results for the analysis in relation to the method of tooth-isolation and the effects of the operators have been reported in a separate paper.[19,20] Pearson's correlation, Cox Proportional Hazards regression analysis (Cox PH) and Multiple Logistic regression models tests were used to validate the results, with the statistical significance set at less than 5%.
Results
Only 766 children were evaluated soon after placement [Table 1] as remaining 38 children were absent from school and considered truant. At the initial evaluation moment (soon after placement), 94.4% of the restorations had survived (score 0, 1, 6 as shown in Table 1). After 2 years, 648 restorations were available for evaluation and 30.8% of them had survived (see score 0, 1, 6, as shown in Table 1).
Survival of restorations and plaque index
A total of 766 children were validly documented for plaque at baseline, and their mean plaque index was 2.26 (SD 0.46), with 587 (76.6%) having a plaque index of 1.5 or over. More males (n = 332) than females (n = 288) had a plaque index of over 1.5. After two years, the 648 children were evaluated and their mean plaque index was 1.9 (SD 2.1). More males had higher plaque indices than females (Chi-square, P = 0.07). When the plaque indices were grouped as: (a) 0 - 1.5, (b) 1.51 and over, and related to the survival rate of the restorations, the plaque indices of 1.5 and lower were associated with a higher survival rate of the restorations. The difference with those that had plaque index of over 1.5 was, however, not statistically significant (Chi-square, P > 0.5). More males than females recorded higher failure-rate; however, the difference again was also not statistically significant (Chi-square, P = 0.57).
Survival of restorations and radiographic findings
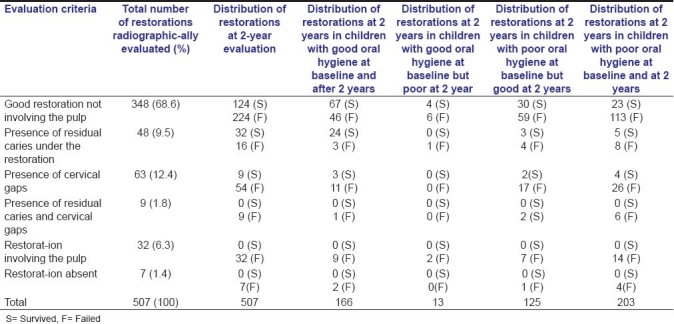
Due to the frequent break-downs of the radiograph machines during the restorative phase and poor quality of some radiographs, in addition to truancy by some of the children, the total number of radiographs were fewer than expected. Only 507 (63.1%) of the possible 804 restorations had good quality radiographs for the study. Nevertheless, this number could be considered to form reasonable representative sample for the study population, allowing for a valid assessment of the possible quality of the restorations and their survival rates. The results of the radiographic assessment are shown in Table 2. Most of the restorations that failed after two years were for children who had a poor oral hygiene status at baseline and after two years. A total of 48 (9.5%) of the 507 restorations had residual caries, and after two years, two-thirds of these restorations (32 or 67%) had survived. The restorations that had residual caries were fewer in children of ages 7 years and older. Most of the restorations that had only marginal gaps at baseline (n = 63) ended up clinically having secondary caries adjacent to them (n = 38), while some of them exfoliated earlier (n = 16), and only a few were still present after two years (n = 9). When the two-year survival rate of the restorations was related to the results of the post-restoration radiographic evaluation [Table 2], there were no statistically significant differences in relation to the survival rate of the restorations that had residual caries and those that didn’t have (Cox PH, Chi-square 19.14, 14 degrees of freedom or df, P = 0.16). The 9 (1.8%) restorations that had both residual caries and gaps had failed at the end of two years. The differences in the two-year survival rate of the restorations with both residual caries and cervical marginal gaps and those with residual caries only and without marginal gaps, was statistically significant (Ch-square, P = 0.003). When the two factors (residual caries and cervical marginal gaps) were related to the operator who placed the restorations, there were almost an equal number of cervical marginal gaps and residual caries present for the restorations placed by six operators. One operator, who apparently had had longer experience with the ART prior to this study, recorded fewer cervical marginal gaps. The difference in the survival of the restorations placed by this particular operator and the other six operators was statistically significant (chi-square, P < 0.05). For all the operators, the restorations placed using rubber dam isolation method had less cervical marginal gaps, and their survival rate was significantly higher when related to those restorations placed using cotton wool roll method (Chi-square, P < 0.05). There was no evidence that the brand of GIC used had any predilection to gap-formation. The plaque indices were again re-categorized into two groups: Indices less than 1.5 representing good oral hygiene and indices above 1.5 for bad oral hygiene. The results were related to the radiographic findings and the survival of the restorations at baseline and after two years [Table 2]. There were more failures for all restorations in children who had plaque indices above 1.5 at baseline and after 2 years, but quite the opposite with the subjects who had plaque indices below 1.5 at both evaluation stages. The difference was, however, not significant statistically (Chi-square, P = 0.06). All the children with both cervical marginal gaps and residual caries did not have any surviving restorations after two years, irrespective of their oral hygiene status. A Pearson correlation test was utilized to relate the survival rate of the restorations to the radiographic findings. The results were as follows: in relation to residual caries X2 = 0.96, 2 df, P = 1.68; cervical marginal gaps Pearson, X2 = 1.47, 3 df, P=0.03; and, both cervical marginal gaps and residual caries Pearson, X2=3.36, 1df, P=0.0024. Multiple regression model tests were used to “adjust” for the effects on the survival rate of the restorations for all these variables in the study (i.e. material brand, method of tooth isolation, operator, assistant, the presence of residual caries, marginal gaps and the oral hygiene status). The results obtained indicated that while the residual caries and oral hygiene did not show any significant effect on the survival rate of the restorations, the restoration-gaps and the method of isolation had a significant effect on the survival rate of the restorations (P < 0.05) irrespective of the other variables in the study. Consequently, in the present study the null hypothesis was not rejected in relation to residual caries and oral hygiene status, but rejected in relation to cervical marginal gaps.
Table 2.
The evaluation criteria and the results of the post-restorative bite-wing radiographs and the oral hygiene of the children in the study
Discussion
In the present longitudinal study, two clinical evaluations of the restorations placed in the primary molars were completed [soon after placement (within 2 hours) and after two years], as well as the post-operative radiographic evaluations were carried out. The clinical evaluation method used in this study has been used in other studies to evaluate ART restorations,[21] and has been found to be simple when compared to the United States Public Health Science (USPH) criteria by Ryge and Snyder.[22] The results of this method have been tested and found to be plausible. Previous studies have reported one-year survival rate of ART restorations in the primary dentition as averaging 75.3% to 100% for single-surface restorations and 42.9% to 93.7% for multi-surface restorations.[23] The 30.8% 2-year survival results in the present study were very low, although other studies have reported much lower results.[24] A total of 5.6% of the proximal restorations in the present study, had failed within the first two hours of placing them, and a few others had lost part of the restoration. This could probably have been due to early restoration-losses, gross marginal failures or failure by the child to abstain from eating within the first one hour.
Influence of oral hygiene on the survival of the restorations
ART approach encompasses good dietary and good oral hygiene habits as part of the important facets of preserving the good health of the dentition.[25] Though not statistically significant, the present study showed poor oral hygiene status and may have resulted in lower survival rate of the restorations. Children who had good oral hygiene at baseline and after two years had higher survival rate of their proximal ART restorations.[26]
Radiographic findings
Previous studies have reported no significant difference in the survival rates of restorations that had residual caries when compared to those without residual caries provided a cavo-material hermetic-seal is present.[7] In the present study, 48 (9.5%) of the restorations had residual caries, 63 (12.5%) had marginal cervical gaps and 9 (1.8%) had both. Any or all of these could have resulted from patient and/or operator-related factors. The two-year cumulative survival of 67% of the restorations with residual caries in the present study could be considered reasonably good (4, 5), when related to results reported by Roeleveld et al.[8] In this study, the presence of residual caries did not also significantly affect the survival rate of the proximal ART restorations. It is to be noted that replacement of the restorations that had residual caries and/or marginal cervical gaps could not be done during the operative stage, as these radiographic results were only found much later when the operative phase of the study had long been completed. The processing of the radiographs was done far away from the study area, and the analysis of the radiographs also took upto months after the placement of the restorations. However, the children who were found to have residual caries and cervical marginal gaps were closely monitored, for any complaint, throughout the study period. Fortunately, none of these children experienced any major complaints with the affected teeth. Most restoration failures have been attributed to marginal leakage arising from poor cavo-material bonding, cracks in the enamel due to restoration setting stress or fracture of the tooth substance at the restoration-cavity interface, probably due to unsupported enamel overhangs and moisture contamination.[26] Additionally, inadequate cavity conditioning, poor mixing of the restorative material and inadequate adhesion of the material to the cavity walls can also lead to gaps and consequently to marginal leakages.[2] The presence of restoration-gaps weakens the restoration and makes it susceptible to early failure.[9] In spite of the operators and their assistants in the present study having been adequately trained and having gained some experience with the technique after training, it is still possible that the above mentioned factors occurred, resulting in the cervical marginal gaps that were observed and the low survival rate of the restorations with both residual caries and gaps.[8] Although the use of caries-detector remains a controversial issue in dental practice,[27] its application in the present study was to help the operator visualize and remove as much of the carious material as possible using the hand instruments. Since the presence of restoration gaps along with residual caries is highly predictive of early restoration failure, adequate tooth-isolation during the placement of a restoration might lead to a reduction in moisture contamination and probably void/gap-formation.[28] It is also possible that poor oral hygiene might worsen the survival rate of the restorations, and more so when the restorations have cervical marginal gaps.
Influence of other possible factors
Due to the similarity in the coefficient of thermal expansion of GIC and the dental hard tissues, good margin adaptation of glass ionomer restorations to the tooth hard-tissues has been cited.[29] However, the material properties can also be influenced by the patient- and operator-related factors. As one operator with a longer experience with ART had less number of restorations with cervical marginal gaps and residual caries, this could suggest that operator experience is a possible influencing factor in survival rate of these restorations.[20]
Conclusions
The survival rate of the proximal ART restorations in the present study was significantly influenced by the presence of cervical marginal gaps related to the restorations, but not with the presence of residual caries under the restorations or the oral hygiene status of the child. However, more conclusive research is needed to evaluate further the effect of the oral hygiene of the child on these restorations.
Acknowledgments
The authors acknowledge the financial and material support from Netherlands Universities’ Foundation for International Cooperation (NUFFIC), GC Europe, 3M ESPE Germany, the University of Nairobi (Deans Committee) and the dedication to the study of the school children, their parents and teachers, ACTA (Dutch) students, the Kenyan doctors, Community Oral Health Officers (COHOs), assistants and the support staff for helping and making this study possible.
Footnotes
Source of Support: Netherlands Universities’ Foundation for International Cooperation, GC Europe, 3M ESPE Germany.
Conflict of Interest: None declared.
References
- 1.Fusayama T. Two layers of carious dentin: Diagnosis and treatment. Oper Dent. 1979;5:63–7. [PubMed] [Google Scholar]
- 2.Fusayama T. Tokyo: Ishiyaku EuroAmerica Inc; 1993. A simple pain-free adhesive restorative system by minimal reduction and total etching; pp. 1–21. [Google Scholar]
- 3.Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry – A review. Int Dent J. 2000;50:1–12. doi: 10.1111/j.1875-595x.2000.tb00540.x. [DOI] [PubMed] [Google Scholar]
- 4.Bönecker M, Grossman E, Cleaton-Jones PE, Parak R. Clinical, histological and microbiological study of hand-excavated carious dentine in extracted permanent teeth. SADJ. 2003;58:273–8. [PubMed] [Google Scholar]
- 5.Mejáre I, Mejáre B, Edwardsson S. Effect of a tight-seal on survival of bacteria in saliva – contaminated cavities filled with composite resin. Endod Dent Traumatol. 1987;3:6–9. doi: 10.1111/j.1600-9657.1987.tb00164.x. [DOI] [PubMed] [Google Scholar]
- 6.Bjørndal L, Larsen T, Thylstrup A. A clinical and microbiological study of deep carious lesions during stepwise excavation using long treatment intervals. Caries Res. 1997;31:411–7. doi: 10.1159/000262431. [DOI] [PubMed] [Google Scholar]
- 7.Kidd EAM. How “clean” must a cavity be before restoration? Caries Res J. 2004;38:305–13. doi: 10.1159/000077770. [DOI] [PubMed] [Google Scholar]
- 8.Roeleveld AC, van Amerongen WE, Mandari GJ. Influence of residual caries and cervical gaps on the survival rate of class II glass ionomer restorations. Eur Arch Paediatr Dent. 2006;7:85–91. doi: 10.1007/BF03320820. [DOI] [PubMed] [Google Scholar]
- 9.Purk JH, Dusevich V, Glaros A, Eick JD. Adhesive analysis of gaps in class II composite resin restorations at the axial and gingival cavity walls restored under in vivo versus in vitro conditions. Dent Mater. 2007;23:871–7. doi: 10.1016/j.dental.2006.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.van’t Hof M, Frencken JE, Wim H, van Palenstein H, Holmgren CJ. The atraumatic restorative treatment (ART) approach for managing dental caries: A meta-analysis. Inter J Dent. 2006;5:345–51. doi: 10.1111/j.1875-595x.2006.tb00339.x. [DOI] [PubMed] [Google Scholar]
- 11.Da Franca C, Colares V, Van Amerongen E. Two-year evaluation of the atraumatic restorative treatment approach in primary molars class I and II restorations. Int I Paediatr Dent. 2011;21:249–53. doi: 10.1111/j.1365-263X.2011.01125.x. [DOI] [PubMed] [Google Scholar]
- 12.de Amorim RG, Leal SC, Frencken JE. Survival of atraumatic restorative treatment (ART) sealants and restorations: A meta-analysis. Clin Oral Investig. 2011;28 doi: 10.1007/s00784-011-0513-3. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Yu C, Gao XJ, Deng DM, Yip HK, Smales RJ. Survival of glass ionomer restorations in primary molars using atraumatic restorative treatment (ART) and conventional cavity preparations: 2-year results. Int Dent J. 2004;54:42–6. doi: 10.1111/j.1875-595x.2004.tb00251.x. [DOI] [PubMed] [Google Scholar]
- 14.Burke JJT, Wilson NH, Cheung SW, Mjör IA. Influence of patient factors on age of restorations at failure and reasons for their placement and replacement. J Dent. 2001;29:317–24. doi: 10.1016/s0300-5712(01)00022-7. [DOI] [PubMed] [Google Scholar]
- 15.Kemoli AM, van Amerongen WE. Influence of the cavity-size on the survival rate of proximal ART restorations in primary molars. Int J Paediatr Dent. 2009;19:423–30. doi: 10.1111/j.1365-263X.2009.01013.x. [DOI] [PubMed] [Google Scholar]
- 16.Greene JC, Vermillion RJ. The simplified oral hygiene index. J Am Dent Assoc. 1964;68:7–13. doi: 10.14219/jada.archive.1964.0034. [DOI] [PubMed] [Google Scholar]
- 17.Landis RJ, Koch CC. The measurement of observed agreement for categorical data. Biometrics. 1997;33:159–74. [PubMed] [Google Scholar]
- 18.Frencken JE, van Amerongen E, Phantumvanit P, Songpaisan Y, Pilot T. 3rd ed. Groningen: WHO Collaborating Centre for Oral Health Services Research; 1997. Manual for Atraumatic Restorative Treatment Approach to control dental caries. [Google Scholar]
- 19.Kemoli AM, van Amerongen WE, Opinya GN. Influence of different isolation methods on the survival of proximal ART restorations in primary molars after two years. Eur Arch Paediatr Dent. 2010;11:132–5. doi: 10.1007/BF03262729. [DOI] [PubMed] [Google Scholar]
- 20.Kemoli AM, van Amerongen WE, Opinya G. Influence of the experience of operator and assistant on the survival rate of proximal ART restorations: Two-year results. Eur Arch Paediatr Dent. 2009;10:227–32. doi: 10.1007/BF03262687. [DOI] [PubMed] [Google Scholar]
- 21.Lo EC, Holmgren CJ, Hu D, van Palenstein Helderman W. Six-year follow up atraumatic restorative treatment restorations placed in Chinese school children. Community Dent Oral Epidemiol. 2007;35:387–92. doi: 10.1111/j.1600-0528.2006.00342.x. [DOI] [PubMed] [Google Scholar]
- 22.Ryge G, Synder M. Evaluating the clinical quality of restorations. J Am Dent Assoc. 1973;87:369–77. doi: 10.14219/jada.archive.1973.0421. [DOI] [PubMed] [Google Scholar]
- 23.Smales RJ, Yip HK. The atraumatic restorative treatment (ART) approach for primary teeth: Review of the literature. Pediatr Dent. 2000;22:294–8. [PubMed] [Google Scholar]
- 24.van Gemert-Schriks MC, van Amerongen WE, ten Cate JM, Aartman IH. Three-year survival of single- and two-surface ART restorations in a high-caries child population. Clin Oral Invest. 2007;11:37–43. doi: 10.1007/s00784-007-0138-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Frencken JE, Holmgren CJ. Basic Package of Oral Care. Nijmegen: WHO Collaborating Centre for Oral Care Planning and Future Scenarios; 2002. van Palenstein- Helderman WHO. [Google Scholar]
- 26.Amerongen WE. Dental caries under glass ionomer. J Public Health Dent. 1996;56:150–4. doi: 10.1111/j.1752-7325.1996.tb02426.x. [DOI] [PubMed] [Google Scholar]
- 27.Al-Sehaibany F, White G, Reiney JT. The use of caries detector to show demineralized dentine. J Clinical Paediatr Dent. 1996;20:293–8. [PubMed] [Google Scholar]
- 28.Williams JH, Billington RW. Changes in compressive strength of glass ionomer restorative materials with respect to the time periods of 24 hours to 4 months. J Oral Rehabil. 2007;18:163–8. doi: 10.1111/j.1365-2842.1991.tb00044.x. [DOI] [PubMed] [Google Scholar]
- 29.Frencken JE, Pilot T, Songpaisan Y, Phantumvanit P. Atraumatic restorative treatment (ART): Rationale, technique, and development. J Public Health Dent. 1996;56:135–40. doi: 10.1111/j.1752-7325.1996.tb02423.x. [DOI] [PubMed] [Google Scholar]