

Abstract
Reinforced endostapling can prevent postoperative air leakage from surgical stumps. We herein present a 58-year old woman with idiopathic interstitial pneumonia who developed lethal haemothorax after a thoracoscopic lung biopsy with the use of an endostapler preloaded with bioabsorbable tissue reinforcement material. This lethal haemothorax, which occurred on the day after the lung biopsy, required an emergency operation. The bleeding point was an intercostal artery of the inferior chest wall adjacent to the surgical stump. The operative findings suggested that the reinforced material on the surgical stump scratched the chest wall through respiratory movement.
Keywords: Endostapler, Reinforcement, Postoperative complication, Haemothorax
INTRODUCTION
Thoracoscopic pulmonary resection with an endostapler is a key diagnostic procedure for interstitial lung disease (ILD). Prolonged air leakage from the staple line may be a risk factor for acute exacerbation of idiopathic pulmonary fibrosis [1]. Polyglycolic acid sheets, fibrin glue and collagen sheets are used to prevent air leakage [2]. We herein report a patient with ILD who developed lethal haemothorax after pulmonary resection with an endostapler preloaded with bioabsorbable tissue reinforcement material (Duet TRS; Covidien) to reduce the air leakage. Intraoperative findings suggested that the bleeding point on the inner chest wall was scratched by the prominent staple line.
CASE REPORT
A 58-year old woman complained of dyspnoea on effort and was diagnosed with interstitial pneumonia by chest computed tomography. Lung biopsy for pathological diagnosis was performed by thoracoscopic surgery via three ports. Pulmonary resection of three lesions in the right lung was performed with an endostapler preloaded with bioabsorbable tissue reinforcement material. Double endostapling with a thickness of 1.5 mm was required for pulmonary resection of the lateral basal segment, which contained a diseased lesion. Single endostapling of two lesions with a thickness of 1.5 mm was required for pulmonary resection of the middle lobe medial segment and anterior segment as control lesions. The surgical lung biopsies were uneventfully completed.
Chest X-rays showed normal findings on the day after the operation. Thereafter, massive pleural bleeding occurred after walking around. Repeated chest X-rays revealed massive haemothorax. An emergency operation was performed through repeated thoracoscopic surgery. Active bleeding was identified from the intercostal artery of the inferior inner chest wall. Haemostasis was successful by electrocauterization. The reinforcement material on the crossing point of the double endostaplings in the lower lobe was sharp and adjacent to the bleeding point under the inflated right lung. These findings suggest that the crossing point of the staple line scratched the inner chest wall in synchrony with respiration, and bleeding occurred. The surgical stump was additionally resected by an endostapler without tissue reinforcement material (Supplementary Video 1). The post-operative course was uneventful.
Supplementary Video 1:
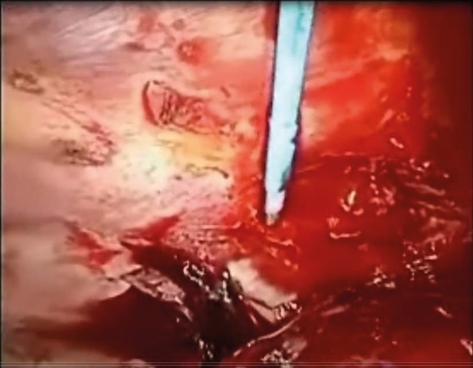
Active bleeding from the inner wall adjacent to the surgical stump of the lateral segment in the right lower lobe was identified during repeated right thoracoscopy. The reinforcement material on the crossing point of the double endostaplings was sharp and scratched the inner chest wall, possibly causing intercostal artery injury under bilateral lung ventilation.
DISCUSSION
Complications of surgical lung biopsy in patients with ILD include fever, prolonged air leakage, respiratory failure, pulmonary infection, pleural effusion, etc. [3]. Prolonged air leakage is one of the risk factors of acute exacerbation of idiopathic pulmonary fibrosis [1]. Endostaplers that are preloaded with a tissue reinforcement material are recommended for the use during pulmonary resection in patients with ILD.
Endostaplers are used safely in most cases, but they sometimes cause haemothorax [4, 5]. Two cases of haemothorax after thoracoscopic surgery using endostaplers without a tissue reinforcement material were reported. Haemorrhage occurred from the internal thoracic artery in one case and from the intercostal artery in another case. The cause of bleeding was speculated to be scratching of the inner chest wall by the edge of the staple line.
In our case, the reinforcement material on the crossing point of the double endostaplings was sharp towards the inner chest wall, which was scratched by the surgical stump in the lateral basal segment during respiratory movement. Careful performance of stapling procedures to avoid scratching the inner wall and additional resection of the sharp reinforcement material on the stump is necessary during pulmonary resection of the lateral segment of the lower lobe using an endostapler.
SUPPLEMENTARY MATERIAL
Supplementary material is available at ICVTS online.
Conflict of interest: none declared.
REFERENCES
- 1.Bando M, Ohno S, Hosono T, Yanase K, Sato Y, Sohara Y, et al. Risk of acute exacerbation after video-assisted thoracoscopic lung biopsy for interstitial lung disease. J Bronchol Interv Pulmonol. 2009;16:229–35. doi: 10.1097/LBR.0b013e3181b767cc. [DOI] [PubMed] [Google Scholar]
- 2.Endo S, Bando M, Sugiyama Y. Surgical lung biopsy for diffuse lung disease. Nihon Kyobu Rinsyo. 2010;69:33–9. [Google Scholar]
- 3.Zhang D, Liu Y. Surgical lung biopsies in 418 patients with suspected interstitial lung disease in China. Inter Med. 2010;49:1097–102. doi: 10.2169/internalmedicine.49.3225. [DOI] [PubMed] [Google Scholar]
- 4.Sakaguchi K, Horio Y, Yamamoto M. Bleeding by staple in video-assisted thoracoscopic interlobar plasty of the lung. Kyobu Geka. 2007;60:907–9. [PubMed] [Google Scholar]
- 5.Motoyama H, Yamashina A, Chihara K. Sudden hemothorax following lobectomy caused by staple. Interact CardioVasc Thorac Surg. 2009;9:117–8. doi: 10.1510/icvts.2009.203786. [DOI] [PubMed] [Google Scholar]