

Abstract
A patient presented with shortness of breath, lethargy and weight loss. A computerized tomography and echocardiogram showed a mass in the right ventricle nearly obstructing the pulmonary valve during systole and prolapsing into the main pulmonary artery. The mass was completely excised. Histology was that of a typical myxoma.
Keywords: Myxoma, Cardiac tumour, Right ventricle
CASE REPORT
A 60-year old man presented with a 1-month history of increasing shortness of breath, lethargy and weight loss. Investigations revealed normal haematology and biochemistry. A computerized tomography scan of the abdomen and chest was performed to exclude malignancy. This showed no abdominal pathology but a large mass in the right ventricle extending into the right ventricular outflow tract (Fig. 1). An echocardiograph confirmed this mass in the right ventricle and showed it nearly obstructing the pulmonary valve during systole and prolapsing into the main pulmonary artery (Fig. 2, Supplementary Videos 1 and 2). There was pulmonary valve obstruction with a right ventricular systolic pressure of 70 mmHg. The mass appeared to arise from the body of the right ventricle. The right atrium and vena cavae appeared normal.
Figure 1:

Initial computerized tomography scan of the chest showing the mass in the right ventricle extending into the main pulmonary artery (arrow).
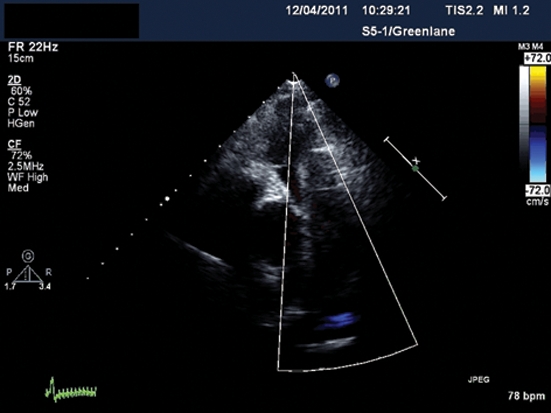
Figure 2:

Parasternal short-axis echo views, with and without colour Doppler, showing the large myxoma nearly obstructing the right ventricular outflow tract (RVOT). The aortic valve (A) is seen adjacent to the pulmonary valve.
Supplementary Video 1:

Parasternal short-axis echo cine showing the large mass arising in the right ventricle and prolapsing through the pulmonary valve causing right ventricular outflow tract obstruction.
Supplementary Video 2:
The corresponding cine with colour Doppler showing the extent of pulmonary valve obstruction.
The patient underwent emergent surgery to remove the mass which was attached to the right ventricular outflow tract by a stalk. The large mass was removed in two pieces, one measuring 60 × 40 × 30 mm and the other 45 × 40 × 30 mm. The macroscopic appearance was of a myxoma and histology confirmed a typical myxoma which was completely excised. The patient made an uneventful recovery.
Benign cardiac tumours are rare with a rate of 0.03% at autopsy; myxomas being the most common of these benign tumours, accounting for 75–80% of primary tumours of the heart [1, 2]. This patient presented with the typical constitutional symptoms of a myxoma and symptoms from pulmonary valve obstruction. These tumours usually arise from the left atrial side of the intra-atrial septum in up to 90% of cases. After that, most arise from the right atrium or the left ventricular cavity. Rarely are they seen in the right ventricle [1, 2] as was the case with this patient.
About 20–25% of primary cardiac tumours are malignant, the vast majority being sarcomas (95%), the remainder being lymphomas (5%). These are usually intramyocardial in nature and not pedunculated as in this case [3]. Metastatic malignancies account for the majority of cardiac tumours. These usually spread by direct extension to the heart and or pericardium. Renal cell carcinoma, lung malignancies, lymphomas and melanomas are the most common tumours [3].
SUPPLEMENTARY MATERIAL
Supplementary material is available at ICVATS online.
Conflict of interest: none declared.
REFERENCES
- 1.Butany J, Nair V, Naseemuddin A, Nair G, Catton C, Yau T. Cardiac tumours: diagnosis and management. Lancet Oncol. 2005;6:219–28. doi: 10.1016/S1470-2045(05)70093-0. [DOI] [PubMed] [Google Scholar]
- 2.Kouchoukos N, Blackstone E, Doty D, Hanley F, Karp K, editors. Kirklin and Barrett-Boyes Cardiac Surgery. 3rd edn. The Netherlands: Elsevier; Chapter 47, Cardiac tumour. [Google Scholar]
- 3.Shapiro LM. Cardiac tumours: diagnosis and management. Heart. 2001;85:218–22. doi: 10.1136/heart.85.2.218. [DOI] [PMC free article] [PubMed] [Google Scholar]