

Abstract
Ovarian reserve plays a crucial role in achieving pregnancy following any treatment in subfertile women. The estimation of ovarian reserve is routinely performed through various ovarian reserve tests (ORTs) in an effort to predict the response and outcome in couples prior to In Vitro Fertilization and counsel them. Most widely used tests are basal follicle stimulating hormone and anti-Mullerian hormone and antral follicle count. The role of ORTs in our routine practice is discussed in this article. A MEDLINE search was done to identify suitable articles for review.
KEY WORDS: Antral follicle count, anti-Mullerian hormone, follicle stimulating hormone, ovarian reserve tests, ovarian reserve
INTRODUCTION
Delayed childbearing, voluntary or involuntary, is a common feature in couples visiting fertility clinics. Majority of the fertility clinics perform ovarian reserve tests (ORTs) as part of the evaluation of women with infertility prior to In Vitro fertilization. Diminishing ovarian reserve is a phenomenon noted in women during mid to late thirties and at times earlier, reflecting the declining follicular pool and oocyte quality.[1] This age-related decline of follicles in the human ovary is believed to more than double when numbers fall below a critical figure of 25,000 at ~37.5 years of age.[2] Assuming fixed time differences between reproductive milestones, fertility will not be lost completely for 4 years, on average, following the onset of this phase.[3]
ORTs provide an indirect estimate of a woman's remaining follicular pool. An ideal ORT should be easy to perform, reproducible, and the decisions based on their results should help differentiate women with a normal and poor ovarian response. This should in turn help identify and counsel couples with negligible chance of conception against any expensive and repeated treatment. However, the availability of multiple ovarian reserve markers suggests that none is ideal. Largely, these tests have been used in subfertile women prior to the first IVF attempt to predict a poor ovarian response. More recently, their value in predicting hyper-response and thus using safe stimulation regimes to prevent OHSS is also explored.[4,5] Their role in the assessment of ovarian reserve in subfertile women not necessarily undergoing IVF or in general population, to identify those at the risk of diminished ovarian reserve, is still poorly understood.
The initial evidence suggested that various ORTs have a good predictive value for pregnancy.[6] However, in the recent years it has been understood that these tests are effective in predicting the ovarian response to stimulation and not for the prediction of pregnancy or its outcome.[7] The interpretation of the results is further complicated by the lack of uniform definitions for poor or hyper-responders and uniform threshold values to identify abnormal results. Biological (age), biochemical, biophysical, and histological tests have been used to identify ovarian reserve [Figure 1].
Figure 1.
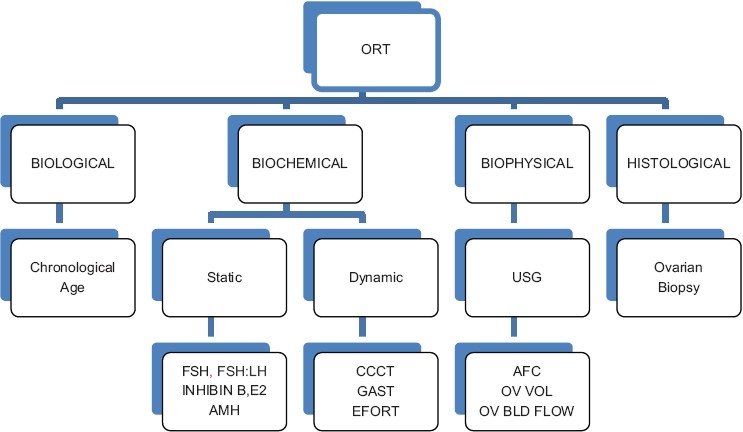
Types of ovarian reserve tests
A literature search was made using the key words “ovarian reserve” and “ovarian reserve tests,” using MEDLINE (1966–2011). A total of 308 articles were found. Further searches were made for individual ORTs using their titles as key words. Appropriate cross-references were manually searched.
Age
It is long established that ovarian reserve reduces progressively with age.[8] Fecundity in both natural and stimulated ovarian cycles declines with maternal age, beginning in the late 20s and becoming more abrupt in the late 30s [Figure 2]. This decline has been observed in population-based studies,[9] and in women undergoing ovulation induction or IVF.[10] Even though fertility does not decline uniformly in women, age is known to be the most important factor determining the pregnancy potential in regularly cycling women.[11–13] However, chronological age alone has a limited value in predicting individual ovarian responses.[14–17] This has led to the development and use of various biochemical and biophysical markers of ovarian reserve.
Figure 2.
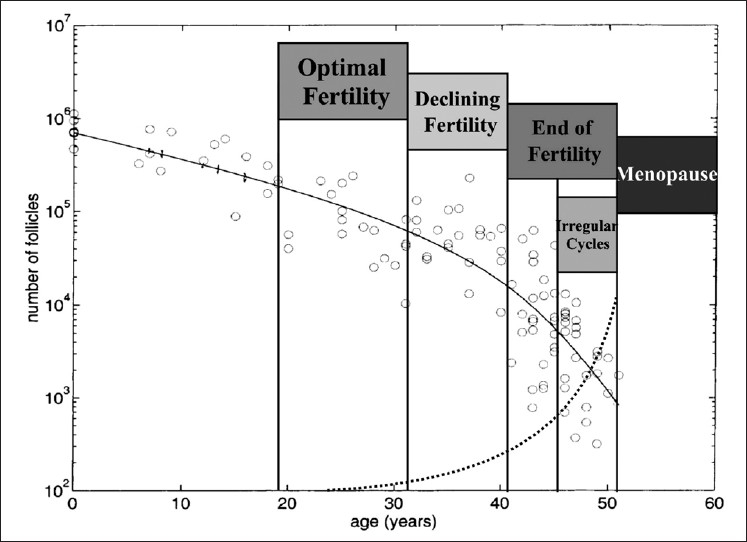
Quantitative (solid line) and qualitative (dotted line) decline of the ovarian follicle pool, which is assumed to dictate the onset of the important reproductive events (reproduced and adapted with permission from[8]).
Basal follicle stimulating hormone
Basal follicle stimulating hormone (FSH) levels measured on day 3 of the menstrual cycle is the most widely used ORT to assess the ovarian response to stimulation, for over two decades now.[14] An increase in FSH levels occurs due to follicle depletion. The measurement of FSH is easy, and inexpensive. However, it is known to have diurnal, intra- and intercycle variability.[18,19] There is no universally accepted cut-off value to identify a poor response. A wide range in threshold values up to 25 IU/L has been used to define abnormal levels of basal FSH. Meta-analysis and systematic reviews have failed to identify any combination of specificity and sensitivity for basal FSH as a test of poor response or prediction of non pregnancy. In regularly cycling women, FSH can predict a poor response adequately only at very high levels, and hence will be helpful only to a small number of women as a screening test, for counselling purposes.[20,21] It is understood that the ovarian aging begins several years before any elevation in FSH levels is noted and hence a normal test cannot rule out a poor ovarian response in some women. Combined with other markers it can be used to counsel couples regarding a poor response but should not be used to exclude regularly cycling women from ART. The usefulness of basal FSH in a general subfertile population or elevated levels in young, regularly cycling women is unclear.[22]
Anti-Mullerian hormone
Anti-Mullerian hormone (AMH) is a dimeric glycoprotein exclusively produced by granulosa cells of preantral (primary and secondary) and small antral follicles (AFs) in the ovary. The production of AMH starts following follicular transition from the primordial to the primary stage, and it continues until the follicles reach the antral stages, with diameters of 2-6 mm.[23–25] The number of the small AFs is related to the size of the primordial follicle pool. With the decrease in the number of the AFs with age, AMH production appears to diminish and become undetectable at and after menopause.[26] AMH levels strongly correlate with basal antral follicle count (AFC) measured by transvaginal ultrasonography.[5] Unlike other biochemical markers, it can be measured on any day of the cycle[27,28] and does not exhibit intercycle variability.[29] Various threshold values, 0.2–1.26 ng/ml, have been used to identify poor responders with 80–87% sensitivity and 64–93% specificity.[30–32] With better understanding of its clinical implications, AMH is now known to have the ability to predict a hyper-response as well.[5,33] The use of nomograms identifies the age-related physiological decline in the AMH levels and thus ovarian reserve, and abnormal deviations can be used for counselling couples wishing to delay childbirth.[34,35] Available evidence does not suggest that serum AMH can be used as a marker to predict pregnancy.[36,37] However, the evaluation of follicular fluid AMH has shown that oocytes obtained from follicles with higher levels of AMH have a better fertility potential compared to those with lower AMH levels.[38]
Longitudinal studies in fertile women have shown a clear decline in AMH levels with age and it is the earliest marker to show a decline longitudinally in young women[39,40] offering the probability of a screening test for women wishing to delay childbirth. It is considered that at levels 0.5–1.26 ng/ml, AMH indicates perimenopausal transition within 3–5 years.[41] Levels within this range still suggest favorable results with ART. Of all the ORTs available, AMH has a unique place in that it may be applicable as a screening test in a general subfertile population.[41]
Inhibin B
Inhibin B is a heterodimeric glycoprotein released by the granulosa cells of the follicle. Women with a low day 3 inhibin B concentration (<45 pg/ml) have a poor response to superovulation for IVF and are less likely to conceive a clinical pregnancy.[42] It is also noted that a decrease in inhibin B probably precedes the increase in the FSH concentration.[43] However, other investigators have failed to show any added predictive value for inhibin B as a measure of ovarian reserve[44,45] and nonoccurrence of pregnancy.[42] At very low threshold levels, the accuracy in the prediction of a poor response and nonpregnancy is only modest[19] and hence its routine use cannot be recommended.
An exaggerated inhibin B response to exogenous FSH ORT has been found to be a predictor of hyper-response in a subsequent cycle.[46]
Basal estradiol
Basal estradiol (E2) has been evaluated as a marker of ovarian reserve in women, prior to IVF. An elevated basal E2 level may mask abnormal FSH levels and hence, FSH levels alone may not be predictable of the ovarian response in such women. Initial studies did show an association between an elevated basal E2 level and a poor ovarian response,[47–49] using different values to define elevated estradiol. A large study showed that a poor ovarian response was more commonly seen in those with <20 or >80 pg/ml of estradiol but did not show any correlation to the pregnancy rate.[50] A meta-analysis concluded that as basal E2 does not add to the predictive value of other commonly used ORTs, its routine use in clinical practice is not recommended.[21]
Clomiphene citrate challenge test
Clomiphene citrate challenge test (CCCT) is a dynamic test involving the administration of 100 mg of clomiphene citrate from the fifth day of the cycle for 5 days. Basal FSH is estimated on day 3 of the cycle and stimulated FSH levels on day 10. Abnormal values on day 3 or day 10, or on addition of the two, is considered as a predictor of a poor ovarian response. However, a meta-analysis has shown that CCCT is no better than basal FSH in predicting a clinical pregnancy.[51] In addition, it has the drawback shared by all dynamic tests in that it is expensive, more invasive, more time consuming, and associated with the possible side effects of administered drugs.[52]
Exogenous follicle stimulating hormone ovarian reserve test
This dynamic test involves the measurement of basal FSH and estradiol followed by the administration of 300 IU FSH on day 3 of the cycle. The serum estradiol concentration is determined 24 h later. It is found to be better than CCCT in predicting hyper-responders and inferior to the latter in predicting a poor response. But, in view of the high rate of false positives, the authors did not recommend this test alone for the identification of hyper-responders.[4]
Gonadotrophin releasing hormone agonist stimulation test
It involves the assessment of serum estradiol on day 2 of the cycle followed by the subcutaneous administration of GnRHa (Triptorelin) 100 μg. A change in estradiol levels is noted by repeating the test 24 h later on day 3. A rise in estradiol is considered to be indicative of good ovarian reserve. It is found to have a good ability for the prediction of poor ovarian reserve but is not superior to inhibin B or AFC in this regard.[53]
ULTRASOUND PARAMETERS
Antral follicle count
AFs are measured by transvaginal ultrasonography in the early follicular phase, by taking the mean of two perpendicular measurements. The numbers of follicles in both ovaries are added for the total AFC. AFC has long been used as a marker of ovarian reserve.[30,40] A count of 8–10 is considered as a predictor of a normal response. Different diameters are used to define AFs – those measuring 2–6 and 7–10 mm. There is no consensus regarding the size of AFs which truly represent ovarian reserve. It is found that the number of AFs 2–6 mm in size declines with age and correlates with other markers such as FSH and CCCT but that of 7–10 mm sized remains constant[54] and hence, the former appears to be a more reliable marker of ovarian reserve. Repeated measurements have shown that there is only a limited intercycle variability.[55] AFC is considered to have the best discriminating potential for a poor ovarian response compared to the total ovarian volume and basal serum levels of FSH, E2, and inhibin B on day 3 of the cycle but lacks the sensitivity and specificity to predict the nonoccurrence of pregnancy.[52,56] More than 14 AFs are considered to be a good predictor of hyper-response.[57] 3D ultrasound does not have any advantage over 2D ultrasound in the assessment of ovarian reserve.[58]
Ovarian volume
The ovarian volume is measured by transvaginal ultrasonography applying the formula for an ellipsoid (D1 × D2 × D3 × π/6). The volume of each ovary is calculated by measuring in three perpendicular directions. The volumes of both ovaries are added for the total basal ovarian volume (BOV). The ovarian volume remains unchanged till the perimenopausal period and does not add to the predictive value of AFC.[56,57] A decline in the ovarian volume is a late event noticed in women >40 years.[59]
Ovarian vascularity
The observation of the ovarian Doppler flow during ovarian stimulation has been studied in IVF cycles. The increase in the Doppler flow noted during stimulation is considered not to provide additional information to AFC.[60]
Ovarian biopsy
Ovarian biopsy done at laparoscopy or laparotomy has shown that the follicular density reduces with age and is correlated with the ovarian volume in women >35 years of age.[61] Also, women with unexplained infertility have fewer follicles than those with tubal factor infertility. However, the distribution of follicles is not uniform within the ovary and hence the biopsy may not represent the true follicular density.[62] It is understood that an invasive ovarian biopsy does not add to the information available through noninvasive modalities and it is not recommended to be used as an ORT.[63]
DISCUSSION
Women in their mid to late 30s and early 40s constitute an important part of the infertile population and many of them require expensive treatments including assisted reproductive technologies. Performing an ORT is an effort toward estimating the primordial follicle pool. It is well understood that the ovarian follicular pool and hence fertility declines with age. However, there is a large individual variation in its onset.[1] The ideal parameter to estimate ovarian reserve would be easily measurable, minimally invasive, inexpensive, and have good predictive value for the outcome being assessed. Majority of the ORTs available are not expensive but need very high threshold levels to identify majority of poor responders.[21] Even though ORTs primarily have been used to identify poor responders, and counsel such women to avoid repeated ineffective treatment, it is now known that some of them are able to predict a hyper-response. This helps avoid maximal ovarian stimulation in such women and minimize the risk of life-threatening OHSS without compromising the pregnancy rate.[33]
Majority of the ORTs, including the most widely used basal FSH levels, show abnormal values late in a woman's reproductive life to be of practical help.[20,21] Abnormal results indicate a much compromised ovarian reserve, implicating that all interventions would be ineffective which is compounded by a huge emotional and financial burden to such couples. Basal E2 and inhibin B are not found to be any better predictive value than FSH. Though FSH induced increase in the inhibin B level may be useful in predicting hyper-response, AMH and AFC are the basal markers found to predict the ovarian response, both poor and hyper, with a high sensitivity and specificity and are comparable in this regard.[5] Serum AMH levels show minimal intra- and intercycle fluctuations and thus can be performed at any stage of the menstrual cycle. They show distinct age-related declines at a very young age, much earlier than other markers including AFC.[40,64] Nomograms have been developed for AMH for infertile women which should help identify those with diminishing ovarian reserve at any given time in the general subfertile population and thus providing an opportunity to counsel couples appropriately regarding reproductive performance. This would also enable them to go through effective modalities of treatment when the chances of achieving a pregnancy are reasonably good.[34,35,65] AMH is the only ORT found to be useful in evaluating the residual ovarian reserve in young women treated for malignancies with chemotherapy or radiotherapy.[66] Dynamic tests do not add to the value of baseline tests and hence cannot be recommended as a diagnostic tool with the available evidence.[67]
Attempts to improve the predictive value of ORTs by using multiple markers instead of single basal marker have not been found to be beneficial.[30,68,69] It is clear from the current evidence that ORTs cannot be used as diagnostic tests for a poor ovarian reserve but should be used as screening tests, and the first IVF attempt remains the diagnostic tool to identify a poor response.[21] AFC and AMH can be used as diagnostic tools to identify hyper-responders and treatment strategy modified accordingly to minimize OHSS.[5,33]
Despite the multitude of ORTs available, age remains the best predictor of pregnancy. A poor predictive value of ORTs in this regard may be due to the fact that chance of pregnancy after IVF depends on many other factors than ovarian reserve alone and that the pregnancy outcome after an ORT is usually assessed in the first IVF cycle alone which may not adequately represent a woman's true reproductive potential.[21]
CONCLUSIONS
ORTs do have a moderate ability to predict poor and hyperresponse.The information can influence the treatment protocol to be chosen for IVF but should not be used to exclude anyone from first attempt at IVF.The present evidence shows that AFC and AMH appear to be the most useful markers of ovarian reserve in addition to chronological age. In addition AMH has the ability to be applied to the general population for identification of diminishing ovarian reserve before it reaches a critical level below which no effective treatment can be offered.This may help women who wish to delay pregnancy to make an informed decision.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared.
REFERENCES
- 1.Scott RT, Hofmann GE. Prognostic assessment of ovarian reserve. FertilSteril. 1995;63:1–11. [PubMed] [Google Scholar]
- 2.Faddy MJ, Gosden RG, Gougeon A, Richardson SJ, Nelson JF. Accelerated disappearance of ovarian follicles in mid-life: implications for forecasting menopause. Hum Reprod. 1992;7:1342–6. doi: 10.1093/oxfordjournals.humrep.a137570. [DOI] [PubMed] [Google Scholar]
- 3.Nikolaou D, Templeton A. Early ovarian ageing: Ahypothesis: Detection and clinical relevance. Hum Reprod. 2003;18:1137–9. doi: 10.1093/humrep/deg245. [DOI] [PubMed] [Google Scholar]
- 4.Kwee J, Schats R, McDonnell J, Schoemaker J, Lambalk CB. The clomiphene citrate challenge test versus the exogenous follicle-stimulating hormone ovarian reserve test as a single test for identification of low responders and hyperresponders to in vitro fertilization. Fertil Steril. 2006;85:1714–22. doi: 10.1016/j.fertnstert.2005.11.053. [DOI] [PubMed] [Google Scholar]
- 5.Broer SL, Dólleman M, Opmeer BC, Fauser BC, Mol BW, Broekmans FJ. AMH and AFC as predictors of excessive response in controlled ovarianhyperstimulation: Ameta-analysis. Hum Reprod Update. 2011;17:46–54. doi: 10.1093/humupd/dmq034. [DOI] [PubMed] [Google Scholar]
- 6.Kahraman S, Vicdan K, Işik AZ, Ozgün OD, Alaybeyoğlu L, Polat G, et al. Clomiphene citrate challenge test in the assessment of ovarian reserve before controlled ovarian hyperstimulation for intracytoplasmic sperm injection. Eur J Obstet Gynecol Reprod Biol. 1997;73:177–82. doi: 10.1016/s0301-2115(97)02742-5. [DOI] [PubMed] [Google Scholar]
- 7.Chuang CC, Chen CD, Chao KH, Chen SU, Ho HN, Yang Y. Age is a better predictor of pregnancy potential than basal follicle-stimulating hormone levels in women undergoing in vitro fertilization. Fertil Steril. 2003;79:63–8. doi: 10.1016/s0015-0282(02)04562-4. [DOI] [PubMed] [Google Scholar]
- 8.de Bruin JP, teVelde ER. Female reproductive ageing: Concepts and consequences. In: Tulandi T, Gosden RG, editors. Preservation of Fertility. London UK: Taylor and Francis; 2004. p. 3. [Google Scholar]
- 9.Wood JW. Fecundity and natural fertility in humans. Oxf Rev Reprod Biol. 1989;11:61–109. [PubMed] [Google Scholar]
- 10.Piette C, de Mouzon J, Bachelot A, Spira A. In-vitro fertilization (influence of woman's age on pregnancy rates) Hum Reprod. 1990;5:56–9. doi: 10.1093/oxfordjournals.humrep.a137041. [DOI] [PubMed] [Google Scholar]
- 11.Padilla SL, Garcia JE. Effect of maternal age and number of in vitro fertilization procedures on pregnancy outcome. Fertil Steril. 1989;52:270–3. doi: 10.1016/s0015-0282(16)60854-3. [DOI] [PubMed] [Google Scholar]
- 12.Seibel MM, Kearnan M, Kiessling A. Parameters that predict success for natural cycle in vitro fertilization-embryo transfer. Fertil Steril. 1995;63:1251–4. doi: 10.1016/s0015-0282(16)57606-7. [DOI] [PubMed] [Google Scholar]
- 13.van Rooij IA, Broekmans FJ, Hunault CC, Scheffer GJ, Eijkemans MJ, de Jong FH, et al. Use of ovarianreservetests for the prediction of ongoing pregnancy in couples with unexplained or mild male infertility. Reprod Biomed Online. 2006;12:182–90. doi: 10.1016/s1472-6483(10)60859-0. [DOI] [PubMed] [Google Scholar]
- 14.Scott RT, Toner JP, Muasher SJ, Oehninger S, Robinson S, Rosenwaks Z. Follicle-stimulating hormone levels on cycle day 3 are predictive of in vitro fertilization outcome. Fertil Steril. 1989;51:651–4. doi: 10.1016/s0015-0282(16)60615-5. [DOI] [PubMed] [Google Scholar]
- 15.Toner JP, Philput CB, Jones GS, Muasher SJ. Basal follicle stimulating hormone level is a better predictor of in vitro fertilization performance than age. Fertil Steril. 1991;55:784–91. doi: 10.1016/s0015-0282(16)54249-6. [DOI] [PubMed] [Google Scholar]
- 16.Sharif K, Elgendy M, Lashen H, Afnan M. Age and basal follicle stimulating hormone as predictors of in vitro fertilization outcome. Br J Obstet Gynaecol. 1998;105:107–12. doi: 10.1111/j.1471-0528.1998.tb09360.x. [DOI] [PubMed] [Google Scholar]
- 17.Erdem M, Erdem A, Gursoy R, Biberoglu K. Comparison of basal and clomiphene citrate induced FSH and inhibin B, ovarian volume and antral follicle counts as ovarian reserve tests and predictors of poor ovarian response in IVF. J Assist Reprod Genet. 2004;21:37–45. doi: 10.1023/B:JARG.0000025936.73125.b4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Scott RT, Jr, Hofmann GE, Oehninger S, Muasher SJ. Intercycle variability of day 3 follicle-stimulating hormone levels and its effect on stimulation quality in in vitro fertilization. FertilSteril. 1990;54:297–302. doi: 10.1016/s0015-0282(16)53707-8. [DOI] [PubMed] [Google Scholar]
- 19.Kwee J, Schats R, McDonnell J, Lambalk CB, Schoemaker J. Intercycle variability of ovarian reserve tests: Results of a prospective randomized study. Hum Reprod. 2004;19:590–5. doi: 10.1093/humrep/deh119. [DOI] [PubMed] [Google Scholar]
- 20.Bancsi LF, Broekmans FJ, Mol BW, Habbema JD, teVelde ER. Performance of basal follicle-stimulating hormone in the prediction of poor ovarian response and failure to become pregnant after in vitro fertilization: Ameta-analysis. Fertil Steril. 2003;79:1091–100. doi: 10.1016/s0015-0282(03)00078-5. [DOI] [PubMed] [Google Scholar]
- 21.Broekmans FJ, Kwee J, Hendriks DJ, Mol BW, Lambalk CB. A systematic review of tests predicting ovarian reserve and IVF outcome. Hum Reprod Update. 2006;12:685–718. doi: 10.1093/humupd/dml034. [DOI] [PubMed] [Google Scholar]
- 22.Esposito MA, Coutifaris C, Barnhart KT. A moderately elevated day 3 FSH concentration has limited predictive value, especially in younger women. Hum Reprod. 2002;17:118–23. doi: 10.1093/humrep/17.1.118. [DOI] [PubMed] [Google Scholar]
- 23.Durlinger AL, Visser JA, Themmen AP. Regulation of ovarian function: The role of anti-Mullerian hormone. Reproduction. 2002;124:601–9. doi: 10.1530/rep.0.1240601. [DOI] [PubMed] [Google Scholar]
- 24.van Rooij IA, Broekmans FJ, teVelde ER, Fauser BC, Bancsi LF, de Jong FH, et al. Serum anti-Müllerian hormone levels: Anovel measure of ovarian reserve. Hum Reprod. 2002;17:3065–71. doi: 10.1093/humrep/17.12.3065. [DOI] [PubMed] [Google Scholar]
- 25.Weenen C, Laven JS, Von Bergh AR, Cranfield M, Groome NP, Visser JA, et al. anti-Müllerian hormone expression pattern in the human ovary: Potential implications for initial and cyclic follicle recruitment. Mol Hum Reprod. 2004;10:77–83. doi: 10.1093/molehr/gah015. [DOI] [PubMed] [Google Scholar]
- 26.de Vet A, Laven JS, de Jong FH, Themmen AP, Fauser BC. anti-Müllerian hormone serum levels: Aputative marker for ovarian aging. Fertil Steril. 2002;77:357–62. doi: 10.1016/s0015-0282(01)02993-4. [DOI] [PubMed] [Google Scholar]
- 27.La Marca A, Stabile G, Artenisio AC, Volpe A. Serum anti-Mullerian hormone throughout the human menstrual cycle. Hum Reprod. 2006;21:3103–7. doi: 10.1093/humrep/del291. [DOI] [PubMed] [Google Scholar]
- 28.Hehenkamp JK, Loomans CW, Themmen AP, de Jong FH, teVelde ER, Broekmans FJ. anti-Mullerian hormone levels in the spontaneous menstrual cycle do not show substantial fluctuation. J ClinEndocrinolMetab. 2006;10:4057–63. doi: 10.1210/jc.2006-0331. [DOI] [PubMed] [Google Scholar]
- 29.Fanchin R, Taieb J, Lozano DH, Ducot B, Frydman R, Bouyer J. Highreproducibility of serum anti-Mullerian hormone measurements suggests a multi-staged follicular secretion and strengthens its role in the assessment of ovarian follicular status. Hum Reprod. 2005;20:923–7. doi: 10.1093/humrep/deh688. [DOI] [PubMed] [Google Scholar]
- 30.Muttukrishna S, McGarrigle H, Wakim R, Khadum I, Ranieri DM, Serhal P. Antral follicle count, anti-Mullerian hormone and inhibin B: Predictors of ovarian response in assisted reproductive technology? BJOG. 2005;112:1384–90. doi: 10.1111/j.1471-0528.2005.00670.x. [DOI] [PubMed] [Google Scholar]
- 31.Tremellen KP, Kolo M, Gilmore A, Lekamge DN. anti-Mullerian hormone as a marker of ovarian reserve. Aust N Z J Obstet Gynaecol. 2005;45:20–4. doi: 10.1111/j.1479-828X.2005.00332.x. [DOI] [PubMed] [Google Scholar]
- 32.La Marca A, Giulini S, Tirelli A, Bertucci E, Marsella T, Xella S, et al. anti-Müllerian hormone measurement on any day of the menstrual cycle strongly predicts ovarian response in assisted reproductive technology. Hum Reprod. 2007;22:766–71. doi: 10.1093/humrep/del421. [DOI] [PubMed] [Google Scholar]
- 33.Nelson SM, Yates RW, Lyall H, Jamieson M, Traynor I, Gaudoin M, et al. anti-Müllerian hormone-based approach to controlled ovarian stimulation for assisted conception. Hum Reprod. 2009;24:867–75. doi: 10.1093/humrep/den480. [DOI] [PubMed] [Google Scholar]
- 34.Nelson SM, Messow MC, McConnachie A, Wallace H, Kelsey T, Fleming R, et al. External validation of nomogram for the decline in serum anti-Müllerian hormone in women: Apopulation study of 15,834 infertility patients. Reprod Biomed Online. 2011;23:204–6. doi: 10.1016/j.rbmo.2011.05.006. [DOI] [PubMed] [Google Scholar]
- 35.Almog B, Shehata F, Suissa S, Holzer H, Shalom-Paz E, La Marca A, et al. Age-related normograms of serum anti-Müllerian hormone levels in a population of infertile women: Amulticenter study. Fertil Steril. 2011;95:2359–63. doi: 10.1016/j.fertnstert.2011.02.057. [DOI] [PubMed] [Google Scholar]
- 36.Peñarrubia J, Fábregues F, Manau D, Creus M, Casals G, Casamitjana R, et al. Basal and stimulation day 5 anti-Mullerian hormone serum concentrations as predictors of ovarian response and pregnancy in assisted reproductive technology cycles stimulated with gonadotropin-releasing hormone agonist–gonadotropin treatment. Hum Reprod. 2005;20:915–22. doi: 10.1093/humrep/deh718. [DOI] [PubMed] [Google Scholar]
- 37.Fiçicioglu C, Kutlu T, Baglam E, Bakacak Z. Early follicular anti-Müllerian hormone as an indicator of ovarian reserve. Fertil Steril. 2006;85:592–6. doi: 10.1016/j.fertnstert.2005.09.019. [DOI] [PubMed] [Google Scholar]
- 38.Fanchin R, Mendez Lozano DH, Frydman N, Gougeon A, di Clemente N, Frydman R, et al. anti-Müllerian hormone concentrations in the follicular fluid of the preovulatory follicle are predictive of the implantation potential of the ensuing embryo obtained by in vitro fertilization. J Clin Endocrinol Metab. 2007;92:1796–802. doi: 10.1210/jc.2006-1053. [DOI] [PubMed] [Google Scholar]
- 39.Van Rooij IA, Tonkelaar I, Broekmans FJ, Looman CW, Scheffer GJ, de Jong FH, et al. anti-Mullerian hormone is a promising predictor for the occurrence of the menopausal transition. Menopause. 2004;11:601–6. doi: 10.1097/01.gme.0000123642.76105.6e. [DOI] [PubMed] [Google Scholar]
- 40.van Rooij IA, Broekmans FJ, Scheffer GJ, Looman CW, Habbema JD, de Jong FH, et al. Serum anti-Müllerian hormone levels best reflect the reproductive decline with age in normal women with proven fertility: A longitudinal study. Fertil Steril. 2005;83:979–87. doi: 10.1016/j.fertnstert.2004.11.029. [DOI] [PubMed] [Google Scholar]
- 41.Gnoth C, Schuring AN, Friol K, Tigges J, Mallmann P, Godehardt E. Relevance of anti-Mullerian hormone measurement in a routine IVF program. Hum Reprod. 2005;23:1359–65. doi: 10.1093/humrep/den108. [DOI] [PubMed] [Google Scholar]
- 42.Seifer DB, Lambert-Messerlian G, Hogan JW, Gardiner AC, Blazar AS, Berk CA, et al. Day 3 serum inhibin-B is predictive of assisted reproductive technologies outcome. Fertil Steril. 1997;67:110–4. doi: 10.1016/s0015-0282(97)81865-1. [DOI] [PubMed] [Google Scholar]
- 43.Seifer DB, Scott RT, Jr, Bergh PA, Abrogast LK, Friedman CI, Mack CK, et al. Women with declining ovarian reserve may demonstrate a decrease in day 3 serum inhibin B before a rise in day 3 follicle-stimulating hormone. Fertil Steril. 1999;72:63–5. doi: 10.1016/s0015-0282(99)00193-4. [DOI] [PubMed] [Google Scholar]
- 44.Corson SL, Gutmann J, Batzer FR, Wallace H, Klein N, Soules MR. Inhibin-B as a test of ovarian reserve for infertile women. Hum Reprod. 1999;14:2818–21. doi: 10.1093/humrep/14.11.2818. [DOI] [PubMed] [Google Scholar]
- 45.Hall JE, Welt CK, Cramer DW. Inhibin A and inhibin B reflect ovarian function in assisted reproduction but are less useful at predicting outcome. Hum Reprod. 1999;14:409–15. doi: 10.1093/humrep/14.2.409. [DOI] [PubMed] [Google Scholar]
- 46.Dzik A, Lambert-Messerlian G, Izzo VM, Soares JB, Pinotti JA, Seifer DB. Inhibin B response to EFORT is associated with the outcome of oocyte retrieval in the subsequent in vitro fertilization cycle. Fertil Steril. 2000;74:1114–7. doi: 10.1016/s0015-0282(00)01627-7. [DOI] [PubMed] [Google Scholar]
- 47.Licciardi FL, Liu HC, Rosenwaks Z. Day 3 estradiol serum concentrations as prognosticators of ovarian stimulation response and pregnancy outcome in patients undergoing in vitro fertilization. Fertil Steril. 1995;64:991–4. doi: 10.1016/s0015-0282(16)57916-3. [DOI] [PubMed] [Google Scholar]
- 48.Smotrich DB, Widra EA, Gindoff PR, Levy MJ, Hall JL, Stillman RJ. Prognostic value of day 3 estradiol on in vitro fertilization outcome. Fertil Steril. 1995;64:1136–40. [PubMed] [Google Scholar]
- 49.Evers JL, Slaats P, Land JA, Dumoulin JC, Dunselman GA. Elevated levels of basal estradiol-17β predict poor response in patients with normal basal levels of follicle-stimulating hormone undergoing in vitro fertilization. Fertil Steril. 1998;69:1010–4. doi: 10.1016/s0015-0282(98)00080-6. [DOI] [PubMed] [Google Scholar]
- 50.Frattarelli JL, Paul A, Bergh PA, Drews MR, Sharara FI, Scott RT., Jr Evaluation of basal estradiol levels in assisted reproductive technology cycles. Fertil Steril. 2000;74:518–24. doi: 10.1016/s0015-0282(00)00693-2. [DOI] [PubMed] [Google Scholar]
- 51.Jain T, Soules MR, Collins JA. Comparison of basal follicle-stimulating hormone versus the clomiphene citrate challenge test for ovarian reserve screening. Fertil Steril. 2004;82:180–5. doi: 10.1016/j.fertnstert.2003.11.045. [DOI] [PubMed] [Google Scholar]
- 52.Maheshwari A, Fowler P, Bhattacharya S. Assessment of ovarian reserve-should we perform tests of ovarian reserve routinely? Hum Reprod. 2006;21:2729–35. doi: 10.1093/humrep/del188. [DOI] [PubMed] [Google Scholar]
- 53.Hendriks DJ, Broekmans FJ, Bancsi LF, Looman CW, de Jong FH, teVelde ER. Single and repeated GnRH agonist stimulation tests compared with basal markers of ovarian reserve in the prediction of outcome in IVF. J Assist Reprod Genet. 2005;22:65–73. doi: 10.1007/s10815-005-1495-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Haadsma MA, Bukman A, Groen H, Roeloffzen EM, Groenewoud ER, Heineman MJ, et al. The number of small antral follicles (2-6 mm) determines the outcome of endocrine ovarian reserve tests in a subfertile population. Hum Reprod. 2007;22:1932–41. doi: 10.1093/humrep/dem081. [DOI] [PubMed] [Google Scholar]
- 55.Bancsi LF, Broekmans FJ, Looman CW, Habbema JD, teVelde ER. Impact of repeated antral follicle counts on the prediction of poor ovarian response in women undergoing in vitro fertilization. Fertil Steril. 2004;81:35–41. doi: 10.1016/j.fertnstert.2003.06.011. [DOI] [PubMed] [Google Scholar]
- 56.Hendriks DJ, Kwee J, Mol BW, teVelde ER, Broekmans FJ. Ultrasonography as a tool for the prediction of outcome in IVF patients: Acomparative meta-analysis of ovarian volume and antral follicle count. Fertil Steril. 2007;87:764–75. doi: 10.1016/j.fertnstert.2006.11.006. [DOI] [PubMed] [Google Scholar]
- 57.Kwee J, Elting ME, Schats R, McDonnell J, Lambalk CB. Ovarian volume and antral follicle count for the prediction of low and hyper responders with in vitro fertilization. Reprod Biol Endocrinol. 2007;5:9. doi: 10.1186/1477-7827-5-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Jayaprakasan K, Hilwah N, Kendall NR, Hopkisson JF, Campbell BK, JohnsonI R, et al. Does 3D ultrasound offer any advantage in the pretreatment assessment of ovarian reserve and prediction of outcome after assisted reproduction treatment? Hum Reprod. 2007;22:1925–31. doi: 10.1093/humrep/dem104. [DOI] [PubMed] [Google Scholar]
- 59.Higgins RV, van Nagell JR, Woods CH, Thompson EA, Kryscio RJ. Interobserver variation in ovarian measurements using transvaginalsonography. Gynecol Oncol. 1990;39:69–71. doi: 10.1016/0090-8258(90)90401-6. [DOI] [PubMed] [Google Scholar]
- 60.Järvelä IY, Sladkevicius P, Kelly S, Ojha K, Campbell S, Nargund G. Quantification of ovarian power Doppler signal with three-dimensional ultrasonography to predict response during in vitro fertilization. Obstet Gynecol. 2003;102:816–22. [PubMed] [Google Scholar]
- 61.Lass A, Silye R, Abrams DC, Krausz T, Hovatta O, Margara R, et al. Follicular density in ovarian biopsy of infertile women: Anovel method to assess ovarian reserve. Hum Reprod. 1997;12:1028–31. doi: 10.1093/humrep/12.5.1028. [DOI] [PubMed] [Google Scholar]
- 62.Schmidt KL, Byskov AG, Andersen AN, Müller J, Andersen CY. Density and distribution of primordial follicles in single pieces of cortex from 21 patients and in individual pieces of cortex from three entire human ovaries. Hum Reprod. 2003;18:1158–64. doi: 10.1093/humrep/deg246. [DOI] [PubMed] [Google Scholar]
- 63.Sharara FI, Scott RT. Assessment of ovarian reserve.Is there still a role for ovarian biopsy? First do no harm! Hum Reprod. 2004;19:470–1. doi: 10.1093/humrep/deh110. [DOI] [PubMed] [Google Scholar]
- 64.Visser JA, de Jong FH, Laven JS, Themmen AP. anti-Müllerian hormone: Anew marker for ovarian function. Reproduction. 2006;131:1–9. doi: 10.1530/rep.1.00529. [DOI] [PubMed] [Google Scholar]
- 65.Nelson SM, Messow MC, Wallace AM, Fleming R, McConnachie A. Nomogram for the decline in serum anti-Müllerian hormone: Apopulation study of 9,601 infertility patients. Fertil Steril. 2011;95:736–41. doi: 10.1016/j.fertnstert.2010.08.022. [DOI] [PubMed] [Google Scholar]
- 66.vanBeek RD, van den Heuvel-Eibrink M, Laven JS, de Jong FH, Themmen AP, Hakvoort-Cammel FG, et al. anti-Mullerian hormone is a sensitive serum marker for gonadal function in women treated for Hodgkin'slymphoma during childhood. J Clin Endocrinol Metab. 2007;92:3869–74. doi: 10.1210/jc.2006-2374. [DOI] [PubMed] [Google Scholar]
- 67.Maheshwari A, Gibreel A, Bhattacharya S, Johnson NP. Dynamic tests of ovarianreserve: Asystematic review of diagnostic accuracy. Reprod Biomed Online. 2009;18:717–34. doi: 10.1016/s1472-6483(10)60019-3. [DOI] [PubMed] [Google Scholar]
- 68.Creus M, Peñarrubia J, Fábregues F, Vidal E, Carmona F, Casamitjana R, et al. Day 3 serum inhibin B and FSH and age as predictors of assisted reproduction treatment outcome. Hum Reprod. 2000;15:2341–6. doi: 10.1093/humrep/15.11.2341. [DOI] [PubMed] [Google Scholar]
- 69.Bancsi LF, Broekmans FJ, Eijkemans MJ, de Jong FH, Habbema JD, teVelde ER. Predictors of poor ovarian response in in vitro fertilization: A prospective study comparing basal markers of ovarian reserve. Fertil Steril. 2002;77:328–36. doi: 10.1016/s0015-0282(01)02983-1. [DOI] [PubMed] [Google Scholar]