

Abstract
Dentigerous cyst is the most prevalent type of odontogenic cyst and is associated with crown of an unerupted or a developing tooth and accounts more than 24% of jaw cysts. Here, we present an interesting case of dentigerous cyst in a 4-year-old boy, which developed around an unerupted maxillary first premolar. Histological examination revealed a cyst with 1-2-cell-thick epithelial lining and presence of inflammatory cells in the connective tissue.
Keywords: Dentigerous cysts, enucleation, infected primary tooth, odontogenic cyst
Introduction
Kramer has defined cyst as pathological cavity having fluid, semi-fluid, or gaseous contents, and is not created by accumulation of pus.[1,2] Dentigerous cyst is the second most common odontogenic cyst after radicular cyst. They account for approximately 24% of all the true cysts in the jaws.[3,4] Dentigerous cyst is formed by the accumulation of fluid between the reduced enamel epithelium and the crown, with consequent expansion of the tooth follicle, and is characteristically attached to the cervical area of the tooth.[5]
Dentigerous cysts involve impacted, unerupted, permanent teeth, supernumerary teeth, and odontomas, and rarely may involve deciduous teeth.[3] They are more common in second and third decades of life and are rare in the first decade.
The aim of the present article is to report a rare case of dentigerous cyst in a child patient with primary dentition, involving unerupted maxillary first premolar.
Case Report
A 4-year-old boy reported to the Department of Pedodontics and Preventive Dentistry with a chief complaint of painless swelling in the upper jaw from past 15 days.
Extra oral examination revealed the presence of hard and well-defined swelling in the right middle third of the face, approximately 2 cm below the ala tragal line [Figure 1]. On intraoral examination, a firm swelling was found on the upper right region, extending along the buccal vestibule from the first primary molar to the second primary molar. The right maxillary first primary molar was found to be grossly carious with grade III mobility.
Figure 1.

Extraoral swelling
Intraoral periapical (IOPA) radiograph revealed pulp involvement and perforation of floor of the pulp chamber in 54. A well-defined radiolucency measuring 1 × 1 cm around the palatal root was noticed [Figure 2]. Panoramic radiograph [Figure 3] revealed the presence of a large translucent unilocular area with well-defined margins in the maxillary right side and unerupted maxillary premolar and canine. Paranasal sinus (PNS) radiograph [Figure 4] showed canine and premolar pushed into the maxillary space compared to the other side.
Figure 2.

Intraoral periapical radiograph showing radiolucency around the palatal root of 54
Figure 3.

Panoramic radiograph
Figure 4.
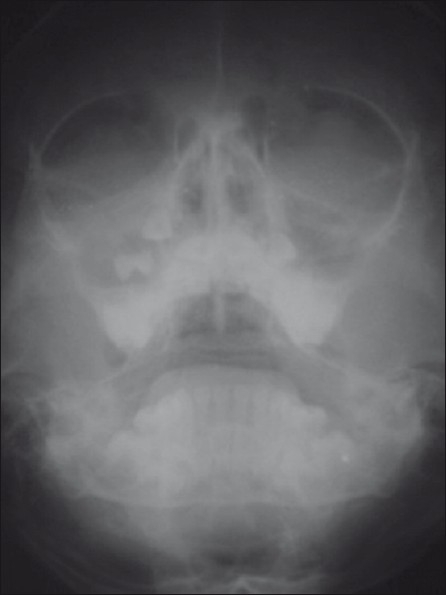
Paranasal sinus radiograph
On the first visit, fine needle aspiration cytology (FNAC) was done and the carious tooth (54) was extracted. The FNAC report was suggestive of cystic aspirate with inflammatory cells. Incisional biopsy was also done and the specimen was sent for histopathologic examination. The cyst was lined by non-keratinized stratified squamous epithelium which was 1–2 cell layer thick with prominent intercellular bridges indicating epithelium derived from reduced enamel epithelium. A definitive diagnosis of dentigerous cyst could be made.
The patient was referred to the Department of Oral Surgery and the opinion from the Department of Pediatrics and Anesthesia was obtained before planning out the procedure under general anesthesia. The necessary blood investigations were carried out. Surgical removal of the cyst (enucleation) was planned under general anesthesia. Crevicular incision was placed from 51 to 55 along with two vertical releasing incisions extending on to the buccal sulcus. The flap was raised using periosteal elevator [Figure 5]. A window in the bone was created and the cystic lining was eased off along with the first premolar with help of curette. Macroscopically the lesion was found attached to the neck of the tooth [Figure 6]. The surgical site was sutured [Figure 7].
Figure 5.
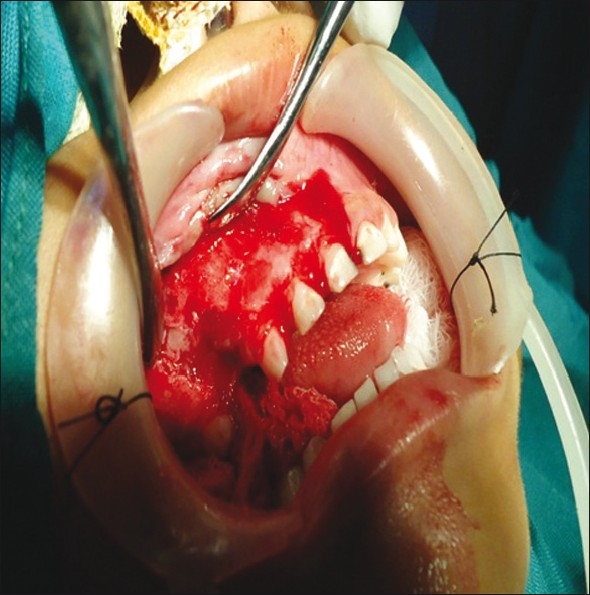
The flap was raised
Figure 6.
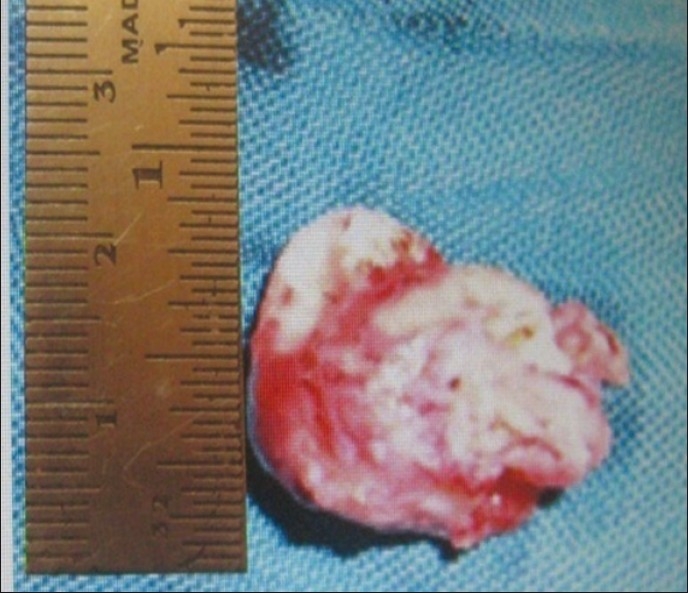
Cystic lesion after enucleation
Figure 7.
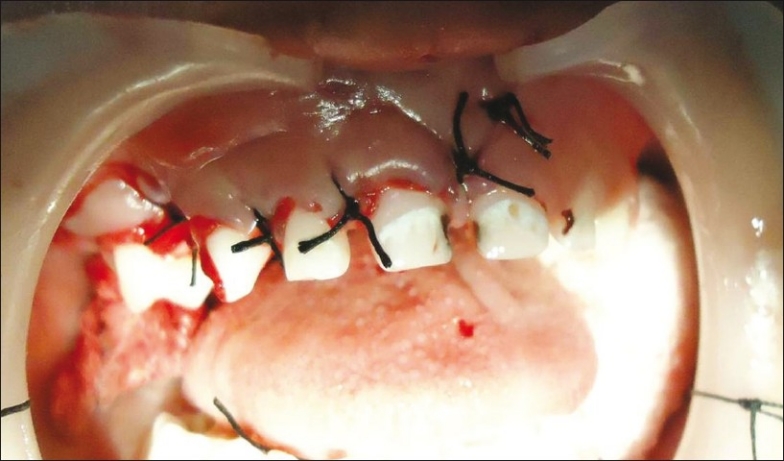
Post-op photograph
The specimen was sent for histopathologic examination and the histopathologic report showed connective tissue stroma which was thick, myxomatous, fibrous, and fibrillar in some areas. The connective tissue was infiltrated with chronic inflammatory cells. Cystic lining showed epithelium of 1–2 cell thickness overlying the connective tissue stroma. The features were suggestive of inflammatory dentigerous cyst [Figure 8].
Figure 8.
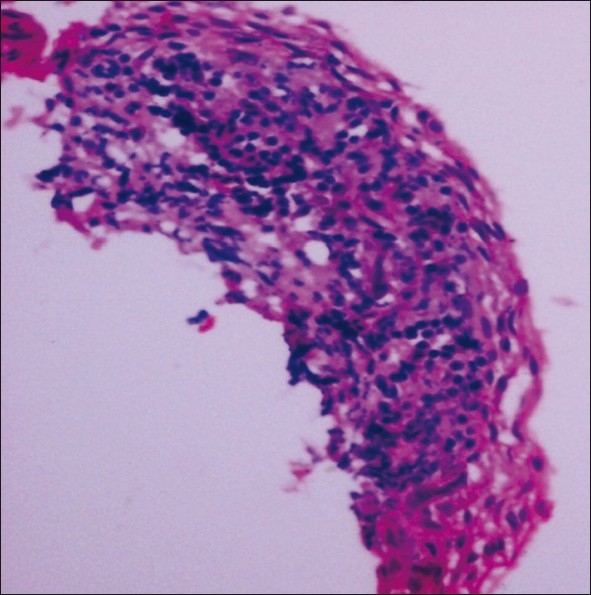
Photomicrograph of dentigerous cyst (H and E, Original magnification ×40)
After one week the patient was recalled for suture removal, the healing of the surgical site was uneventful [Figure 9]. The future treatment protocol decided by the Department of Pedodontics and Preventive Dentistry was periodic recall and review of the patient and posterior tooth replacement. Future treatment can be planned, once all the permanent teeth erupt where either fixed prosthesis or implant can be placed.
Figure 9.

Postoperative after one week
Discussion
Dentigerous cysts are the most common developmental cysts with a frequency of 1.44 per 100 unerupted teeth.[6] Our case is considered to be rare because in the period of primary dentition it is the eruption cyst which is commonly seen and not the dentigerous cyst.[7] Mandibular molar area is the most common site of involvement, whereas if maxilla is involved the anterior region is the most common area.Three radiological variations of the dentigerous cysts are observed:[1] Central variety, circumferential variety, and lateral type. In our case, it was of the central envelopmental variety in which the entire tooth appeared to be enveloped by cyst.
It is very important in diagnosis that a dilated follicle is distinguished from a small dentigerous cyst. While a normal follicular space is 3–4 mm, a dentigerous cyst can be suspected if the space is more than 5 mm.There are two types of dentigerous cysts reported in the literature: developmental and inflammatory types. The developmental type of dentigerous cyst is formed around the crown of an unerupted tooth by accumulation of fluid between the reduced enamel epithelium.[1]
The origin of inflammatory type of dentigerous cyst is thought to be from the overlying non-vital necrotic deciduous tooth.[8] The resultant periapical inflammation spreads to involve the follicle of the unerupted permanent successor; an inflammatory exudate ensues and results in dentigerous cyst formation as seen in our case where the first primary molar on the right side was found to be grossly carious. There are two basic surgical procedures, namely, marsupialization (decompression) and enucleation. Marsupialization, a comparatively simple procedure, consists of surgically producing a “window” in the cystic wall to relieve intracystic tension. The notable disadvantages of the technique are: (a) it is a two-stage surgical procedure; (b) pathological tissue is left behind and a more sinister pathological process (i.e. squamous cell carcinoma) may be overlooked; and (c) in a large cystic cavity, it takes a long period of time for the bone to regenerate.[7]
Enucleation with primary closure was the treatment of choice in our case[9] as the cyst was very small and it was of central variety where the crown was completely enclosed by the cystic lesion. Enucleation without bone grafting was done to the patient because of the smaller diameter of the cyst. Patients with cystic lesions of the jaws following surgery should be followed up through yearly panoramic radiograph, at least up to full bony regeneration of the affected area. Prosthesis to replace the missing tooth is a requirement to prevent over eruption of the opposing tooth or drifting of the adjacent teeth.[10]
Conclusion
Though dentigerous cyst is very uncommon in pediatric patients, we should do thorough investigation to rule out dentigerous cyst when children come with swelling during primary or mixed dentition period, and if possible, the tooth should be saved.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Shear M. Dentigerous cyst. In: Shear M, editor. Cysts of the oral regions. Mumbai: Varghese Publishing House; reprinted in 1996; originally published in 1992. [Google Scholar]
- 2.Kumar N, Devi R, Vanaki S, Puranik RS. Dentigerous Cyst Occurring in Maxilla Associated with Supernumerary Tooth Showing Cholesterol Clefts-A Case Report. Int J Dent Clin. 2010;2:39–4. [Google Scholar]
- 3.Kumar S, Charantimath S, Byakodi R, Shwetha RS. Non syndromic bilateral mandibular dentigerous cysts in a 7 year old child- report of a rare case. Int J Contemp Dent. 2011;2:101–4. [Google Scholar]
- 4.Yamalik K, Bozkaya S, Erkmen E. Non syndromic Bilateral Mandibular Dentigerous Cysts: Report of a Rare Case. Turkiye Klinikleri J Dental Sci. 2007;13:129–34. [Google Scholar]
- 5.Mahajan S, Raj V, Boaz K. Non – Syndromic bilateral dentigerous cysts of mandibular premolars: A rare case and review of literature. Hong Kong Dent J. 2006;3:129–33. [Google Scholar]
- 6.Benn A, Altini M. Dentigerous cyst of inflammatory origin. Oral Surgery Oral Med Oral Pathol Oral Radiol. 1996;81:203. doi: 10.1016/s1079-2104(96)80416-1. [DOI] [PubMed] [Google Scholar]
- 7.Bodner L. Cystic lesions of the jaws in children. Int J Pediatr Otorhinolaryngol. 2002;62:25–9. doi: 10.1016/s0165-5876(01)00583-3. [DOI] [PubMed] [Google Scholar]
- 8.Shaw W, Smith M, Hill F. Inflammatory follicular cysts. ASDC J Dent Child. 1980;47:97–101. [PubMed] [Google Scholar]
- 9.Van Doorm ME. Enucleation and primary closure of jaw cysts. Int J Oral Surg. 1972;1:17–25. doi: 10.1016/s0300-9785(72)80032-2. [DOI] [PubMed] [Google Scholar]
- 10.Mathewson RJ, Primosch RE. Fundamentals Of Pediatric Dentistry. 3rd ed. Missouri: Quintessence Publishing Co; 1995. Prosthodontics; pp. 352–71. [Google Scholar]