

Abstract
This case report describes the partial pulpotomy treatment of complicated crown fractures of two cases by using white mineral trioxide aggregate (WMTA) with long-term follow-up. In the cases presented here, to injured incisor teeth were open apices and the pulp exposure site was large, so it was decided to perform vital pulpotomy with WMTA. Long-term follow-up examinations revealed that the treatment preserved pulpal vitality with continued root development and apex formation. WMTA may be considered as an alternative option for the treatment of traumatized immature permanent teeth.
Keywords: Complicated crown fracture, partial pulpotomy, white mineral trioxide aggregate
Introduction
The clinical and radiographic findings of traumatic dental injury reveal a loss of tooth structure with pulp exposure, which is commonly referred to in dental literature as complicated crown fracture.[1] Complicated crown fractures represent 18–20% of all traumatic injuries to permanent teeth.[2] The majority of these injuries occur in recently erupted or young permanent teeth that have immature roots.[3]
The treatment planning is influenced by the extent of the exposure of the pulp to the oral environment, the degree of root development and the time interval between the traumatic dental injury and the examination.[4] The treatment strategy of the crown fracture after pulp exposure is dictated by the concern for vitality of the dental pulp for continued root development of immature permanent teeth.[5] Pulp preservation by vital pulp therapy includes pulp capping and pulpotomy in complicated crown fractures of immature permanent incisors. Pulp capping is recommended for small exposure that occurred not more than a few hours previously. As the exposure site was large or the elapsed time was long between the accident and examination, partial pulpotomy was considered as the treatment of choice.[6] Conversely, in mature teeth with closed apex, root canal therapy is recommended due to the extensive loss of tooth structure.[7]
Cvek's vital pulpotomy technique has been used until 1983 with a calcium hydroxide mixture in order to initiate reparative dentin formation by controlling infection and stimulating the wound healing process.[6] In the past decade, mineral trioxide aggregate (MTA) became popular for maintaining the healing of the pulp tissues as it provides good sealing ability, biocompatibility, and low cytotoxicity and also induces odontoblast to form a hard barrier.[8,9] MTA was first described in the dental scientific literature in 1993[10] and was given approval for endodontic use by the US Food and Drug Administration in 1998.[11] Up to 2002, only one MTA material consisting of gray-colored powder was available, and in that year, white mineral trioxide aggregate (WMTA) was introduced as ProRoot MTA (Dentsply Endodontics, Tulsa, OK, USA) to address esthetic concerns.[12] Both formulae contain 75% Portland cement, 20% bismuth oxide, and 5% gypsum by weight.[13,14] However, few clinical studies exist in the dental literature, showing the success of vital pulpotomy by using MTA with long follow-up.
The aim of presenting these case reports is to describe vital pulpotomy treatment with MTA in complicated crown fractures of permanent immature anterior teeth in two cases with long-term follow-up.
Case Reports
Case 1
A 9-year-old boy was referred to the pediatric dentistry clinic with a chief complaint of a trauma that caused fracture in maxillary central incisors by a bicycle accident. His medical history was non-contributory. The clinical examination was performed 2 hours after the accident. The intraoral examination revealed horizontal mid-crown fractures of his maxillary central incisors with pulp exposure. The teeth were not mobile and electronic pulp testing showed vital pulpal responses within normal limits. The teeth were asymptomatic to percussion sensitivity. The radiographic examination revealed that both the teeth had immature apices without any root fracture or periapical radiolucent area [Figure 1a].
Figure 1.
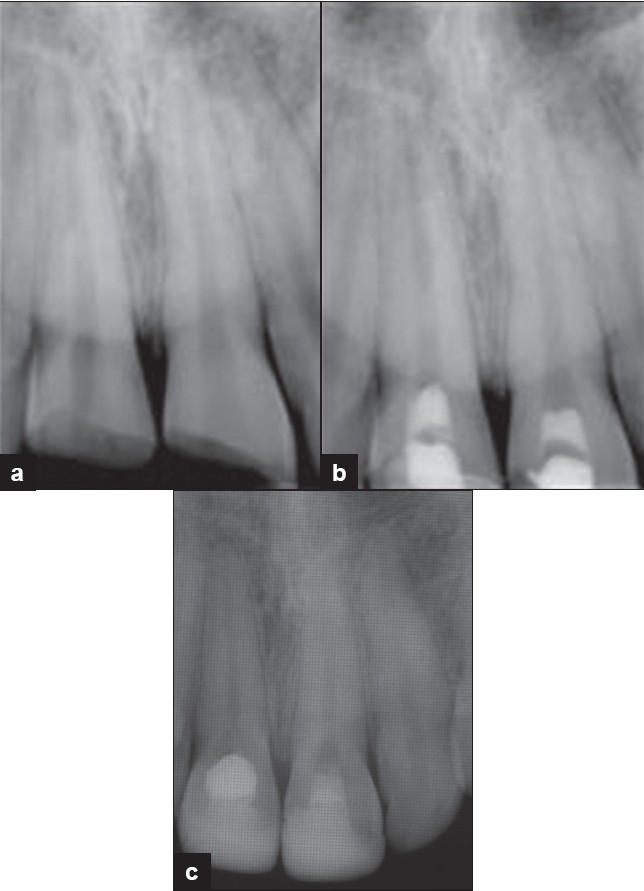
(a) Preoperative radiograph of Case 1; (b) postoperative radiograph of Case 1; (c) 4.5 years follow-up radiograph showing apical root development
A decision was made to perform partial pulpotomies instead of direct pulp capping due to the size of exposure. It was suggested that the teeth should be treated using WMTA (ProRoot, Dentsply, Tulsa Dental, OK, USA) as a partial pulpotomy therapy. Under local anesthesia and rubber dam isolation, the coronal pulp tissues were gently removed to a depth of 2 mm by using a high-speed sterile round diamond bur (Dentsply Maillefer, Tulsa, OK, USA) under water cooling. Hemorrhage was controlled with sterile cotton pellets and sterile saline solution to avoid clot formation. When pulpal bleeding stopped within 3 min, MTA powder was mixed with distilled water according to the recommended consistency and placed without any pressure to cover the exposed pulps. A moist cotton pellet was placed on the MTA and the cavity was sealed temporarily with glass ionomer cement (Fuji IX, GC Corporation, Tokyo, Japan). After 3 days, upper fractured central incisors were reexamined. As the teeth were asymptomatic to percussion sensitivity and gave vital response to electronic pulp test; permanent composite resin restorations (Z250, 3M/ESPE, St. Paul, MN, USA) were achieved [Figure 1b].
The patient was followed for 4.5 years with 3-month examination intervals. During this period, the patient was asymptomatic and electronic pulp tests were within normal limits. The clinical and radiographic evaluations of maxillary central incisors presented no spontaneous pain or discomfort to percussion with evidence of continuing apical root development [Figure 1c].
Case 2
An 8-year-old boy was referred to pediatric dental clinic for the treatment of maxillary left central incisor tooth. The patient reported that he had a schoolyard accident 4 hours ago. His medical history was non-contributory. Extraoral examination revealed no injury. Intraoral examination revealed a complicated crown fracture of the maxillary left central incisor tooth. The tooth was not mobile and gave a vital pulpal response on electronic pulp testing. There was no evidence of traumatic injury to any other teeth or alveolar structures.
Radiographic examination revealed that the maxillary central incisors had open apices and the left maxillary central incisor was fractured. There was no apparent periapical pathosis or alveolar bone fracture [Figure 2a].
Figure 2.
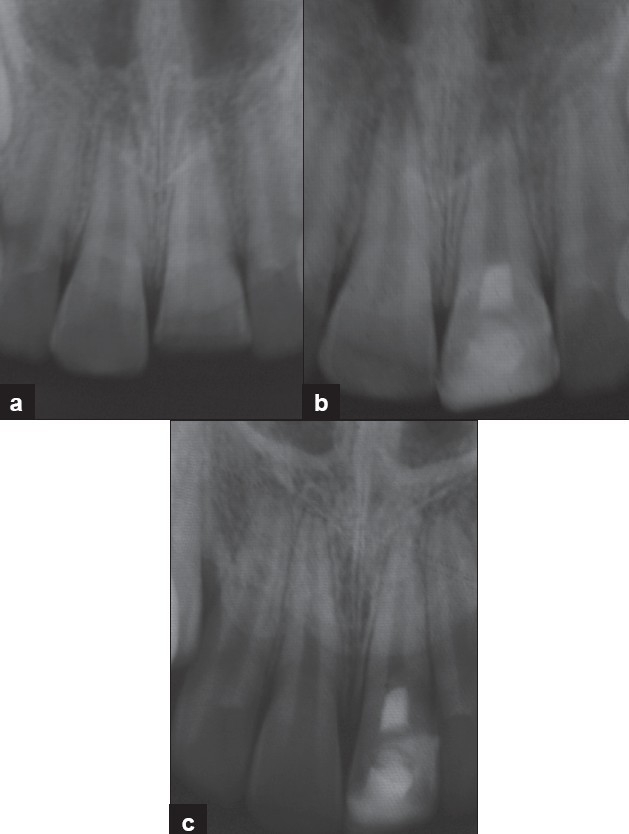
(a) Preoperative radiograph of Case 2; (b) postoperative radiograph of Case 2; (c) 2 years follow-up radiograph showing apical root development with coronal dentin bridge formation
Due to the open apices of the maxillary incisors, it was decided to perform vital partial pulpotomy of maxillary left central incisor with WMTA. The patient and his mother were informed about the advantages and possible complications of the treatment plan. Upon approval of the patient and his parents, the tooth was treated as in Case 1 [Figure 2b].
Careful follow-up examinations were done at 3-month intervals in order to observe the root development of left maxillary central incisor. At the 2-years follow-up examination, no problems were detected and periapical radiograph showed that the apex of the maxillary left central incisor tooth was closed without any sign of pathology, and a dentine bridge was apparent at the pulpotomy site [Figure 2c].
Discussion
In complicated crown fractures, preserving the vital dental pulp or part of it in a healthy state is the main goal in treating young permanent teeth.[15] It was revealed in several studies that inflammation is confined to the surface 2–3 mm of the pulp when traumatically exposed and left untreated for up to 168 hours.[16–18] Therefore, it is universally accepted that vital techniques are recommended for immature teeth.[7]
For many years, calcium hydroxide has been used in vital pulpotomy to cause a coagulation necrosis, inducing a low-grade irritation that leads to differentiation of the undifferentiated pulp cells. These cells synthesize predentine which is subsequently mineralized, while the coagulated tissue is calcified.[19] MTA is one of the materials of choice which has been suggested for use in vital pulpotomy treatment, with a reparation mechanism similar to that of calcium hydroxide. When compared with calcium hydroxide, MTA produces significantly more dentinal bridging in a shorter period of time with significantly less inflammation and also provides a hard-setting, non-resorbable surface without the presence of tunnels in the dentine barrier.[8,9,20] Therefore, in the cases presented here, WMTA was used for the vital pulpotomy treatment.
Many in vivo and histological studies have reported the superior physical and biological properties of MTA in a short follow-up period.[21–25] In the cases presented here, after long-term follow-up periods, injured tooth treated with WMTA pulpotomy showed successful clinical and radiographical outcomes. This result should be attributed to excellent sealing ability of WMTA to prevent microleakage of bacteria and their by-products.
Conclusion
Long-term follow-up of these case reports have shown that vital pulpotomy with WMTA would be a successful treatment choice, showing good long-term prognosis for immature teeth with complicated crown fracture.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Flores MT, Andreasen JO, Bakland LK. Guidelines for the evaluation and management of traumatic dental injuries. Dent Traumatol. 2001;17:1–4. doi: 10.1034/j.1600-9657.2001.170101.x. [DOI] [PubMed] [Google Scholar]
- 2.De Blanco LP. Treatment of crown fractures with pulp exposure. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;82:564–8. doi: 10.1016/s1079-2104(96)80204-6. [DOI] [PubMed] [Google Scholar]
- 3.Webber RT. Apexogenesis versus apexification. Dent Clin North Am. 1984;28:669–97. [PubMed] [Google Scholar]
- 4.Robertson A, Andreasen FM, Andreasen JO, Noren JG. Long term prognosis of crown fractured permanent incisors: The effect of stage of root development and associated luxation injury. Int J Pediatr Dent. 2000;10:191–3. doi: 10.1046/j.1365-263x.2000.00191.x. [DOI] [PubMed] [Google Scholar]
- 5.Flores MT, Andreasen JO, Bakland LK, Feiglin B, Gutmann JL, Oikarinen K, et al. Guidelines for the evaluation and management of traumatic dental injuries (part 3 of the series) Dent Traumatol. 2001;17:97–102. doi: 10.1034/j.1600-9657.2001.017003097.x. [DOI] [PubMed] [Google Scholar]
- 6.Cvek M. Endodontic treatment of traumatized teeth. In: Andreasen JO, editor. Traumatic injuries to the teeth. 2nd ed. Copenhagen: Blackwell Munksgaard; 2003. pp. 321–83. [Google Scholar]
- 7.Andreasen JO, Andreasen FM. Copenhagen: Blackwell Munksgaard; 2008. Textbook and color atlas of traumatic injuries to the teeth. [Google Scholar]
- 8.Ford TR, Torabinejad M, Abedi HR, Bakland LK, Kariyawasam SP. Using mineral trioxide aggregate as a pulp capping mateerial. J Am Dent Assoc. 1996;127:1491–4. doi: 10.14219/jada.archive.1996.0058. [DOI] [PubMed] [Google Scholar]
- 9.Aeinechi M, Eslami B, Ghanbariha M, Saffar AS. Mineral trioxide aggregate and calcium hydroxide as pulp capping agents in human teeth: A preliminary report. Int Endod J. 2003;36:225–31. doi: 10.1046/j.1365-2591.2003.00652.x. [DOI] [PubMed] [Google Scholar]
- 10.Lee SJ, Monsef M, Torabinejad M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J Endod. 1993;19:541–4. doi: 10.1016/S0099-2399(06)81282-3. [DOI] [PubMed] [Google Scholar]
- 11.Schmitt D, Bogen G. Multifaceted use of ProRoot MTA root canal repair material. Pediatr Dent. 2001;23:326–30. [PubMed] [Google Scholar]
- 12.Dammaschke T, Gerth HU, Zuchner H, Schafer E. Chemical and physical surface and bulk material characterization of white ProRoot MTA and two Portland cements. Dent Mater. 2005;21:731–8. doi: 10.1016/j.dental.2005.01.019. [DOI] [PubMed] [Google Scholar]
- 13.Lurgio S. Dentsply, Tulsa Dental. Material safety data sheet (Gray MTA) 2003 [Google Scholar]
- 14.Greenburg J. Dentsply, Tulsa Dental. Material safety data sheet (White MTA) 2002 [Google Scholar]
- 15.ESE. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int Endod J. 2006;39:921–30. doi: 10.1111/j.1365-2591.2006.01180.x. [DOI] [PubMed] [Google Scholar]
- 16.Cvek M, Cleaton-Jones PE, Austin JC, Andreasen JO. Pulp reactions to exposure after experimental crown fracture or grinding in adult monkey. J Endod. 1982;8:391–7. doi: 10.1016/S0099-2399(82)80092-7. [DOI] [PubMed] [Google Scholar]
- 17.Heide S. Pulp reactions to exposure for 4, 24 and 168 hours. J Dent Res. 1980;59:1910. [Google Scholar]
- 18.Heide S, Kerekes K. Delayed partial pulpotomy in permanent incisors of monkeys. Int Endod J. 1986;19:78. doi: 10.1111/j.1365-2591.1987.tb00591.x. [DOI] [PubMed] [Google Scholar]
- 19.Rasmussen P, Mjor IA. Calcium hydroxide as an ectopic bone inductor in rats. Scand J Dent Res. 1971;79:24–30. doi: 10.1111/j.1600-0722.1971.tb01989.x. [DOI] [PubMed] [Google Scholar]
- 20.Trope M, Chivian N, Sigurdsson A, Vann FV., Jr . Traumatic injuries. In: Cohen S, Burns RC, editors. Pathways of the pulp. 8th ed. St. Louis, MO: Mosby; 2002. pp. 603–49. [Google Scholar]
- 21.Holland R, de Souza V, Murata SS, Nery MJ, Bernabé PF, Otoboni Filho JA, et al. Healing process of dog dental pulp after pulpotomy and pulp covering with mineral trioxide aggregate or Portland cement. Braz Dent J. 2001;12:109–13. [PubMed] [Google Scholar]
- 22.Khayat A, Abbasi A, Tanideh N. A comparative study of dentin bridge formation following pulpotomy using calcium hydroxide and mineral trioxide aggregate in young dogs. Ir J Vet Res. 2004;5:47–54. [Google Scholar]
- 23.Karami B, Khayat A, Moazami F, Pardis S, Abbott P. Histological evaluation of the effect of three medicaments: Trichloracetic acid, formocresol and mineral trioxide aggregate on pulpotomised teeth of dogs. Aust Endod J. 2009;35:18–28. doi: 10.1111/j.1747-4477.2007.00112.x. [DOI] [PubMed] [Google Scholar]
- 24.Parolia A, Kundabala M, Rao NN, Acharya SR, Agrawal P, Mohan M, et al. A comparative histological analysis of human pulp following direct pulp capping with Propolis, mineral trioxide aggregate and Dycal. Aust Dent J. 2010;55:59–64. doi: 10.1111/j.1834-7819.2009.01179.x. [DOI] [PubMed] [Google Scholar]
- 25.Nair PN, Duncan TR, Pitt Ford TR, Luder HU. Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: A randomized controlled trial. Int Endod J. 2009;42:422–44. doi: 10.1111/j.1365-2591.2009.01558.x. [DOI] [PubMed] [Google Scholar]