

Abstract
Background
Studies have suggested that nonmaternal care (NMC) may either carry risks or be beneficial for children’s language development. However, few tested the possibility that NMC may be more or less protective for children with different family backgrounds. This study investigates the role of the family environment, as reflected in the socioeconomic status (SES), in the association between NMC in the first year of life and children’s receptive language skills prior to school entry.
Method
A representative sample of 2,297 Canadian children aged between 0 and 11 months at their first assessment was followed over 4 years. Receptive language skills were assessed with the Peabody Picture Vocabulary Test Revised (PPVT-R) when the child was 4 to 5 years old.
Results
After controlling for selection factors, SES was found to moderate the association between NMC and receptive language skills: Full-time NMC in the first year of life was associated with higher PPVT-R scores among children from low SES families (d = .58), but not among children from adequate SES families.
Conclusion
Full-time NMC in infancy may contribute to reducing the cognitive inequalities between children of low and adequate SES.
Keywords: Language development, cognitive development, nonmaternal care, child-care, socioeconomic status, infancy
Over the past two decades, considerable attention has been given to the role of nonmaternal care (NMC) experiences in children’s early cognitive and language development. Studies have suggested that NMC in the first year of life may either carry risks (Waldfogel, Han, & Brooks-Gunn, 2002) or be beneficial for children’s cognitive and language development (Andersson, 1992). Whereas some studies examined the features of NMC that may be related to its protective or detrimental impact, few tested the possibility that NMC may be more or less protective for children with different family backgrounds. For instance, NMC may be particularly beneficial for children who grow up in impoverished home environments. Conversely, NMC may be particularly detrimental for children who would otherwise benefit from an enriched home environment. Furthermore, the extent to which NMC may be beneficial or detrimental for subgroups of children may depend on the amount (e.g., part-time vs. full-time) of the experience.
The general purpose of the present study was to examine the moderating role of socioeconomic status (SES) in the association between NMC in the first year of life and children’s receptive language skills prior to school entry. We refer to nonmaternal care (NMC) as the various forms of non-parental care experienced by preschool children (e.g., daycare centers, family daycare).
The moderating role of SES
Three types of interactions between socioeconomic and child-care contexts have been discussed: a) NMC may compensate for a low SES environment, b) NMC may represent an additional risk for children from a low SES background, or c) NMC may represent a risk for children from an adequate SES family.
The first type of interaction, termed compensatory or protective processes, suggests that a risk factor such as low SES may not lead to negative outcomes when a compensatory experience mitigates the risk. For instance, NMC may be particularly beneficial for low SES children, because NMC might provide cognitive stimulation and opportunities for learning that may not be available in the home. Several studies have shown that children from economically disadvantaged families are at increased risk of developing language problems (Hoff, 2003). This association may come about because children from a disadvantaged background receive less verbal stimulation than other children. For instance, in a naturalistic study, Hart and Risley (1995) showed that the quantity of maternal speech differed as a function of family SES. Specifically, low SES families spent an average of 7 minutes per hour interacting with a child whereas higher SES families spent an average of 42 minutes per hour. To offset the detrimental effects of such early experiences, Hart and Risley (1995) recommended that low SES children experience full-time out-of-home care during the preschool years.
Experimental studies with random assignments such as the Infant Health and Development Program (IHDP) or Abecedarian projects provide convincing evidences that enrolment into early and intensive intervention programs can improve cognitive competence for at-risk children (Burchinal, Campbell, Bryant, Wasik, & Ramey, 1997; McCormick et al., 2006).
Thus, full-time NMC that begins as early as infancy may be particularly beneficial for low SES children. In line with this hypothesis, Caughy, Di-Pietro, and Strobino (1994) showed, with a correlational design, that early entry into full-time NMC was associated with higher reading recognition abilities at 4 or 5 years of age for children from disadvantaged backgrounds. This relation was strongest if participation began before the child’s first birthday.
A second possible interaction, termed multiple risks or risk accumulation, is that instead of being protective, NMC may represent an additional risk for children from already impoverished backgrounds. In line with this argument, Waldfogel and colleagues (2002) reported negative effects of full-time maternal employment (almost synonymous to NMC in that study) in the first year of life on low income children’s PPVT-R and PIAT scores at 4 years.
A third type of interaction is that NMC acts as a risk factor for children from adequate SES families (i.e., lost resource). For instance, by receiving NMC, children from adequate SES families may be deprived of the stimulation and learning opportunities that would be provided by a resourceful parent. In this line, Caughy et al. (1994) reported that maternal employment in the first year of life was associated with lower PPVT-R scores at 4–5 years for children from high income households. However, there are indications that NMC may not be associated with language skills among children from adequate SES families (Erel, Oberman, & Yirmiya, 2000).
Selection into NMC
An important issue in correlational child-care studies has been to account for the selection of children and families into NMC. There is evidence that the extent to which families make use of NMC is influenced by characteristics of the families that also represent risks for children’s development. For instance, children from low SES families are less likely than those from middle or high SES families to receive NMC in toddlerhood (Borge, Rutter, Côté, & Tremblay, 2004). Researchers have discussed other relations with family characteristics and child-care preference such as ethnicity (Early & Burchinal, 2001), maternal education (Singer, Fuller, Keiley, & Wolf, 1998), and family functioning (Borge et al., 2004). If selection factors are not carefully controlled, it may not be possible to separate the effects of child-care from those generated by family factors. In the present study, we tested whether family and child characteristics that are related to receptive language skills influenced the choice of NMC versus MC in the first year of life with the objective of accounting for social selection if it was detected.
Research questions
Two main questions were addressed in this study. First, do family factors influence selection of NMC in the sample? Second, is the (potential) association between NMC and receptive language skills moderated by family SES? In other words, is NMC in the first year of life differentially associated with language skills in children from low SES families as compared to children from adequate SES families?
Method
Participants
The sample was drawn from the National Longitudinal Survey of Children and Youth (NLSCY). The NLSCY conducts biennial assessments of a representative sample of newborns to 11-year-old Canadian children living in private households. In each household, the person most-knowledgeable agent the child (PMKs) (the mothers of households) completed questionnaires that assessed parental and family characteristics along with the child’s physical, cognitive and social development.
The NLSCY comprises several longitudinal and cross-sectional samples, which forms an accelerated longitudinal design. For the first data collection (1994–95: Cycle 1) a sample of 22,831 children were surveyed. Data collections were then undertaken every 2 years (1996–97: Cycle 2; 1998–99: Cycle 3, 2000–01: Cycle 4, etc.) For this study, we selected a cross-section of infants from two cohorts who were between 0 and 11 months of age at the first (n = 1,678), and second (n = 1,415) data collection, resulting in a total sample of 3,093 children. Details about the study can be found in Statistics Canada website (http://www.statcan.ca).
Measures and procedure
Characteristics of the sample on key variables are summarized in Table 1.
Table 1.
Sample characteristics
| Variables | Sample (n = 3,093)
|
Cases in the analyses (n = 2,297)
|
||
|---|---|---|---|---|
| % | n | % | n | |
| Amount of care | ||||
| Maternal care | 75.2 | 2,310 | 75.1 | 1,724 |
| Part-time NMC | 9.8 | 302 | 9.9 | 227 |
| Full-time NMC | 15.0 | 462 | 15.0 | 345 |
| SES | ||||
| Adequate | 75.0 | 2,294 | 77.6 | 1,783 |
| Low | 25.0 | 765 | 22.4 | 514 |
| Sex | ||||
| Male | 51.2 | 1,582 | ||
| Female | 48.8 | 1,511 | ||
| Birth weight | ||||
| Normal | 93.6 | 2,825 | 93.1 | 2,137 |
| Low | 6.4 | 193 | 6.9 | 159 |
| Premature birth | ||||
| Normal range | 89.5 | 2,700 | ||
| Premature | 10.5 | 316 | ||
| Health at birth | ||||
| Good health | 98.2 | 2,883 | ||
| Poor health | 1.8 | 156 | ||
| First language learned | ||||
| English only | 65.6 | 2,018 | 66.0 | 1,517 |
| French only | 21.1 | 648 | 22.9 | 526 |
| French and English | 1.4 | 44 | 1.6 | 36 |
| Others | 11.9 | 365 | 9.5 | 217 |
| Ethnicity | ||||
| Caucasian | 86.5 | 2,490 | ||
| Not Caucasian | 13.5 | 388 | ||
| Working status | ||||
| Not working | 42.9 | 1,088 | ||
| Working | 57.1 | 1,451 | ||
| Breast-feeding | ||||
| Yes | 77.0 | 2,340 | 77.5 | 1,780 |
| No | 23.0 | 698 | 22.5 | 517 |
| Marital status | ||||
| Intact | 89.8 | 2,778 | ||
| Not intact | 10.2 | 315 | ||
| M | SD | M | SD | |
|
|
||||
| PPVT-R | 99.27 | 15.02 | 99.46 | 14.96 |
| Temperament | 8.44 | 5.74 | ||
| Siblings | .86 | .94 | .87 | .92 |
| Family functioning | 7.61 | 5.20 | 7.35 | 5.14 |
| Maternal depression | 4.76 | 4.69 | 4.75 | 4.57 |
| Age in months | 6.16 | 3.02 | 6.19 | 3.02 |
| Maternal age | 29.09 | 5.05 | 29.28 | 4.95 |
| Maternal smoking | 2.11 | 5.09 | 2.10 | 5.09 |
Dependent variable
Receptive language skills
Receptive language skills were measured using the Peabody Picture Vocabulary Test Revised (PPVT-R) (Dunn & Dunn, 1981). The child examined four pictures on an easel and had to identify the picture that matched the word the interviewer read out. It was administered to children aged 55.4 months (SD = 4.5) in either English or French. A French version was developed and normed separately for children who took the test in French (Dunn, Theriault-Whalen, & Dunn, 1993). The internal consistency (Mdn = .82) and test–retest reliability (Mdn = .79) of the instrument are high, and it is correlated with other measures of vocabulary (Dunn & Dunn, 1981). A total raw score was calculated for each child who completed the PPVT-R by computing correct responses. The raw scores were then converted into standardized scores based on age (i.e., M = 100.0, SD = 15.0). The mean PPVT-R scores was slightly higher for children from the second cohort (1996: Cycle 2; M = 100.40, SD = 15.32) than for children from the first cohort (1994: Cycle 1; ) than for children from the first cohort (1994: Cycle 1; M = 98.18, SD = 14.65, t (2,557) = −3.74, ) = −3.74, p < .001). This cohort effect was controlled in the analyses.
Independent variables
Socioeconomic status
SES is a composite measure based on the education (years of schooling) and occupation of the mother and spouse, and household income (Willms & Shields, 1996). Occupation of the mother and spouse (ranging between 0 = lowest and 16 = highest) were based on a schema developed by Pineo, Porter, and McRoberts (1977). Household income was obtained from the total family income and expressed in units of $1,000. Each of the five variables was standardized to have a mean of zero and a standard deviation of one. The SES composite was then calculated by taking the average of the five standardized variables. If one of the five variables had missing data due to non-response (refusal, don’t know, etc.) then the average was taken over the remaining non-missing items. If there was no spouse/partner in the household then the average was taken over the mother-only variables. In this sample, the value for the SES score ranged from −2.72 to 2.82. The SES variable was split at the 25th percentile (−.59) into two groups: 75% adequate SES (coded as 0); 25% low SES (coded as 1). We chose this cut-off point because it represents a risk condition and because it includes a sufficiently large portion of the population to have implication for public policy. In the average low SES family, parents had not completed high school, are unemployed or worked in an unskilled position, and annual household income was approximately 20,000$CAN. In the average high-SES family, the mother had a university degree and the father had a grade 13; the mother was employed as a semi-professional and the father as a semi-skilled clerical worker, and annual household income was approximately 57,000$.
Amount of NMC
Main types of NMC during the first year of life were distributed as follows: care in someone else’s home by a non-relative (39.3%), care in a relative’s home (23.7%), care in the child’s home by a non-relative (12.4%) or relative (14.8%), or care in a day-care center (8.4%). Only 1.4% of children experienced other, non-defined types of NMC. Children spent on average 30.57 (SD = 17.08) hours per week in various types of NMC (ranging between 1 and 120 hours per week). The majority of children did not change care arrangement in the first year (89.8%, n = 690). Amount of care was measured by the number of hours per week in types of care in the first year of life. The variable was split into three categories: MC represented all children cared for at home by their mother; part-time NMC represented children who attended child-care for 1 to 24 hours per week; and full-time NMC represented children who attended child care more than 25 hours per week.
Potential selection factors
Child characteristics
Basic characteristics of the child such as sex, prematurity (child born in normal range or premature, i.e., 258 days or less), birth weight (normal or low, i.e., < 2,500 g), ethnicity (Caucasian or not Caucasian), age of child in months at first assessment, and a proxy of health at birth (i.e., Compared to other babies in general, would you say that your child’s health at birth was: Good or not good?) were examined as potential selection factors. Temperament was assessed with 6 items from the Infant Characteristics Questionnaire (ICQ; Bates, 1987) (e.g., how often fussy per day). High values indicate a difficult temperament. The internal consistency was good (Cronbach’s α was .78). The first language learned at home was represented with dummy variables indicating whether the child first learned English only, French only, French and English or other languages (i.e., neither French nor English).
Household characteristics
The PMKs provided information about the number of siblings from 0 to 18 years of age living in the child’s household. The number of siblings varied between 0 and 9. Family functioning was assessed with twelve items reflecting the quality of family relationship, such as problem solving, communication, roles, affective responsiveness, and behavioral control (Boyle et al., 1987). The scores ranged from 0 to 30 on the scale. A high value indicates a dysfunctional family environment. The internal consistency value for the items of these scales was above .90. The marital status of the family was dichotomized according to whether the family was intact or whether the parents had divorced, separated, remarried, or were widowed.
Maternal characteristics
Mothers reported the frequency of depressive symptoms experienced in the past week. The scale was a short version of the CES-D (Radloff, 1977) and included twelve items scored as 0 (never) to 4 (often). The scores ranged from 0 to 36 (Cronbach’s α = .94). Maternal age varied between 15 and 44 years. The working status of the mother was dichotomized: working or not working. Breast-feeding was represented by a dummy variable indicating whether the mother had or had not breast-fed the child. Maternal smoking during pregnancy was reflected in the number of cigarettes smoked per day. The scores ranged between 0 and 35 cigarettes/day.
Missing data
Approximately 82.7% (n = 2,559) of the 3,093 children had completed data on the receptive language skills measure at age 4–5 years. Complete data for the multivariate model was available for 2,297 children.
Children retained for our analyses (n = 2,297) were compared to excluded children (n = 796). The Bonferroni correction was used for multiple group comparisons (p < .004). The two samples of children were not significantly different on PPVT-R scores and amount of NMC. However, they differed on SES, family functioning, and language first learned. Specifically, as compared to the analysis sample, the excluded sample had larger proportions of low SES children (32.9% vs. 22.4%; χ2 (2) = 34.04, p < .001) and of children whose first language learned was neither French nor English (18.9% vs. 9.5%; χ2 (3) = 60.17, p < .001) and had higher scores on the family dysfunction scale (M = 8.4, SD = 5.31 vs. M = 7.35, SD = 5.14), t (3,036) = 4.80, p < .001). We conducted additional analyses to test whether result would have been different if we had a complete data set (see results section).
Data analysis
The main objective of the analyses was to examine the possibility that the association between amount of NMC in the first year of life and children’s receptive language skills prior to school entry was moderated by the SES of the family. The statistical analyses were conducted in 3 steps.
In the first step, we searched, among 17 child, maternal and household characteristics, the variables that could bias the results by being associated with selection in amount of NMC and the PPVT-R. The variables tested for selection were age of the child in months at first assessment, sex of the child, ethnicity, health of the child at birth, birth weight, premature birth, breast-feeding, maternal smoking during pregnancy, family functioning, family status, working status, language, temperament, maternal age, maternal depression, SES, and number of siblings. First, using chi-squares or t-tests, we identified the variables significantly associated with selection of children into MC and NMC. Second, using correlation (Pearson’s r) or t-tests, we searched among the same set of variables, those significantly associated with language skills. Variables were included as control in the regression models if they were significantly associated with MC/NMC and language skills.
In the second step, we tested the potentially moderating effect of SES in the association between amount of NMC in the first year of life and children’s language skills. Hierarchical multiple regressions analyses were conducted where a) the PPVT-R score was used as dependent variable, and b) SES and amount of NMC, as well as the two-way interactions between those factors, were used as predictors. The models included controls for selection factors.
In the third step, Cohen’s d effect sizes were calculated to describe the differences between NMC versus MC groups in standard deviation units on the receptive language skills outcome (Cohen, 1988). Positive d’s indicate higher PPVT-R scores in the NMC than the MC group while negative d’s indicate lower PPVT-R scores in the NMC group. In all analyses, the longitudinal data were weighted to take into account non-respondents and the stratification design of the NLSCY.
Results
1. Testing for social selection into NMC
With regard to social selection, 10 variables (out of 17) met the selection criterion: 1. age of the child at first assessment; 2. birth weight; 3. breast-feeding; 4. first language learned at home; 5. smoking during pregnancy; 6. maternal depression; 7. maternal age; 8. number of siblings; 9. family functioning; and 10. SES.
Children in MC were younger (M = 5.57 months, SD = 3.02) than children in part-time NMC (M = 7.63 months, SD = 2.43, t(431.68) = −13.44, p < .001) or children in full-time NMC (M = 8.13 months, SD = 2.05, t(911.86) = −22.42, p < .001), and older children had higher PPVT-R scores (r = .06, p = .003).
Low birth weight children were more likely to be in part-time NMC (14.5%) than normal birth weight children (9.6%), χ2 (2) = 6.23, p = .04, and they had a 3.95 points disadvantage on the PPVT-R (M = 95.61, SD = 14.78) as compared with normal birth weight children (M = 99.56, SD = 14.99, t(2,510) = 3.34, p = .001).
Children who were not breastfed were more likely to be in MC (77.4%) than children who were breastfed (74.5%), χ2 (2) = 12.37, p = .002, and they had a 2.91 points disadvantage on the PPVT-R (M = 97.06, SD = 15.29) as compared with those who were breast-fed (M = 99.97, SD = 14.87, t(2,520) = 4.08, p < .001).
Children whose first language learned was neither French nor English were more likely to be in MC (83.0%) (compared with English = 73.0%, French = 77.6%, French and English = 71.1%, χ2 (6) = 26.14, p < .001), and they had lower PPVT-R scores (M = 88.17, SD = 16.28) (compared with English (M = 101.14, SD = 14.20), t(341.36) = −12.38 p < .001, French (M = 99.35, SD = 14.37), t(474.47) = −9.69, p < .001 and French and English (M = 95.40, SD = 15.82) t(309) = −2.61 p = .01).
Children whose mother smoked cigarettes during pregnancy were more likely to be in MC (M = 2.24, SD = 5.28) than children in full-time NMC (M = 1.40, SD = 3.82, t(773.43) = 3.84, p < .001), and they had lower PPVT-R scores (r = −.06, p = .002).
Children in MC had mothers with higher depression scores (M = 4.93, SD = 4.76) than children in full-time NMC (M = 4.21, SD = 4.36, t(693.6) = 3.18, p = .002), and they had lower PPVT-R scores (r = −.08, p < .001).
Children in MC were from younger mothers (M = 28.92, SD = 4.99) than children in full-time NMC (M = 29.71, SD = 5.02, t(2,748) = −3.08, p = .002), and children from older mothers had higher PPVT-R scores (r = .11, p < .001).
Children in MC were from larger families (M = .92, SD = .96) than children in part-time NMC (M = .74, SD = .97, t(2,610) = 3.06, p = .002; or children in full-time NMC (M = .62, SD = .69, t(2,770) = 6.35, p < .001) and they had lower PPVT-R scores (r = −.16, p < .001).
Children in full-time NMC were from more dys-functional families (M = 8.67, SD = 5.38; than children in part-time NMC (M = 7.42, SD = 4.84, t(743) = −3.22, p = .001; or children in MC (M = 7.43, SD = 5.19, t(2,730) = −4.63, p < .001) and they had lower PPVT-R scores (r = −.14, p < .001).
Children from low SES families were more likely to be in MC (83.3%) than those who were not low on SES (72.4%), (χ2 (2) = 38.78, p < .001) and they had a 6.02 points disadvantage on the PPVT-R (M = 94.63, SD = 14.78) compared with children who were not low on SES (M = 100.66, SD = 14.78, t(2,532) = 8.63, p < .001).
2. Does SES moderate the association between amount of NMC and language skills?
The hierarchical regression included 3 steps. First, we entered the selection factors identified previously and the cohort variable. Second, we entered the main effects of the independent variables (SES, and amount of NMC) in order to examine their independent contribution. Finally, we added the two-way interaction between amount of NMC and SES. Table 2 reports the results of the hierarchical multiple regression for each step.
Table 2.
Hierarchical multiple regression testing SES as moderator of the association between amount of NMC and language skills (n = 2,296)
| Model 1
|
Model 2
|
Model 3
|
|||||||
|---|---|---|---|---|---|---|---|---|---|
| B | SE | β | B | SE | β | B | SE | β | |
| Step 1: Control variables | |||||||||
| Cycle | 1.85** | .58 | .06 | 1.88*** | .58 | .06 | 1.90*** | .58 | .06 |
| Age in months | .16 | .1 | .03 | .25* | .10 | .05 | .26* | .10 | .05 |
| Birth weight | −3.08** | 1.16 | −.05 | −2.93* | 1.16 | −.05 | −3.01** | 1.15 | −.05 |
| Language (French) | −1.01 | .74 | −.03 | −1.14 | .73 | −.03 | −1.22 | .73 | −.03 |
| Language (French/English) | −3.84 | 2.34 | −.03 | −4.35 | 2.34 | −.04 | −4.34 | 2.33 | −.04 |
| Language (others) | −13.17*** | 1.02 | −.26 | −12.92*** | 1.03 | −.25 | −13.26*** | 1.03 | −.26 |
| Breast-feeding | −1.69* | .74 | −.05 | −1.78* | .74 | −.05 | −1.73* | .74 | −.05 |
| Maternal age | .47*** | .06 | .16 | .40*** | .07 | .13 | .42*** | .07 | .14 |
| Maternal depression | −.05 | .07 | −.02 | −.03 | .07 | −.01 | −.04 | .07 | −.01 |
| Smoking | −.13* | .06 | −.05 | −.09 | .06 | −.03 | −.09 | .06 | −.03 |
| Family functioning | −.24*** | .06 | −.08 | −.21*** | .06 | −.07 | −.20*** | .06 | −.07 |
| Siblings | −3.02*** | .33 | −.19 | −2.95*** | .34 | −.18 | −2.93*** | .33 | −.18 |
| Step 2: main effects | |||||||||
| SES (low) | −3.20*** | .77 | −.09 | −4.09*** | .83 | −.11 | |||
| Part-time NMC | −1.91 | 1.02 | −.04 | −1.85 | 1.10 | −.04 | |||
| Full-time NMC | −.80 | .88 | −.02 | −2.35* | .94 | −.06 | |||
| Step 3: two-way interaction | |||||||||
| Low SES* part-time | −1.59 | 2.75 | −.01 | ||||||
| Low SES* Full-time | 10.37*** | 2.34 | .10 | ||||||
Note. Δ R2 = .140 for Step 1; Δ R2 = .147 for Step 2; Δ R2 = .155 for Step 3 (ps < .001).
p < .001;
p < .01;
p < .05.
The amount of NMC in the first year of life did not contribute to the prediction of PPVT-R scores after taking the other variables into account. However, the two-way interaction between low SES and full-time NMC significantly predicted PPVT-R scores, indicating that full-time NMC was beneficial for language skills for children from low SES environment. Figure 1 illustrates the interaction effect using non-adjusted PPVT-R means.
Figure 1.
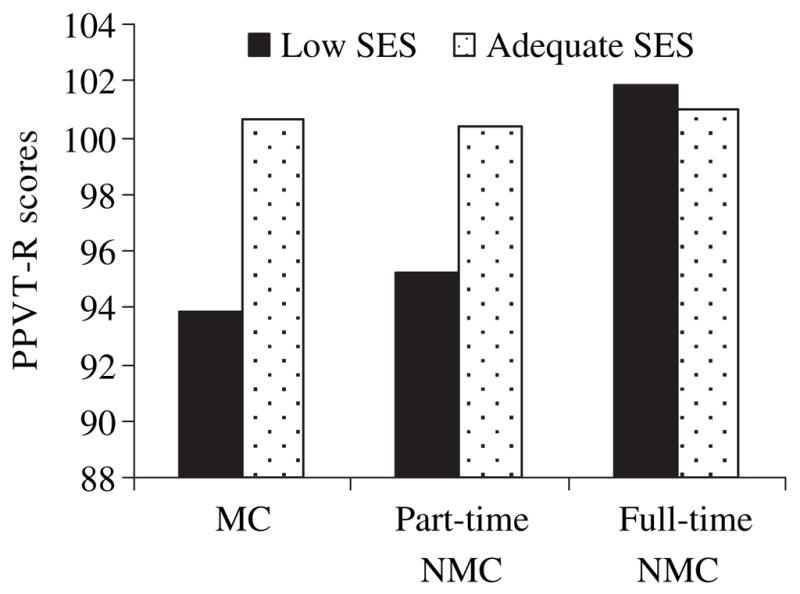
PPVT-R scores according to SES and the amount of NMC in the first year
We used SAS PROC MI to examine whether or not the listwise deleted results were consistent with 10 separate imputed results, i.e., that all 11 datasets were equal in population estimates. The results across the 11 different analyses were equivalent.
3. Effect sizes
The effect sizes, calculated with adjusted means (full-time NMC (M = 104.68, SD = 15.89, N = 46) versus MC (M = 96.47, SD = 14.10, N = 436)), within the low SES children was d = .58, or moderate (Cohen, 1988); Confidence Interval (CI) = .27–.88. The effect sizes, calculated with non-adjusted means (full-time NMC (M = 101.81, SD = 16.62, N = 50) versus MC (M = 93.84, SD = 14.62, N = 490)), within the low SES children was d = .54, or moderate Confidence Interval (CI) = .24–.83.
Discussion
The objective of the study was to examine the moderating role of the SES in the association between NMC in the first year of life and children’s receptive language skill prior to school entry among a large and nationally representative sample. In order to do so, it was essential to examine whether social selection factors were operating with regard to the children receiving or not receiving nonmaternal care. Ten selection factors were identified (SES, family functioning, maternal depression, maternal age, language first learned, siblings, birth weight, breastfeeding, smoking during pregnancy, and age of the child at first data collection) and controlled in the multivariate analyses.
The most important finding concerns the differential effects of NMC on children’s receptive language skills for children from adequate and low SES families. Full-time NMC operated in opposite directions according the presence or absence of a family risk. Among children from low SES family, the compensatory/protective processes hypothesis was supported, suggesting that NMC acts as a protective factor. After controlling for various selection factors, full-time NMC in the first year of life was associated with an advantage of 8.21 standardized points on the PPVT-R (as compared with low SES children in MC). The beneficial effect of NMC for low SES children observed in the present study is consistent with previous longitudinal studies showing that NMC experiences might compensate for limited resources at home (Caughy et al., 1994). Among adequate SES children, full-time NMC was not associated with PPVT-R scores, suggesting that NMC had a neutral effect when the home environment was adequate.
Strengths and limitations
This study offers some strong methodological features such as a large sample size, representative sample, longitudinal data from early infancy, replication of the key finding on two cohorts of children, and statistical control for possible confounding factors. Accordingly, the findings are likely to be generalizable to other populations within certain constraints.
However, there are also limitations. First, there were no measures of quality of NMC provided in the NLSCY, and it cannot be assumed that the findings will generalize to populations where the quality of NMC differs from that available in Canada. But, note that the mean level quality of NMC services in Canada (Goelman, Doherty, Lero, LaGrange, & Tougas, 2000; Japel, Côté & Tremblay, 2005) is similar to that of several other industrialized countries (i.e., United States, Germany, Portugal, & Spain) (Cryer, Tietze, Burchinal, Leal, & Palacios, 1999; Vandell & Wolfe, 2000). There is also evidence, in Canada as in the US, that children from less advantaged backgrounds are less likely to receive NMC, and that when they do, the services they receive tend to be of poorer quality (Japel et al., 2005; NICHD ECCRN, 2006).This suggests that the beneficial effect of NMC for low SES children could be more pronounced if the quality of NMC services was taken into account. Future studies examining the impact of the quality of community-wide NMC services among low SES children are needed to examine this possibility.
Second, the main NMC arrangement selected by the parents of this sample was out-of-home family care. Because of the small sample size within the low SES segment of the sample, it was not possible to test whether the protective effect varied as a function of the type of NMC. Future studies are needed in order to test the possibility that other types of NMC services, such as center-based care, can have a similar protective effect.
Third, in our representative Canadian sample, only 28.5% of families use some form of NMC for their infant. This is in sharp contrast with data from the US indicating that 80% of families use some form of NMC in the first year of life (NICHD ECCRN, 2006). This discrepancy may come about because of the Canadian parental leave program. Most Canadian mothers have 6 to 12 months paid parental leave at the birth of a child, which makes MC a very common choice (71.5% in our sample). Because infants who received NMC may be from more privileged families, it was necessary to consider whether the interaction could be an artifact of social selection on the family’s choice of NMC or MC. This possibility seems not plausible, because the significant moderating effect of SES applied after taking account of possible confounding variables. However, there is still possibility that the interaction effect reflects some unmeasured variables, such as quality of care.
Finally, there were significant differences between children who were included in the multivariate model and those who were not. For example, there was a higher proportion of low SES children among the participants who were not included in multi-variate model due to missing data. However, we used SAS PROC MI to test whether results would have been different if we had a complete data set. The imputed data set showed that the missing data do not significantly affect the results.
Implications for social policy
The protective role of NMC in the first year of life for high-risk children was previously demonstrated experimentally (Campbell, Ramey, Pungello, Sparling, & Miller-Johnson, 2002). But, our findings are novel in that they highlight the protective role of community-based child-care services for low SES children. Accordingly, our findings may be relevant for social policy programs. Thus, we highlighted the fact that policy programs should facilitate NMC services accessibility for at-risk children. In our representative sample, there were inequalities in NMC utilization indicating that low SES children were less likely to receive NMC. In Canada, employed families with low income are eligible to subsidies which may reduce the cost of child care. However, despite such subsidies programs, there is a relatively high proportion of low SES infants who remain in MC. This may come about because there are no child-care subsidies for the most vulnerable children: those whose mothers or fathers are unemployed. Policy programs should target the more vulnerable children and design child-care services better adapted to their special needs.
Acknowledgments
This study was made possible by research fellowships to MCG from the Social Sciences and Humanities Research Council and the Quebec Inter-University Centre for Social Statistics, by research scientist awards to SMC from the Canadian Institutes for Health Research (CIHR) and to JRS from the Fonds de Recherche en Sante du Québec (FRSO), by CIHR grant #79420 to SMC and JRS and SSHRC (Social Science and Humanities Research Council of Canada) grant to SMC, by the Ste-Justine Hospital Research Centre, and by the Research Unit on Childhood Psychosocial Maladjustment.
Abbreviations
- NMC
nonmaternal care
- SES
socioeconomic status
- PPVT-R
Peabody Picture Vocabulary Test Revised
References
- Andersson BE. Effects of day-care on cognitive and socioemotional competence of thirteen-year-old Swedish schoolchildren. Child Development. 1992;63:20–36. [Google Scholar]
- Bates JE. Temperament in infancy. In: Osofsky J, editor. Handbook of infant development. 2. New York: Wiley; 1987. pp. 1101–1149. [Google Scholar]
- Borge AIH, Rutter M, Côté S, Tremblay RE. Early childcare and physical aggression: Differentiating social selection and social causation. Journal of Child Psychology and Psychiatry. 2004;45:367–376. doi: 10.1111/j.1469-7610.2004.00227.x. [DOI] [PubMed] [Google Scholar]
- Boyle MH, Offord DR, Hofmann HG, Catlin GP, Byles JA, Cadman DT, et al. Ontario Child Health Study: I. Methodology. Archives of General Psychiatry. 1987;44:826–831. doi: 10.1001/archpsyc.1987.01800210078012. [DOI] [PubMed] [Google Scholar]
- Burchinal MR, Campbell FA, Bryant DM, Wasik BH, Ramey CT. Early intervention and mediating processes in cognitive performance of children of low-income African American families. Child Development. 1997;68:935–954. doi: 10.1111/j.1467-8624.1997.tb01972.x. [DOI] [PubMed] [Google Scholar]
- Campbell FA, Ramey CT, Pungello E, Sparling J, Miller-Johnson S. Early childhood education: Young adult outcomes from the Abecedarian Project. Applied Developmental Science. 2002;6:42–57. [Google Scholar]
- Caughy MOB, DiPietro JA, Strobino DM. Day-care participation as a protective factor in the cognitive development of low-income children. Child Development. 1994;65:457–471. [PubMed] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2. Hillsdale, NJ: Erlbaum; 1988. [Google Scholar]
- Cryer D, Tietze W, Burchinal M, Leal T, Palacios J. Predicting process quality from structural quality in preschool programs: A cross-country comparison. Early Childhood Research Quarterly. 1999;14:339–361. [Google Scholar]
- Dunn LM, Dunn LM. Peabody Picture Vocabulary Test-Revised (PPVT-R) Circles Pines, MN: American Guidance Services; 1981. [Google Scholar]
- Dunn LM, Theriault-Whalen CM, Dunn LM. Manuel pour les formes A et B. Toronto, ON: Psycan; 1993. Échelle de Vocabulaire en Images Peabody. Adaptation française du Peabody Picture Vocabulary Test-Revised. [Google Scholar]
- Early DM, Burchinal MR. Early childhood care: Relations with family characteristics and preferred care characteristics. Early Childhood Research Quarterly. 2001;16:475–497. [Google Scholar]
- Erel O, Oberman Y, Yirmiya N. Maternal versus nonmaternal care and seven domains of children’s development. Psychological Bulletin. 2000;126:727–747. doi: 10.1037/0033-2909.126.5.727. [DOI] [PubMed] [Google Scholar]
- Goelman H, Doherty G, Lero DS, LaGrange A, Tougas J. Caring and learning environments: Quality in child care centres across Canada. You bet I care! Guelph, ON: Centre for Families, Work and Well-Being, University of Guelph; 2000. (ERIC Document Reproduction Service No. ED453904) [Google Scholar]
- Hart B, Risley TR. Meaningful differences in the everyday experience of young American children. Baltimore, MD: Paul H. Brookes; 1995. [Google Scholar]
- Hoff E. The specificity of environmental influence: Socioeconomic status affects early vocabulary development via maternal speech. Child Development. 2003;74:1368–1378. doi: 10.1111/1467-8624.00612. [DOI] [PubMed] [Google Scholar]
- Japel C, Côté S, Tremblay R. Quality counts! Assessing the quality of daycare services based on the Quebec Longitudinal Study of Child Development. Montréal, QC: Institute for Research on Public Policy; 2005. [Google Scholar]
- McCormick MC, Brooks-Gunn J, Buka SL, Goldman J, Yu J, Salganik M, et al. Early intervention in low birth weight premature infants: Results at 18 years of age for the Infant Health and Development Program. [see comment] Pediatrics. 2006;117:771–780. doi: 10.1542/peds.2005-1316. [DOI] [PubMed] [Google Scholar]
- NICHD ECCRN. Child-care effect sizes for the NICHD study of early child care and youth development. American Psychologist. 2006;61:99–116. doi: 10.1037/0003-066X.61.2.99. [DOI] [PubMed] [Google Scholar]
- Pineo PC, Porter J, McRoberts HA. The 1971 Census and the socioeconomic classification of occupations. Canadian Review of Sociology and Anthropology. 1977;14:91–102. [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Singer JD, Fuller B, Keiley MK, Wolf A. Early child-care selection: Variation by geographic location, maternal characteristics, and family structure. Developmental Psychology. 1998;34:1129–1144. doi: 10.1037//0012-1649.34.5.1129. [DOI] [PubMed] [Google Scholar]
- Vandell DL, Wolfe B. Child care quality: Does it matter and does it need to be improved? Madison, WI: Institute for Research on Poverty, Wisconsin University; 2000. (ERIC Document Reproduction Service No. ED 441941) [Google Scholar]
- Waldfogel J, Han WJ, Brooks-Gunn J. The effects of early maternal employment on child cognitive development. Demography. 2002;39:369–392. doi: 10.1353/dem.2002.0021. [DOI] [PubMed] [Google Scholar]
- Willms DJ, Shields M. A measure of socioeconomic status for the National Longitudinal Study of Children. 9607. Fredericton, NB: Atlantic Center for Policy Research in Education, University of New Brunswick and Statistics Canada; 1996. [Google Scholar]