

Abstract
Introduction
Abdominal pain is the primary presenting complaint of patients with acute appendicitis. Acute appendicitis presenting as chest pain is extremely rare and according to our search such presentation due to herniation of appendix into thorax through congenital diaphragmatic defect has not yet been reported.
Presentation of case
We present a case of a 12 year old male child who presented with acute chest pain. ECG was suggestive of ischemic changes. Echocardiogram and cardiac enzymes were within normal limits. Chest X-ray and gastrograffin contrast study confirmed the diagnosis of congenital diaphragmatic hernia. On exploration inflamed appendix was found herniated through the diaphragm along with caecum, ascending colon and transverse colon. Histology confirmed the diagnosis of acute appendicitis.
Discussion
Acute appendicitis may sometimes have very varied and rare presentation. In late presenting CDH, the most important factor responsible for acute or chronic presentation seems to be the type of herniated viscera.
Conclusion
This report presents a rare case of late-presenting CDH with herniated appendix along with caecum, ascending colon and transverse colon. Unusual presentation of chest pain was due to an attack of acute appendicitis. Late-presenting CDH is a very intriguing defect with a wide spectrum of clinical manifestations. It should be suspected in cases of unexplained acute or chronic respiratory or gastrointestinal symptoms, and abnormal chest radiographic findings. The prognosis is favorable with correct diagnosis and prompt surgical repair.
Keywords: Acute appendicitis, Congenital diaphragmatic hernia, Chest pain
1. Introduction
Abdominal pain is the primary presenting complaint of patients with acute appendicitis. The diagnostic sequence of colicky central abdominal pain followed by vomiting with migration of the pain to the right iliac fossa was first described by Murphy but may only be present in 50% of patients1.
The appendix may be positioned as preileal, postileal, paracolic, retrocaecal, subcaecal, pelvic and rarely subhepatic2. It is positioned in left iliac fossa in case of situs inversus totalis.
Congenital diaphragmatic hernia (CDH) is a well-known cause of severe respiratory distress in newborns, and is associated with a high mortality rate. There is a milder form of CDH that does not present symptoms until later in life3. Late-presenting CDH is characterized by a wide clinical spectrum. In late-presenting CDH, the most important factor responsible for acute or chronic presentation seems to be the type of herniated viscera3.
2. Presentation of case
A 12 years old male child presented to the emergency department with complaints of acute pain in chest and epigastric region.
Patient had history of 2 episodes of vomiting. There was no history of trauma or previous similar episodes. On examination patient was afebrile, tachycardic, with severe tenderness in epigastrium. Air entry was reduced over left side. Routine investigations were within normal limits except leukocytosis. ECG was suggestive of inferior and anterolateral wall ischemia. Cardiac enzymes and echocardiogram were found to be within normal limits (see Figs. 1–3).
Fig. 1.

Plain radiograph showing distended bowel loops in thorax.
Fig. 2.

Gastrograffin contrast radiograph showing distended bowel loops in thorax.
Fig. 3.
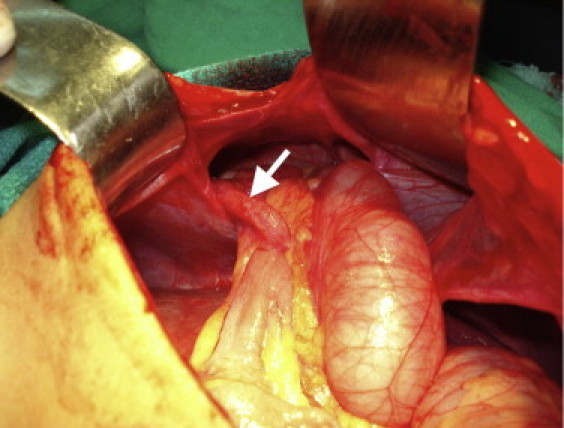
Gross photograph of diaphragmatic defect with herniated appendix.
Chest X ray was suggestive of distended bowel loop in the centre of chest with normal lungs. There was no mediastinal shift. Gastrograffin contrast study was done which confirmed the diagnosis of diaphragmatic hernia located retrosternally.
On exploration a large retrosternal diaphragmatic defect was found slightly towards left with ascending colon, transverse colon, caecum and inflamed appendix herniating through it. Reduction of hernia with appendicectomy, caecopexy and primary closure of the defect was done. On histological examination appendix showed evidence of oedema and congestion with transmural neutrophilic infiltration suggesting acute appendicitis. Post operative period was uneventful.
3. Discussion
Acute appendicitis is one of the most common causes of acute abdomen. Accurate and prompt diagnosis is essential to minimise morbidity as major complications can occur when treatment is delayed.
Although the clinical diagnosis of acute appendicitis may be straightforward for patients who present with classic signs and symptoms, a wide variety of atypical presentations exist that may elude even the most experienced clinicians. Atypical presentation may lead to diagnostic confusion and treatment delay4.
Some rare presentations of acute appendicitis have been described in literature like acute appendicitis presenting as acute left scrotal pain5, distal duodenal obstruction6, perinephric abscesss7, scrotal mass8 etc.
Although a case of acute appendicitis presenting as chest pain due to herniation through radiation induced diaphragmatic defect in an elderly9 has been cited earlier, no case of acute appendicitis presenting as chest pain due to herniation of appendix through congenital diaphragmatic defect has been described in past.
This patient presented with classic signs and symptoms of myocardial ischemia (chest pain, tachycardia, sweating) based on which immediate ECG and echocardiogram were done which were non-contributory. This highlights the difficulty of identifying the primary pathology on the basis of clinical signs alone.
This is a rare case of late-presenting CDH in which the unusual presentation of chest pain was due to an attack of acute appendicitis.
Most cases of late presenting CDH occur in the first few years of life10,11, but cases are reported with some frequency well into adolescence. The outcomes of late-presenting CDH are usually favorable 12 which are related to the absence of accompanying pulmonary hypoplasia and low incidence of other congenital malformations.
Acute presentation may be due to rapid visceral displacement into the chest or rapid distension of previously herniated hollow viscera in most cases. Chronic symptoms result from longstanding compression of the ipsilateral lung. The hernia is best repaired through a transabdominal approach, with excision of the sac and primary closure of the defect in the diaphragm.
4. Conclusion
This report presents a rare case of late-presenting CDH with herniated appendix along with caecum, ascending and transverse colon. Unusual presentation of chest pain was due to an attack of acute appendicitis.
Late-presenting CDH is a very intriguing defect with a wide spectrum of clinical manifestations. It should be suspected in cases of unexplained acute or chronic respiratory or gastrointestinal symptoms, and abnormal chest radiographic findings. The prognosis is favorable with correct diagnosis and prompt surgical repair.
Conflict of interest statement
None.
Funding
None.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
All authors contributed.
References
- 1.Murphy J. Two thousand operations for appendicitis, with deductions from his personal experience. Am J Med Sci. 1904;128:187–211. [Google Scholar]
- 2.O’ Connell P. Ronan. 23rd ed. Arnold Publishers; London, UK: 2000. The vermiform appendix. Bailey and Love's short practice of surgery. p. 1076–92. [Google Scholar]
- 3.Gosche J.R, Islam S., Boulanger S.C. Congenital diaphragmatic hernia: searching for answers. Am J Surg. 2005;190:324–332. doi: 10.1016/j.amjsurg.2005.05.035. [DOI] [PubMed] [Google Scholar]
- 4.Sakalkale R., Reeve P. Portal venous thrombophlebitis in a case of perforated appendicitis: lessons from a case. N Z Med J. 2006;119:U1984. [PubMed] [Google Scholar]
- 5.Stanley A., Wilkins M.D., Jr., Lawrence E., Holder M.D., Rajesh V., Raiker M.D., Theodore H., Wilson M.D., Jr. Acute appendicitis presenting as acute left scrotal pain: diagnostic considerations. Urology. 1985;25(June (6)):634–663. doi: 10.1016/0090-4295(85)90300-0. [DOI] [PubMed] [Google Scholar]
- 6.Chan S.-c., Kwok K.-f., Chu K.-m. Acute appendicitis presenting with distal duodenal obstruction. Surgery. 2003;134(July (1)):105–106. doi: 10.1067/msy.2003.23. [DOI] [PubMed] [Google Scholar]
- 7.Bologna R.A., Khoudary K.P., Danesis G.G., Summers J.L., Porter J.A. Acute appendicitis presenting as a perinephric abscess. J Urol. 1996;156(November (5)):1758. [PubMed] [Google Scholar]
- 8.Alvear D.T., Rayfield M.M. Acute appendicitis presenting as a scrotal mass. J Pediatr Surg. 1976;11(February (1)):91–92. doi: 10.1016/0022-3468(76)90176-7. [DOI] [PubMed] [Google Scholar]
- 9.Schellhaas E., Döbler O., Kroesen A.J., Buhr H.J., Hotz H.G. Gangrenous intrathoracic appendicitis, a rare cause of right-sided chest pain: report of a case. Surg Today. 2010;40(September (9)):874–877. doi: 10.1007/s00595-009-4172-9. [DOI] [PubMed] [Google Scholar]
- 10.Kitano Y., Lally K.P., Lally P.A. Late-presenting congenital diaphragmatic hernia. J Pediatr Surg. 2005;40(12):1839–1843. doi: 10.1016/j.jpedsurg.2005.08.023. [DOI] [PubMed] [Google Scholar]
- 11.Baghaj M. Late-presenting congenital diaphragmatic hernia in children: a clinical spectrum. Pediatr Surg Int. 2004;20:658–669. doi: 10.1007/s00383-004-1269-5. [DOI] [PubMed] [Google Scholar]
- 12.Mei-Zahav M., Solomon M., Trachsel D., Langer J.C. Bochdalek diaphragmatic hernia: not only a neonatal disease. Arch Dis Child. 2003;88(6):532–535. doi: 10.1136/adc.88.6.532. [DOI] [PMC free article] [PubMed] [Google Scholar]