

This report describes a case of a bleeding leiomyoma during twin pregnancy successfully managed by myomectomy in the first trimester.
Introduction
Uterine fibroids are often seen in pregnancy, with a reported prevalence between 0.1% and 15%.1 The incidence is increasing because more women delay pregnancy. The effect of uterine fibroids on fertility and pregnancy depends on number, size and location.1,2 In 2% of all pregnancies with uterine fibroids, conservative therapy fails and myomectomy by laparotomy or laparoscopy had to be performed, mainly for unbearable pain or haemoperitoneum.2 In these cases myomectomy appears to improve pregnancy outcome,3,4 although uterine rupture may occur at a time later in pregnancy.5
Case report
A 33-year-old primigravid woman was referred at 9 weeks' gestation with a dichorionic-diamniotic twin pregnancy. The medical history was uneventful. On obstetrical examination the uterine fundus appeared to be palpable halfway between umbilicus and xiphoid. Abdominal ultrasound demonstrated two viable fetuses and a subserous, broadly pedunculated fibroid of 17.5 × 13 cm at the dorsal side of the uterus. Until then, the patient was unaware of the myoma.
She was admitted to the hospital at 10 weeks' gestation because of vomiting and abdominal pain. The diagnosis of hyperemesis gravidarum, possibly in combination with ischaemia of the myoma, was made. Treatment consisted of rehydration, analgetic, drugs and anti-emetics. The following day, laboratory tests revealed a decrease in haemoglobin levels from 6.9 mmol/L to 4.1 mmol/L. Blood pressure and pulse frequency remained normal. Fluid in the Pouch of Douglas was seen on abdominal ultrasound and MRI, indicating intra-abdominal bleeding. The distance between the gestational sac and the peduncle of the myoma was 13 mm (Figure 1). As conservative therapy failed to stabilize the patient, a laparotomy was performed under general anaesthesia. The abdomen was filled with 3000 mL of blood and coagulated blood. A large venous bleeding was found approximately 3 cm distal from the uterine basis of the peduncle. The peduncle was 6 cm in diameter, the myoma 15 cm (Figure 2). The uterine serosa was opened in order to identify the capsule of the myoma before dissection of the peduncle, clamps were placed on the peduncle and the myometrium was sutured with Vicryl 1-0 (Ethicon). Total blood loss was 4500 mL. The patient received 4 packed cells and 2 units of fresh frozen plasma.
Figure 1.

MRI before surgery
Figure 2.
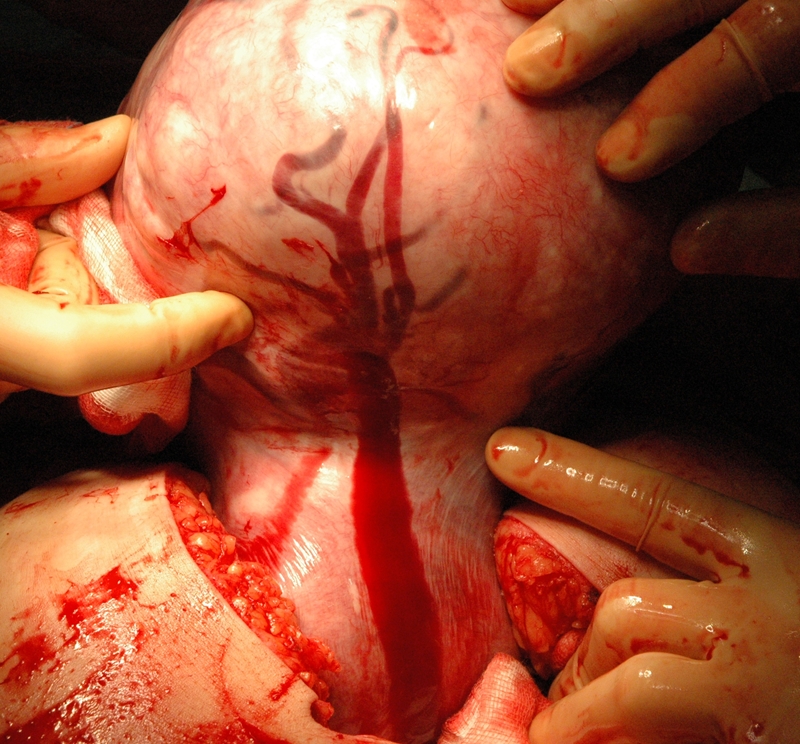
Gravid uterus with pedunculated myoma. Large ruptured vein causing massive intra-abdominal bleeding
Postoperative MRI demonstrated a myometrial thickness of only 5 mm at the site of the dissected peduncle. The patient recovered without complications and was discharged 5 days after surgery. The pathological diagnosis was leiomyoma with necrosis, the myoma weighing 2.745 kg. Repeated ultrasound examinations showed a small hematoma of 2 cm above the surgical site. Caesarean section was planned at 37 weeks. The course of the pregnancy was uneventful until 36 weeks. At 36 weeks, vaginal bleeding and abdominal cramps occurred. No abnormalities were seen on ultrasound examination.
Suspecting a partial abruptio placentae, an emergency Caesarean section was performed, resulting in the birth of two twin sons of normal weight for the gestational age and with optimal APGAR scores. The amniotic fluid of the second child contained blood, and the placenta of the second child showed an indentation supporting the diagnosis of a partial abruption placentae. The postoperative course was uneventful.
Discussion
Myomata in pregnancy are generally asymptomatic.2 Complications usually present in the first trimester of the pregnancy2 due to red degeneration which causes a ‘myomata’ syndrome associated with nausea, vomiting and fever.2,6 In most cases this syndrome can be treated by conservative measures. Myomectomy is inevitable in about 2% of cases.2 Haematoperitoneum and fetal compression syndrome are rare indications for myomectomy in pregnancy. Three reports described massive hemoperitoneum due to a bleeding in subserous uterine leiomyoma in singleton pregnancies.3,7,8 Generally it is stated that bleeding only will occur after trauma or torsion. In our case, no cause for the bleeding could be identified. Kasum et al.7 encountered a massive intraperitoneal bleeding due to a bleeding subserous uterine leiomyoma following gynaecologic examination in a singleton pregnancy, necessitating myomectomy. Wong et al.8 describe spontaneous hemoperitoneum from a 12 cm uterine leimyoma at 8 weeks gestation. They performed no myomectomy, but placed haemostatic sutures around the bleeding venous vessels. Their patient had an uneventful pregnancy and a vaginal delivery. In 1972, Butterly et al.3 published a review on spontaneous hemoperitoneum complicating uterine myomata in both pregnant and non-pregnant women. Death resulted in three out of 53 cases reviewed. In all three cases, hemoperitoneum was associated with pregnancy and no surgical treatment was attempted. Given the imaging techniques and surgical opportunities available nowadays death due to bleeding fibroids is unlikely to occur.
Four papers, including 72 cases, indicate that myomectomy can be performed during pregnancy.4,5,9,10 The rate of pregnancy loss seems similar both in patients treated surgically and in patients treated expectantly. After myomectomy in pregnancy, Caesarean section is the mode of delivery in 94% of the cases.10 We found one case report on myomectomy in a twin pregnancy.2 This case report suggests a relation between the myomectomy in the first trimester and fetal limb anomalies and hydrocephalus in later pregnancy.2 Although evidence is lacking, fetal complications and the risk for pregnancy loss should be taken into consideration before surgery. Our patient presented at 36 weeks' gestation with a partial abruption of the placenta. Several studies describe an increased risk of abruption of the placenta in pregnancies with uterine myomas.1,4 Myomas with a retroplacental and submucosal localization (and myomas with a diameter greater than 7–8 cm) had the highest incidence of placental abruption.1,6 Abnormal trophoblast invasion might be the link between placental abruption and myomas.6 Although conservative measurements remain the first treatment of choice in pregnant patients with myomas, surgery should be considered in selected cases as presented in this report. In contrast to the single other report on myomectomy in a twin pregnancy, both twins were perfectly healthy in our case.
DECLARATIONS
Competing interests
None declared
Funding
None
Ethical approval
Written informed consent to publication was obtained from the patient or next of kin
Guarantor
MHAvH
Contributorship
SRDB wrote the first version of the manuscript and subsequent improved versions; VHMK was the consultant gynaecologist; GY provided the figures and legends; MHAvH assisted during surgery; RMFvdW and MHAvH assisted in the editing of the manuscript
Acknowledgements
None
Reviewer
Uma Krishnamoorthy
References
- 1.Cooper NP, Okolo S Fibroids in pregnancy – common but poorly understood. Obstet Gynecol Surv 2005;60:132–8 [DOI] [PubMed] [Google Scholar]
- 2.Danzer E, Holzgreve W, Batukan C, Miny P, Tercanli S, Hoesli I Myomectomy during the first trimester associated with fetal limb anomalies and hydrocephalus in a twin pregnancy. Prenat Diagn 2001;21:848–51 [DOI] [PubMed] [Google Scholar]
- 3.Butterly BW Spontaneous haemoperitoneum complicating uterine fibromyoma. Aust N Z J Obstet Gynecol 1972;12:210–13 [DOI] [PubMed] [Google Scholar]
- 4.Exacoustos C, Rosati P Ultrasound diagnosis of uterine myomas and complications in pregnancy. Obstet Gynecol 1993;82:97–101 [PubMed] [Google Scholar]
- 5.Mollica G, Pittini L, Minganti E, Perri G, Pansini F Elective uterine myomectomy in pregnant women. Clin Exp Obstet Gynecol 1996;23:168–72 [PubMed] [Google Scholar]
- 6.Rice JP, Ray HH, Mahony BS The clinical significance of uterine myomas in pregnancy. Am J Obstet Gynecol 1989;160:1212–16 [DOI] [PubMed] [Google Scholar]
- 7.Kasum M Hemoperitoneum caused by a bleeding myoma in pregnancy. Acta Clin Croat 2010;49:197–200 [PubMed] [Google Scholar]
- 8.Wong L, Ching TW, Kok TL, Koon TH Spontaneous hemoperitoneum from an uterine leiomyoma in pregnancy. Acta Obstet Gynecol Scand 2005;84:1208–9 [DOI] [PubMed] [Google Scholar]
- 9.Glavind K, Palvio DHB, Lauritsen JG Uterine myoma in pregnancy. Acta Obstet Gynecol Scand 1990;69:617–19 [DOI] [PubMed] [Google Scholar]
- 10.Michalas SP, Oreopoulou FV, Papageorgiou JS Myomectomy during pregnancy and caesarean section. Hum Reprod 1995;10:1869–70 [DOI] [PubMed] [Google Scholar]