

Abstract
Background & objectives:
India has the second highest HIV population in the world with about 2.5-3.0 million cases. HIV-2 cases among general and blood donor population have also been reported mostly from west and south India. This single centre study was carried out to observe the HIV-1 and HIV-2 prevalence among blood donors from north India.
Methods:
A total of 2,04,677 people were screened for the presence of HIV infection over the 11 year period (1999 to 2009). Till 2004, a third generation ELISA kit was used. From 2005 till January 2009 all tests were done using the fourth generation ELISA kit which detected the presence of HIV-1 P24 antigen and anti-HIV antibodies. From February 2009 onwards, the kits used were Genscreen ULTRA HIV Ag-Ab Assay.
Results:
A total of 506 (0.247%) donors were found to be repeat reactive for HIV. Of these, 486 (96%) donors tested using the Western blot were found positive for HIV-1 infection. Twenty (4%) donors showed a negative Western blot result, none of the donors were found reactive for HIV-2 infection.
Interpretation & conclusions:
The prevalence of HIV was 0.249 per cent among blood donors of north India. No HIV-2 case was found among the studied blood donor population indicating that it is not a threat currently.
Keywords: Donor screening, HIV-1, HIV-2, north India, prevalence
According to the United Nations Joint Program on HIV/AIDS (UNAIDS), at the end of 2010, an estimated 34 million people with AIDS living within the world1. The highest number of patients (22.9 million) is reported from sub-Saharan Africa (31.6-35.2 million)2. India harbours the third largest number of HIV infected individuals in the world3. Several States in India have now reported the presence of HIV-2 after the first case was reported from Mumbai in 19914.
HIV infection resulting from blood transfusion has been documented repeatedly since the first case report from the United States in late 19825. The problems of transfusion associated acquired immuno deficiency syndrome resulted in a notification in 1989 under the Drugs and Cosmetics Act which made the test for HIV mandatory6. Several methods are available for the detection of HIV which detect the presence of anti-HIV antibody or the HIV antigen or both. Recently, nucleic acid based tests which are either PCR or transcription mediated amplification to detect the viral nucleic acid have been introduced for blood donor screening7. The specialized rapid assays and the Western blot are two commonly used assays which differentiate between HIV-1 and HIV -2.
Cases of HIV-2 have been reported by several studies from southern and western part of India4 ; however, not much evidence is available from the northern part of our country. This study undertaken at Indraprastha Apollo Hospital, New Delhi, was aimed to find the prevalence of HIV-1 and HIV-2 among the blood donor population of north India.
Material & Methods
All donors who donated blood at the Indraprastha Medical Corporation Limited Blood Bank, Indraprastha Apollo Hospital, New Delhi, a tertiary care hospital in north India, from a period 1999 to 2009, were included in the study. The donors were apparently healthy adults of the age group 18-60 yr. All donors were subjected to a pre-test counselling which was done by qualified staff trained to screen donors for blood donation. Donors who did not fulfil the general criteria for blood donation, paid and commercial donors and those with a history of high risk behaviour were excluded. Consent for infectious marker testing was obtained from all donors at the time of pre-test counselling prior to blood donation.
The donor blood samples were collected at the time of blood donation from the primary bag and tested for the presence of HIV using enzyme linked imunosorbent assay (ELISA). Till 2004, a third generation ELISA kit (Ortho HIV1/2, Clinical Diagnostics, Johnson & Johnson, USA) using fully automated ARIO walk away system, was used. It detected the presence of anti-HIV antibodies in the serum of blood donors. From 2005 till January 2009, all tests were done using the fourth generation ELISA kit (Genscreen HIV1/2, Bio-Rad, USA) on a fully automated platform EVOLIS which detected the presence of HIV-1 P24 antigen and anti-HIV antibodies. From February 2009 onwards, the kits used were Genscreen ULTRA HIV Ag-Ab Assay from Bio-Rad. All samples tested positive by ELISA were repeat tested in duplicate using the same ELISA kit and using the same sample obtained from the donor at the time of blood donation. If the donor was found repeatedly reactive, the sample was subjected to Western blot testing using the HIV 2.2 Genelab Kit, Singapore. All Western blot results were interpreted using the WHO criterion8.
Statistical analysis: Data were analyzed statistically by Chi-square test.
Results
A total of 2,04,677 people were screened for the presence of HIV over the 11 year period. Of these, 1, 92,954 (94.2%) donors were males and 11,723 (5.8%) donors were females; 511 (0.249%) were found initially reactive for HIV. Upon repeat testing in duplicate 506 (0.247%) donors were found to be reactive. These included 207 (210 initial reactive) donors from 1999-2004 when third generation HIV ELISA kits (Ortho HIV1/2), were used and 299 (301 initial reactive) donors when fourth generation kits (Genscreen) were used.
Of the donors testing positive for HIV by ELISA, 97.4 per cent (493/506) were males and 2.6 per cent (13/506) were females. A high rate of HIV positivity 54.9 per cent (278/506) was seen in the age group of 18-30 yr and a small fraction 3.9 per cent (20/506) were in the age category of 51-60 yr. The 31-40 yr olds showed the second highest clustering of HIV positives, 27.7 per cent (140/506) followed by 13.4 per cent (68/506) in the age range of 41-50 yr.
All the 506 donor samples found positive on repeat testing were further tested by Western blot. The WHO criterion used requires the presence of at least two envelope bands (gp 160, gp120, gp41) with or without the presence of gag and pol gene products. Of the 506 donors tested using the Western blot, 486 (96%) were found positive for HIV-1 infection. Whereas 20 (4%) donors showed a negative Western blot result. None of the donors were found reactive for HIV-2 infection.
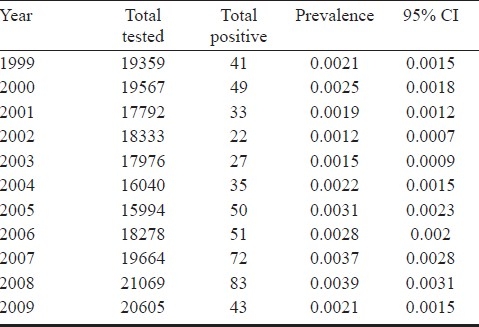
To study the prevalence of HIV positivity during the period (1999-2009), Chi square goodness of fit was employed to see the trend over the period, the results indicated no change over the period under consideration (Table).
Table.
Year-wise prevalence of HIV with 95% CI
Discussion
The first documented HIV infection in India was among a cohort of sex workers in the southern State of Tamil Nadu, in 19869,10. The virus since then has been spreading rapidly across the country. States with a high prevalence of HIV include Maharashtra, Tamil Nadu, Karnataka, Andhra Pradesh, Manipur, and Nagaland1,9. Within these high-prevalence areas, the HIV epidemic reflects the diverse social, cultural, religious, and sexual practices11,12. There are “hot spots,” where commercial sex work is common, such as in coastal Andhra Pradesh, northern Karnataka, and southern Maharashtra1.
Epidemiology of HIV-2 is much varied. Ever since its first occurrence from Senegal, West Africa in 198613, many cases of HIV-2 have been reported from various parts of the world especially in the West African countries14,15. Several reports of HIV-2 infection have been received from Portugal, Mozambique, Angola, South-Western India and Brazil, all areas with former ties to Portugal14–16. We did not find any HIV-2 seropositive donors.
The indeterminate results using this WHO criterion for Western blot interpretation were 4 per cent. The switch from third to fourth generation assays resulted in a decreased rate of false positivity and hence, increased specificity. The specificity increased from 98.57 per cent (207 out of 210 were repeat reactive) to 99.33 per cent (299 out of 301 showing repeat reactivity). The prevalence of HIV among our blood donor population was found to be 0.247 per cent using serological tests (third and fourth generation ELISA).
The prevalence of HIV reported in Indian blood donors ranges from 0.084-3.87 per cent17. A study conducted on blood donors at a tertiary care centre of the Armed forces revealed seropositivity rates of 0.12 per cent in 2003, 0.17 per cent in 2004 and 0.10 in 2005, with an overall seropositivity of 0.13 per cent17. Four major blood banks in the capital jointly reported an overall HIV seroprevalence of 3.1 per thousand donors. HIV-1 constituted the major bulk (89.0%), HIV-2 was detected only in two cases (1.4%) and HIV-1/2 in 9.6 per cent of the samples18. In our previous study which compared the trends of HIV infection in blood donors of Delhi, the HIV seropositivity rates per 1000 samples screened among voluntary donors were 0.63, 0.45, 1.9, 3.03, and 3.87 in 1989, 1990, 1991, 1992, and 1993, respectively. Among replacement donors, these rates were 0.46, 0.50, 1.9, 5.24, and 7.48, respectively. Among professional donors, these rates were 1.50, 0.90, 1.3, 3.28, and 3.76, respectively19.
The presence of HIV-2 has been reported from south-western part of India4, whereas no data are available from the northern part of the country. We, in the present study failed to demonstrate any case of HIV- 2. Among the 4,31,300 blood donors screened for HIV at a tertiary care hospital of south India, 350 (0.81%) were positive for HIV. Of these, 304 (0.704%) were positive for HIV-1, while 46 (0.106%) were positive for the HIV-220. Thakral et al21, showed a 0.16 per cent seropositivity of HIV-2, while Singh and colleagues22 demonstrated HIV-2 seropositivity rates of 0.54 per cent among blood donors of Delhi. Kannangai et al4 showed a very low frequency of HIV-2 infection (0.003%). There have also been reports of HIV-1 and -2 dual infections predominantly from the southern States of India4. A high prevalence of HIV-2 was also seen in a group of high risk individuals in a study conducted in Mumbai23. The rate of monoinfection with HIV-2 was 4 per cent and that of dual infection was 20 per cent23.
According to NACO, more men are HIV positive than women. Nationally, the prevalence rate for adult females is 0.29 per cent, while that for males is 0.43 per cent. The findings of higher infectivity among men in the reproductive age group, in the present study are in concurrence with the findings of other studies on blood donors16. Heterosexual promiscuity seems to be the only cause of higher seropositivity in males. In our study, only 2.6 per cent females were tested positive for HIV as compared to males who were in majority (97.4%).
In conclusion, HIV-1 remains the major threat for transfusion transmitted infections in India, and HIV-2 does not appear to be a significant threat to the current blood supply in north India.
References
- 1.UNAIDS Data Table 2011. [accessed on December 28, 2011]. Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2011/JC2225_UNAIDS_datatables_en.pdf .
- 2.UNAIDS World AIDS Day Report 2011. [accessed on December 28, 2011]. Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2011/JC2216_WorldAIDSday_report_2011_en.pdf .
- 3. [accessed on December 28, 2011]. Available from: http://www.unicef.org/india/hiv_aids_156.htm (UNICEF)
- 4.Kannangai R, Nair SC, Sridharan G, Prasannakumar S, Daniel D. Frequency of HIV type 2 infections among blood donor population from India: A 10-year experience. Indian J Med Microbiol. 2010;28:111–3. doi: 10.4103/0255-0857.62485. [DOI] [PubMed] [Google Scholar]
- 5.Lange JM, Van den Berg H, Dooren LJ, Vossen LM, Kuis W, Goudsmit J. HTLV III/LAV infec-tion in nine children infected with a single plasma donor: clinical outcomes and recognition patterns of viral proteins. J Infect Dis. 1986;154:171–4. doi: 10.1093/infdis/154.1.171. [DOI] [PubMed] [Google Scholar]
- 6.The Gazette of India. New Delhi: Ministry of Health & Family Welfare; 1989. Ministry of Health & Family Welfare, Government of India (1989): Drugs and Cosmetics Act. [Google Scholar]
- 7.Allain JP. Genomic screening for blood borne viruses in transfusion settings. Clin Lab Haematol. 2000;22:1–10. doi: 10.1046/j.1365-2257.2000.00265.x. [DOI] [PubMed] [Google Scholar]
- 8.WHO. Acquired immunodeficiency syndrome (AIDS).Proposed criteria for interpreting results from Western blot asssays for HIV-1, HIV-2 and HTLV-I/HTLV-II. Weekly Epidemiol Rec. 1990;65:281–98. [PubMed] [Google Scholar]
- 9.John TJ, Babu PG, Jeyakumari HM, Simoes EAF. Current prevalence and risk groups of HIV infection in Tamil Nadu, India. Lancet. 1987;1:160–1. doi: 10.1016/s0140-6736(87)91992-1. [DOI] [PubMed] [Google Scholar]
- 10.Simoes EA, Babu PG, Jeyakumari HM, John TJ. The Initial detection of Human Immunodeficiency virus 1 and its subsequent spread in Prostitutes in Tamil Nadu, India. J Acquir Immune Defic Syndr. 1993;6:1030–4. [PubMed] [Google Scholar]
- 11.Steinbrook R. HIV in India - A Complex Epidemic. N Engl J Med. 2007;356:1089–93. doi: 10.1056/NEJMp078009. [DOI] [PubMed] [Google Scholar]
- 12.Chandrasekaran P, Dallabetta G, Loo V, Rao S, Gayle H, Alexander A. Containing HIV/AIDS in India: the unfinished agenda. Lancet Infect Dis. 2006;6:508–21. doi: 10.1016/S1473-3099(06)70551-5. [DOI] [PubMed] [Google Scholar]
- 13. [accessed on December 28, 2011]. Available from: http://www.aegis.com/pubs/cdc_fact_sheets/1996/CDC96091.html .
- 14.Kanki PJ. Human immunodeficiency virus type 2 (HIV-2) AIDS Rev. 1999;1:101–8. [Google Scholar]
- 15.Kanki P, DeCock K. Epidemiology and natural history of HIV-2. AIDS. 1994;8:S1–9. [Google Scholar]
- 16.Smallman-Raynor M, Cliff A. The spread of human immunodeficiency virus type 2 into Europe: A geographical analysis. Int J Epidemiol. 1991;20:480–9. doi: 10.1093/ije/20.2.480. [DOI] [PubMed] [Google Scholar]
- 17.Chattoraj A, Behl R, Kataria VK. Infectious disease markers in blood donors. Med J Armed Forces India. 2008;64:33–5. doi: 10.1016/S0377-1237(08)80142-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Krishna R, Gupta SM, Manju B. Prevalence of HIV Antibodies in replacement blood donors in Delhi, India. J AIDS. 2001;26:393–4. doi: 10.1097/00126334-200104010-00021. [DOI] [PubMed] [Google Scholar]
- 19.Makroo RN, Salil P, Vashist RP, Shivlal Trends of HIV infection in the blood donors of Delhi. Indian J Pathol Microbiol. 1996;39:139–42. [PubMed] [Google Scholar]
- 20.Sonth SB, Solabannavar SS, Baragundi MC, Patil CS. The prevalence of HIV-2 seropositivity in blood donors. J Clin Diagn Res. 2010;4:3091–4. [Google Scholar]
- 21.Thakral B, Saluja K, Sharma RR, Marwaha N. Alogrithm donors for recall of HIV reactive Indian blood donors by sequential immunoassays enables selective donor referral for counseling. J Postgrd Med. 2006;52:106–9. [PubMed] [Google Scholar]
- 22.Singh B, Verma M, Kotru M, Verma K, Batra M. Prevalence of HIV & VDRL seropositivity in blood donors of Delhi. Indian J Med Res. 2005;122:234–6. [PubMed] [Google Scholar]