

Abstract
Objective:
To evaluate the depth of penetration of three resin-based root canal sealers into the dentinal tubules at the cervical, middle and apical third of the root canal.
Materials and Methods:
Root canals of 32 extracted human mandibular premolar teeth were prepared and obturated using EndoREZ + resin-coated gutta-percha points (group A), Epiphany + Resilon points (group B), or AH Plus + gutta-percha (group C). The teeth were split longitudinally in bucco-lingual direction and viewed under scanning electron microscope. Photographs were taken at cervical, middle and apical levels for all samples and corresponding measurements were made. The data obtained was statistically analyzed using one-way ANOVA and the post-hoc Bonferroni test for inter-group comparison.
Results:
The results showed that the greatest penetration into dentinal tubules was by EndoREZ sealer (525.2 μ, 327.802 μ and 198.36 μ at cervical, middle and apical third), followed by Epiphany sealer (479.7 μ, 297.212 μ, and 182.22 μ), and the least penetration was seen with AH Plus sealer (224.2 μ, 65.419 μ, and 40.7 μ). The penetration of sealer into the dentinal tubules was statistically significant between each group at each level and between different levels within each group (P<.05).
Conclusion:
The penetration depth of EndoREZ and Epiphany into the dentinal tubules is significantly greater than that of AH Plus.
Keywords: EndoREZ; Epiphany, AH Plus, sealer penetration, scanning electron microscope
INTRODUCTION
Complete three-dimensional obturation of the root canal system with an impervious, biocompatible and dimensionally stable filling material is important for endodontic success.[1] The quality of root canal filling and coronal restoration after root canal treatment have a strong effect on the outcome of endodontic treatment.[2] Inability to completely obliterate the irregularities of root canal spaces with the filling material and adequately sealing the apical foramen, accounts for nearly 60% of root canal failures.[3] Root canal sealers serve as lubricants and are necessary to fill voids and irregularities in the space between dentinal walls and the obturating material, so as to effectively seal the interface. Thus, a desirable property of a root canal sealer is to have good sealing ability[4] along with adequate adhesive strength (both to dentin and the core material) and cohesive strength to hold the obturation together.[5]
Interest in application of adhesive dentistry concepts to endodontics has been stimulated by the introduction of resin-based root canal sealers. They are emerging as the material of choice due to their ability to penetrate deeper into the dentinal tubules in comparison to the existing sealers. Factors affecting the tubular penetration of the sealers include surface activity of sealers, contact angle formed between sealer and root dentin, diameter of the open dentinal tubules, and obturation technique employed.[6] They may also exert antibacterial effect either by entombing any residual bacteria, or directly through their chemical composition.[7]
An inverse relationship exists between microleakage and dentinal tubule penetration of sealers i.e., as the penetration increases, the microleakage decreases.[6] Thus, greater penetration of root canal sealers into the dentinal tubules may enhance the potential for successful outcome of endodontic therapy. This is because greater penetration increases the surface contact between the root canal and the sealant material, thus improving the sealing ability and retention at the material and dentin interface. The aim of this study was to establish the average depth of penetration of three resin-based root canal sealers (EndoREZ, Epiphany and AH Plus) into the dentinal tubules at the cervical, middle and apical third levels.
MATERIALS AND METHODS
Thirty-two human permanent mandibular first premolars with relatively straight roots, and fully formed apices (freshly extracted for orthodontic reasons), were selected. The teeth were cleaned using an ultrasonic scaler (Satelec Acteon, Cedex, France) and stored in normal saline until use.
Specimen preparation
The teeth were sectioned at 14 mm from the apex, using a diamond disk in a slow speed handpiece under copious water irrigation. The canal patency was checked with the help of a #10 K-file. The pulp tissue was extirpated with a barbed broach.The working length was established using radiographs up to 1 mm short of the apical foramen. The apex was sealed using sticky wax to prevent extrusion of irrigants. Biomechanical preparation of the canals was done using ProTaper instruments (Dentsply-Maillefer, Ballaigues, Switzerland) till size F3, along with Glyde File Prep (Dentsply-Maillefer, Ballaigues, Switzerland) for lubrication during instrumentation. During the entire preparation, alternate irrigation and recapitulation was done with 5.25% sodium hypochlorite (NaOCl) (Avarice Laboratory, Ghaziabad, India) and #10 K-file, respectively. Smear layer was removed by irrigating the canals with 3 ml of freshly prepared 17% ethylene diaminetetracetic acid (EDTA) solution (Orango Laboratories, Mumbai, India), followed by irrigation with 3 ml of 5.25% NaOCl, each for 3 minutes. EDTA was employed as the final rinse, followed by a rinse with distilled water. Canals were dried using paper points for 1 to 2 seconds.
All the samples were divided randomly into 3 groups of 10 teeth each, while the remaining 2 teeth served as a negative control. Lateral compaction technique was applied for the obturation of samples using 6% gutta-percha or Resilon points as the initial cone, followed by filling of any remaining space with accessory cones. Manufacturers’ instructions were followed for the manipulation of each sealer material.
Groups
Group A (ER): EndoREZ sealer (UltradentProducts Inc, South Jordan, UT, USA) along with 6% resin-coated gutta-percha points (RCGP) (Ultradent, USA) of size 30.
Group B (EP): Epiphany sealer (Pentron Clinical Technologies, USA) along with 6% Resilon points (Resilon Research LLC, USA) of size 30.
Group C (AH): AH Plus sealer (Dentsply-DeTrey, Switzerland) along with 6% gutta-percha points (Dentsply-Maillefer, Ballaigues, Switzerland) of size 30.
Radiographs were taken to assess the quality of obturation. The canal orifices were sealed with sticky wax. All specimens were stored in 100% relative humidity at 37°C for 24 hours to ensure complete set of the root canal sealers.
Scanning electron microscope analysis
Samples were then sectioned in the bucco-lingual direction with the help of a safe-sided cutting disc under copious irrigation with distilled water. The half which retained the obturation material was chosen for examination under a scanning electron microscope (LEOVP435, Cambridge, UK). The tooth halves were soaked in EDTA solution for 10 minutes, followed by soaking in 5.25% NaOCl solution for 10 minutes, and then washed thoroughly with distilled water. Samples were dehydrated and gold sputtered for SEM evaluation.
Evaluation of sealer penetration
Samples were studied for dentinal tubule penetration of sealers at three levels - coronal, middle and apical levels. Photographs showing the maximum penetration at each level were taken. At each level, 5 points were marked corresponding to the maximum sealer penetration; the distance of the points was measured from the sealer-dentin interface and the depth of penetration was calculated. A mean of five readings was taken at each level. The data obtained was subjected to statistical analysis using the one-way analysis of variance (ANOVA), followed by post-hoc analysis (Bonferroni) for intergroup comparison of means. The probability value was set at P<.05.
RESULTS
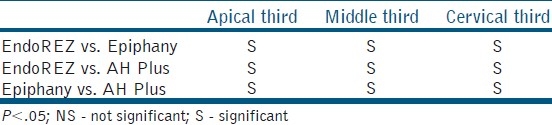
The mean depth of tubular penetration of sealers and standard deviation in different experimental groups at different levels is presented in Table 1. Statistical analysis [Table 2] showed that there was a statistically significant difference between each group at each level, and also between different levels within each group (P<.05).
Table 1.
Mean depth of tubular penetration of sealers at different levels, in microns (μ) in the experimental study

Table 2.
Post-hoc analysis for significant difference in tubular penetration in different thirds in the experimental study
DISCUSSION
The penetration of root canal sealers into the dentinal tubules is considered to be a desirable outcome as it increases the interface between the filling material and dentin, and might improve the retention and sealing ability of the obturation. In the present study, the depth of penetration of three resin-based root canal sealers (EndoREZ, Epiphany and AH Plus) into the dentinal tubules was evaluated with the help of a SEM. In all the experimental groups, greater penetration was seen at the cervical third, followed by the middle third, and least in the apical third. This difference in penetration could be due to the presence of significantly higher density of dentinal tubules with greater diameter at the cervical and middle third, as compared to the apical third.[8]
The cleaning and shaping procedure for all samples was carried out using hand ProTaper instruments so as to obtain a uniform root canal preparation. The presence of smear layer has been shown to obstruct the sealers from penetrating the dentinal tubules.[9] Accordingly, the smear layer was removed by the sequential use of EDTA solution followed by 5.25% NaOCl, with the help of 30 gauge NaviTip tips (Ultradent, USA), so as to reach closer to the apex and produce maximum effect on the entire length of the canal wall.
A final rinse of EDTA solution was given followed by a rinse with distilled water, to eliminate the effect of the residual oxygen liberated from NaOCl on polymerization of resin sealers. The canal was dried with paper points for only 1-2 seconds, as the manufacturers of EndoREZ and Epiphany suggest that complete dehydration might hinder the penetration of the hydrophilic resins into the dentinal tubules.
The obturation of the samples was carried out using lateral compaction technique as it has been shown that adding a core of laterally condensed gutta-percha gives a better control of the filling procedure, and helps to press the resin into the dentinal tubules, and into irregularities in the canal walls, producing a tight contact with the dentin surface.[1] Gutta-percha cones of 6% taper were used as the master cones for use with AH Plus instead of ProTaper F3 cones, to provide standardization between the groups. Quartz tungsten halogen (QTH) light source was preferred over plasma arc or light-emitting diode (LED) to obtain a better seal in case of EndoREZ. It has been found that QTH brings about slower polymerization that allows the material to flow in pregel stage, providing some stress relief during polymerization shrinkage.[10]
It has been shown that maximum penetration of the sealers into the dentinal tubules occurs in the buccal and lingual direction.[11] Hence, longitudinal sections of the tooth samples were taken for evaluation. The sections were evaluated using SEM as it allows highly detailed observation of the dentinal tubules and the sealer. It allows accurate measurement of penetration depths.[12] Further, it does not require any dye incorporation. Therefore, it was decided to use the SEM for visualization of resin penetration.
The results of this study showed significantly (P<.05) greater penetration in group A (ER) at the cervical third (525.2 μ) as compared to the middle third (327.802 μ), and at the apical third (198.36 μ). The penetration at middle third was significantly greater than at the apical third. Sevimay and Kalayci[13] had also reported greater penetration of EndoREZ in the cervical and middle third as compared to apical third, at which no penetration was seen. However, in our study, penetration of EndoREZ at the apical third was seen. This could be due to better smear layer removal; and also due to the fact that in their study the canals were dried completely, while we left them slightly moist, as per the manufacturer's recommendation. The greater penetration of EndoREZ reported by Mamootil and Messer[12] (863 μ) as compared to our study could be due to difference in the root sectioning method, as they used transverse root sections for SEM evaluation rather than longitudinal sectioning as used in our study.
The mean penetration for Group B (EP) at cervical third (479.7 μ) was found to be significantly greater than at the middle (297.212 μ) or at the apical third (182.22 μ). The penetration at the middle third was significantly greater than at the apical third. This trend was in agreement with the results of previous researches.[14,15] In contrast to our study, a greater penetration depth for Epiphany was reported by Gharib et al. [15] (714.9 μ, 538.1 μ and 303.8 μ at the cervical, middle and apical third respectively) and by Patel et al.[14] for RealSeal, a sealer similar to Epiphany (1114.88 μ, 914.88 μ and 696.75 μ at the cervical, middle and apical third respectively). This could be due to the incorporation of Rhodamine B dye, or due to the difference in the obturation technique, or the sectioning method employed.[13]
The mean penetration for Group C (AH) at cervical third (224.2 μ) was found to be significantly greater than at the middle (65.419 μ) or at the apical third (40.7 μ). The penetration at the middle third was significantly greater than at the apical third. The lesser depth of penetration for AH Plus as shown previously by Kokkas et al.[9] (54.6 μ) could be due to difference in the smear layer removal method, as we used 5.25% of NaOCl along with 17% freshly prepared EDTA, while Kokkas et al. used a concentration of 1% NaOCl and 17% EDTA. The lesser depth of penetration shown by Balguerie et al.[16] (122 μ at the cervical third) could be due to the difference in the obturation method, or the difference in sectioning method employed.
The lesser amount of penetration seen with Epiphany as compared to EndoREZ could be due to the difference in the viscosity of the sealers. As a thinning resin is added to adjust the viscosity of the Epiphany sealer, it is speculated that the viscosity obtained was not adequate to allow it to penetrate to greater depths.
The penetration for group A (ER) was found to be significantly greater (P<.05) than that for group C (AH) at all levels. At different levels, the penetration for group B (EP) was found to be significantly greater (P<.05) than that for group C (AH).This difference in penetration, at cervical, middle and apical third, could be explained on the basis of the composition of the sealers. EndoREZ and Epiphany sealers with a hydrophilic composition displayed greater penetration than AH Plus sealer. Also, the silicone oil in AH Plus could have prevented it from flowing into the moist dentin.
The present study focuses on one of the properties desirable of an ideal root canal sealer, that is, formation of a bond between the filling material and dentin. EndoREZ and Epiphany showed extensive penetration at all levels and would theoretically be able to form strong bonds with the root canal wall, resulting in a clinically successful outcome.
CONCLUSION
Within the limitation of the experimental design and the test parameters, it can be concluded that the tubular penetration of EndoREZ and Epiphany is significantly greater than that of AH Plus.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ahlberg KM, Tay WM. A methacrylate-based cement used as a root canal sealer. IntEndod J. 1998;31:15–21. [PubMed] [Google Scholar]
- 2.Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabiwala K. Outcome of primary root canal treatment: Systematic review of the literature - Part 2. Influence of clinical factors. Int Endod J. 2008;41:6–31. doi: 10.1111/j.1365-2591.2007.01323.x. [DOI] [PubMed] [Google Scholar]
- 3.Dow PR, Ingle JI. Isotope determination of root-canal failure. Oral Surg Oral Med Oral Pathol. 1955;8:1100–4. doi: 10.1016/0030-4220(55)90062-1. [DOI] [PubMed] [Google Scholar]
- 4.Branstetter J, von Fraunhofer JA. The physical properties and sealing action of endodontic sealer cements: A review of literature. J Endod. 1982;8:312–6. doi: 10.1016/S0099-2399(82)80280-X. [DOI] [PubMed] [Google Scholar]
- 5.Himel VT, McSpadden, Goodis HE. Instruments, materials and devices. In: Cohen S, Hargreaves KM, editors. Pathways of the pulp. 9th ed. St. Louis, Mo.: Mosby Inc.; 2006. p. 265. [Google Scholar]
- 6.Sen BH, Piskin B, Baran N. The effect of tubular penetration of root canal sealers on dye microleakage. Int Endod J. 1996;29:23–8. doi: 10.1111/j.1365-2591.1996.tb01355.x. [DOI] [PubMed] [Google Scholar]
- 7.Heling I, Chandler NP. The antimicrobial effect within dentinal tubules of four root canal sealers. J Endod. 1996;22:257–9. doi: 10.1016/s0099-2399(06)80144-5. [DOI] [PubMed] [Google Scholar]
- 8.Ferrari M, Mannocci F, Cagidiaco M, Mjor I. Bonding to root canal: Structural characteristics of the substrate. Am J Dent. 2000;13:255–60. [PubMed] [Google Scholar]
- 9.Kokkas AB, Boutsioukis AC, Vassiliadis LP, Stavrianos CK. The influence of the smear layer on dentinal tubule penetration depth by three different root canal sealers: An in vitro study. J Endod. 2004;30:100–2. doi: 10.1097/00004770-200402000-00009. [DOI] [PubMed] [Google Scholar]
- 10.Nagas E, Cehreli ZC, Durmaz V, Vallittu PK, Lassila LV. Regional push-out bond strength and coronal microleakage of Resilon after different light-curing methods. J Endod. 2007;33:1464–8. doi: 10.1016/j.joen.2007.07.028. [DOI] [PubMed] [Google Scholar]
- 11.Weis MV, Parashos P, Messer HH. Effect of obturation technique on sealer cement thickness and dentinal tubule penetration. Int Endod J. 2004;37:653–63. doi: 10.1111/j.1365-2591.2004.00839.x. [DOI] [PubMed] [Google Scholar]
- 12.Mamootil K, Messer HH. Penetration of dentinal tubules by endodontic sealer cements in extracted teeth and in vivo. Int Endod J. 2007;40:873–81. doi: 10.1111/j.1365-2591.2007.01307.x. [DOI] [PubMed] [Google Scholar]
- 13.Sevimay S, Kalayci A. Evaluation of apical sealing ability and adaptation to dentin of two resin-based sealers. J Oral Rehab. 2005;32:105–10. doi: 10.1111/j.1365-2842.2004.01385.x. [DOI] [PubMed] [Google Scholar]
- 14.Patel DV, Sherriff M, Ford TR, Watson TF, Mannocci F. The penetration of RealSeal primer and Tubliseal into root canal dentinal tubules: A confocal microscopic study. Int Endod J. 2007;40:67–71. doi: 10.1111/j.1365-2591.2006.01184.x. [DOI] [PubMed] [Google Scholar]
- 15.Gharib SR, Tordik PA, Imamura GM, Baginski TA, Goodell GG. A confocal laser scanning microscopic investigation of the Epiphany obturation system. J Endod. 2007;33:957–61. doi: 10.1016/j.joen.2007.03.011. [DOI] [PubMed] [Google Scholar]
- 16.Balguerie E, Georgelin-Gurgel M, Diemer F, Calas P. Root canal sealers: Scanning electron microscope study of tubular penetration. Eur Cells Mater. 2007;13:29. [Google Scholar]