

Abstract
Cancer metastases represent the most devastating aspect of malignancy, since the mortality of cancer patients is mainly related to the metastatic behavior of the primary neoplasm. Skin metastases are usually late events in the course of tumor progression. Excluding melanoma, the most common tumor to metastasize to the skin is breast cancer. Patients who develop cutaneous metastases rarely present with a zosteriform distribution. Herein, we present a 60-year-old female, an undiagnosed case of breast cancer, with zosteriform metastases along her right T2-T3 dermatome.
Keywords: Undiagnosed breast cancer, zosteriform metastases, cutaneous metastases
Introduction
Skin metastases have been reported with an increasing frequency ranging from 0.7-10.4% in patients with cancer.[1] Metastasis to the skin is often a preterminal event that heralds poor outcome. However in some cases, skin metastases may be the initial clinical indication of internal, occult or even unknown primary malignancies. As such, the detection of skin metastases requires a high index of clinical suspicion.[2] Excluding malignant melanoma, breast cancer has the highest incidence (23.9%)[3] of cutaneous metastases compared to any other solid malignancy.[3,4] Usually nodular, such metastases rarely present in a zosteriform distribution.[1,2,5] Here, we report one case having an underlying undiagnosed carcinoma breast.
Case Report
A 60-year-old female presented with tender erythematous grouped pseudovesicular papules, arranged in a linear unilateral fashion over the right side of the trunk along the T2-T3 dermatome with mild swelling and erythema of right arm since 15 days. A clinical diagnosis of herpes zoster was made and she was treated with oral acyclovir five times a day for seven days. She reported after 20 days with no change in the cutaneous lesions [Figure 1], aggravated symptoms of the arm, a palpable swelling in the right axilla and tenderness and induration of the right breast. An incisional biopsy of the infiltrated nodule was done that revealed nodular aggregates of the tumor forming glandular structures and solid sheets in the deep dermis, consistent with metastatic adenocarcinoma [Figure 2]. Individual cells appeared pleomorphic with increased nuclear:cytoplasmic ratio [Figure 3]. A provisional diagnosis of cutaneous metastases probably due to breast carcinoma was made. Mammogram followed by cytology of a fine-needle aspirate from the right breast, corroborated the diagnosis of metastatic breast carcinoma. She was then referred to the Oncology department and advised surgical excision combined with chemotherapy.
Figure 1.

Nodular lesions arranged in a segmental unilateral pattern along right T2-T3 dermatome
Figure 2.
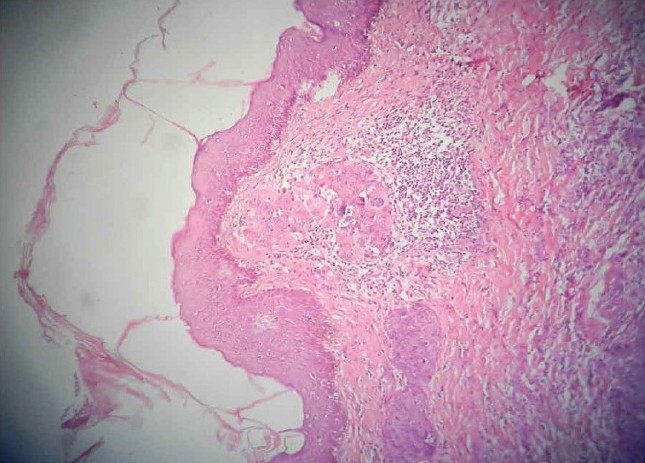
Histopathology; showing malignant cells forming glandular structures and solid sheets in the dermis (H and E stain, ×100)
Figure 3.
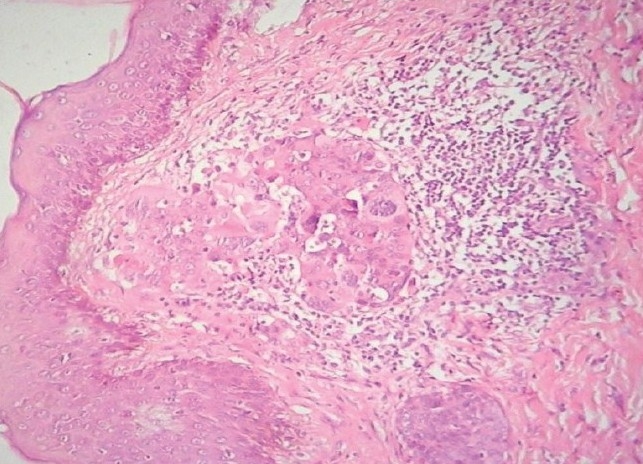
Histopathology view of glandular arrangement of malignant cells with prominent nuclei and nucleoli (H and E stain, ×400)
Discussion
The incidence of cutaneous manifestation in patients with breast carcinoma is 23.9%.[1,3] Cutaneous metastases from breast carcinoma appear within five years after the excision and are usually nodular. Rarely, erysipeloid, telangiectatic, alopecia neoplastica, generalized erythematous patches, eberneum, ‘en cuirase’, erythema annulare centrifugum-like, and bullous zosteriform metastases are reported.[1,2,5] Histologically, these metastases usually show features reminiscent of the primary malignancy, but with variable degrees of differentiation.[2] There are some reports about the coexistence of different clinical manifestations.[6]
Zosteriform metastases are cutaneous metastases, which occur in a dermatomal distribution.[7] To date about a dozen cases of zosteriform metastases due to breast carcinoma have been described in the literature.[1,3,5,8,9] Prior to our case report, we have come across only a solitary such case of cutaneous metastases from an underlying undiagnosed breast carcinoma.[9] The mechanism of zosteriform distribution often remains unknown. However, proposed theories include lymphatic spread, koebnerization at the site of previous zoster infection, surgical implantation of tumor cells and neural spread via the dorsal ganglia. Clinically, metastases localized in the proximity of the underlying internal carcinoma, as in our case, suggest lymphatic spread to the skin.[4,5,7] Cutaneous metastases, especially from adenocarcinoma of the breast are considered as a bad prognostic sign. Also, their prognosis depends primarily on the pathology and biological behavior of the primary neoplasm and its response to treatment.[4]
In conclusion, our patient of zosteriform metastases furnished a clue to the underlying breast carcinoma, which is an extremely rare occurrence.
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1.De Giorgi V, Grazzini M, Alfaioli B, Savarese I, Corciova SA, Guerriero G, et al. Cutaneous manifestations of breast carcinoma. Dermatol Ther. 2010;23:581–9. doi: 10.1111/j.1529-8019.2010.01365.x. [DOI] [PubMed] [Google Scholar]
- 2.Hussein MR. Skin metastasis: A pathologist's perspective. J Cutan Pathol. 2010;37:e1–e20. doi: 10.1111/j.1600-0560.2009.01469.x. [DOI] [PubMed] [Google Scholar]
- 3.Mordenti C, Peris K, Concetta Fargnoli M, Cerroni L, Chimenti S. Cutaneous metastatic breast carcinoma. [Last accessed on 2011 January 28];Acta Dermatovenerol Alp Panonica Adriat. 2000 9:4. Available from: http://www1.mf.uni-lj.si/acta-apa/acta-apa-00-4/mordenti.html . [Google Scholar]
- 4.Prabhu S, Pai SB, Handattu S, Kudur MH, Vasanth V. Cutaneous metastases from carcinoma breast: The common and the rare. Indian J Dermatol Venereol Leprol. 2009;75:499–502. doi: 10.4103/0378-6323.55395. [DOI] [PubMed] [Google Scholar]
- 5.Bassioukas K, Nakuci M, Dimou S, Kanellopoulou M, Alexis I. Zosteriform cutaneous metastases from breast adenocarcinoma. J Eur Acad Dermatol Venereol. 2005;19:593–6. doi: 10.1111/j.1468-3083.2005.01205.x. [DOI] [PubMed] [Google Scholar]
- 6.Gade JN, Kimmick G, Hitchcock MG, McMichael AJ. Generalized cutaneous metastases from breast adenocarcinoma. J Am Acad Dermatol. 1997;37:129–30. doi: 10.1016/s0190-9622(97)70228-7. [DOI] [PubMed] [Google Scholar]
- 7.LeSueur BW, Abraham RJ, DiCaudo DJ, O’Connor WJ. Zosteriform skin metastases. Int J Dermatol. 2004;43:126–8. doi: 10.1111/j.1365-4632.2004.02112.x. [DOI] [PubMed] [Google Scholar]
- 8.Yaghoobi R, Mostoufi NE, Sina N. Zosteriform skin Metastases from breast cancer. Iran J Med Sci. 2003;28:203–5. [Google Scholar]
- 9.Heckmann M, Volkenandt M, Lengye ER, Schirren CG, Gizycki-Nienhaus BV. Cytological diagnosis of zosteriform skin metastases in undiagnosed breast carcinoma. Br J Dermatol. 1996;135:502–3. doi: 10.1111/j.1365-2133.1996.tb01538.x. [DOI] [PubMed] [Google Scholar]