

Abstract
INTRODUCTION
Rupture of extensor pollicis longus (EPL) tendon is a recognised complication following volar plate fixation of distal radius fractures, usually from attrition caused by prominent screws. We sought to identify the screw holes in some of the most commonly used plates which may precipitate tendon injury.
SUBJECTS AND METHODS
Three fixed-angle volar locking plates were sequentially positioned into 18 cadaveric arms. A wire was passed through each of the holes in the plates using a locking guide and the dorsal relationships noted.
RESULTS
Each plate had specific ‘high-risk’ holes which directed the wire towards the EPL groove. The central screw holes appeared mostly implicated in EPL injury.
CONCLUSIONS
Awareness of ‘high-risk’ holes and appropriate minor alterations in surgical technique may consequently decrease the incidence of EPL irritation and rupture.
Keywords: Complications, Distal radius fracture, Flexor pollicis longus (FPL), Tendon, Volar plate
Distal radius fractures are one of the most common fractures presenting to orthopaedic surgeons. Traditionally, such fractures have largely been treated by closed reduction and immobilisation in plaster, yet improvements in orthopaedic technology have changed the management of distal radius fractures. The use of volar plates for managing distal radius fracture is now almost universal to orthopaedic surgeons engaged in adult trauma care.
The conventional means of internal fixation of dorsally displaced distal radius fractures was by dorsal plating to create a mechanically stable, dorsal buttress effect. The close proximity between plate and tendons, however, meant that extensor tendon irritation and rupture were common; hence, although it inferred improved fixation, it had unacceptable tendon complications.1-4 Improvements in plate design, in the form of locking plates, have allowed mechanical stability of the fracture to be achieved with plates on the volar surface of the radius, which has better tendon relationships. This mechanical advantage stability, even in osteoporotic bone, allows early active mobilisation and has resulted in a marked increase in the use of volar fixation of distal radius fractures.5,6
Despite the improved tendon relationships, extensor tendon complications remain. Most commonly affected is the tendon of the extensor pollicis longus (EPL), owing to its confinement within the EPL groove. The cause of tendon irritation and rupture is thought to be due to attrition either by prominent screws or perforating the dorsal surface intra-operatively with a drill.7-13
We sought to investigate if it were possible to identify screw hole positions, within three of the most commonly used locking plates in the UK, through which a long screw may pose a risk of injury to the EPL tendon in the EPL groove. This knowledge combined with the understanding that the use of all screw holes is not always necessary to achieve fracture stability may reduce the risk of EPL tendon irritation and rupture.
Subjects and Methods
Eighteen preserved cadaveric forearms were examined. Each arm was from a different individual and had been preserved by freezing and was completely thawed before use. Cadavers were examined both visually and radiographically to ensure that there was no evidence of altered anatomy to the distal radius from previous trauma or other pathology. Volar structures of the forearm were removed to enable easy access to the distal radius. The dorsal surface was similarly exposed to visualise the EPL groove. Ethical permission was obtained prior to commencement of the study.
Three commercially available plates were fixed sequentially in the position of best anatomical fit on to 18 cadaveric arms by a senior surgical trainee in orthopaedic surgery. The plates available to use were ‘standard’ or ‘medium’ size – if a cadaveric arm required a different size plate, this was excluded from our series. The position was confirmed radiologically to ensure that observational best fit matched radiological best fit. The plates used were the Hand Innovations (Miami, FL. USA) DVR plate, the Acumed (Hillsboro, OR, USA) Acu-Loc plate and the AO Synthes LCP distal radius system (Salzburg, Austria).
Each screw hole was drilled, guided by the appropriate locking drill guide with a 1.6-mm K-wire. The exit point of the wire through the dorsal surface of the radius was visualised, and those wires penetrating EPL groove recorded (Fig. 1).
Figure 1.
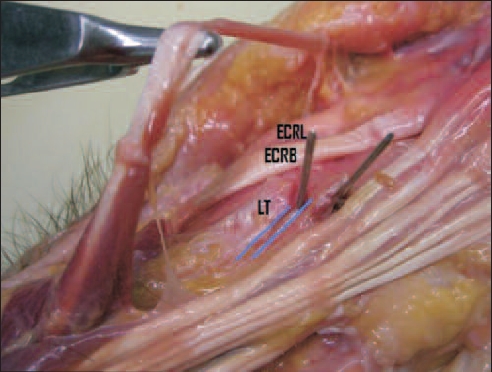
With the tendon of EPL reflected, a K-wire can be seen passing through the EPL groove (blue - see web file) ulna to Lister’s tubercle (LT). A further wire from a different screw hole can also be seen.
Results
All plates had specific screw holes which would reproducibly direct the drill, and hence screw, into the EPL groove.
Thirteen, standard-sized Acumed plates were used (five plates excluded as a non-standard sized plate offered a better fit). The plate had three holes which directed the K-wire to perforate the EPL groove. The third from radial hole on the proximal row was most implicated with EPL groove perforation in five (39%) cases. The second and third from radial screws on the distal row perforated the EPL groove in three (23%) and five (31%) cases, respectively.
Thirteen, standard-sized DVR plates were used (five plates excluded as a non-standard sized plate offered a better fit). The plate had three holes which directed the K-wire to perforate the EPL groove. The second from radial hole on the proximal row was most implicated with EPL groove perforation in seven (54%) cases. The third from radial screw on the distal row was implicated in two cases (15%) and the hole immediately ulna to this in one (7%) case.
Eighteen, universal-sized Synthes plates were used. The plate had three holes which directed the K-wire to perforate the EPL groove. The forth from radial hole was most implicated with EPL groove perforation in seven (38%) cases. The second from radial screw hole directed one (5%) wire towards EPL groove and the third from radial hole directed six (33%) wires.
This information is represented schematically for the operating surgeon in Figures 2 and 3.
Figure 2.
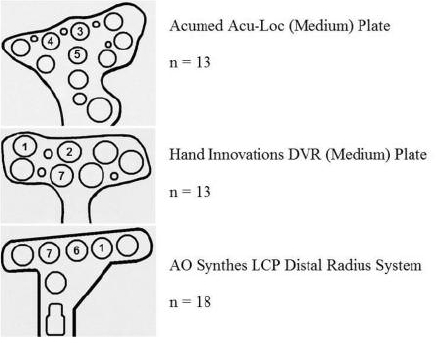
Data by number of hits at EPL groove from each screw hole (all plates shown as right-sided).
Figure 3.
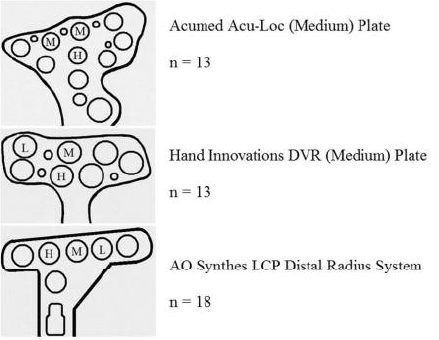
Schematic representation of risk. Risk of EPL groove perforation: H, high probability (> 35%); M, medium probability (10–35%); L, low probability (< 10%); and blank, negligible risk.
Discussion
This study clearly demonstrates that certain screw hole positions, in some of the most commonly used fixed-angle volar locking plates, direct the screw towards the EPL groove and, therefore, risk damaging the tendon.
Injury to the EPL tendon may be especially common because of the intimate relationship of the tendon around Lister’s tubercle at the wrist. The tendon of EPL passes through the extensor retinaculum in the third extensor compartment of the wrist, immediately ulna to Lister’s tubercle, and is further stabilised by the narrow ‘EPL’ groove in the radius. The fixed path and relatively poor blood supply make the EPL tendon particularly vulnerable.14
Volar plating has evolved in the treatment of distal radius fractures owing to the improved tendon relationships compared to dorsal plates; however, tendon complications have not been eliminated. Flexor tendon injury is most common and rupture of FPL (flexor pollicis longus) has been reported in up to 12% of cases.10 Extensor tendon complications following volar plating was first reported in 1989 in a Barton’s fracture and attributed to a prominent screw causing attrition rupture of EPL.13 Since then, numerous similar reports of extensor tendon rupture exist, particularly for EPL, which has been attributed predominantly to prominent screws dorsally causing attrition rupture7,8,13 and direct intra-operative damage through drilling.8 Estimates of the frequency of EPL complications following volar plating vary between 4.4% and 8.6%.7,8,11
Assessing screw prominence in distal radius fractures is difficult, both clinically and radiologically, owing to the complex geometry of the distal radius and the potential for dorsal fracture comminution. Cadaveric studies show that, even with multiple intra-operative fluoroscopic views, radiological detection of screw prominence is difficult.9,15 One study identified that the average screw prominence in the third extensor compartment required for radiological detection was 3.5 mm on lateral views and 2.5 mm on pronated views.15
Intra-operatively, surgeons attempt to overcome extensor tendon complications by a number of means. The use of unicortical screws and the, somewhat problematic, avoidance of dorsal surface penetration can be employed but these may reduce the mechanical stability of the fracture construct. For this reason, bicortical fixation is sometimes essential, and consequently it is important to be aware of the ‘high-risk positions’ to maximise fracture stability whilst minimising tendon complications.
Two previous papers have sought to identify the screw holes which pose a risk to EPL tendon.9,16 One study included only two cadavers, and the other the plate of a single manufacturer. They similarly suggested that the central holes were ‘high-risk’ holes, but did not attempt to schematically present this risk for practical intra-operative use.
Our study, simply and schematically, demonstrates which screw holes persistently pose a risk to the EPL tendon in some of the most commonly used locking plates and allows a surgeon to quantify the risk of penetration of the third dorsal compartment. The agreement of past studies supports the utility and reproducibility of the findings.
Our findings enable a surgeon to use caution at ‘high-risk’ holes and consider the most appropriate method of screw fixation – bicortical, unicortical or none. Fracture fixation and stability must remain the primary goal and we recognise that these should not be compromised in order to attempt to minimise a potential extensor tendon complication.
Conclusions
This study has quantified the risk to the EPL tendon of different screw holes in three of the most commonly used fixed-angle volar locking plates. This will allow the surgeon to consider the implications of screw position to minimise the risk of extensor tendon complications.
Acknowledgments
The senior author (DB) has received an honoraria for lecturing from Acu-Med.
References
- 1.Ring D, Jupiter JB, Brennwald J, Büchler U, Hastings H. Prospective multicenter trial of a plate for dorsal fixation of distal radius fractures. J Hand Surg. 1997;22:777–84. doi: 10.1016/S0363-5023(97)80069-X. [DOI] [PubMed] [Google Scholar]
- 2.Axelrod TS, McMurtry RY. Open reduction and internal fixation of comminuted, intraarticular fractures of the distal radius. J Hand Surg. 1990;15:1–11. doi: 10.1016/s0363-5023(09)91097-8. [DOI] [PubMed] [Google Scholar]
- 3.Rozental TD, Beredjiklian PK, Bozentka DJ. Functional outcome and complications following two types of dorsal plating for unstable fractures of the distal part of the radius. J Bone Joint Surg Am. 2003;85:1956–60. doi: 10.2106/00004623-200310000-00014. [DOI] [PubMed] [Google Scholar]
- 4.Jakob M, Rikli DA, Regazzoni P. Fractures of the distal radius treated by internal fixation and early function. A prospective study of 73 consecutive patients. J Bone Joint Surg Br. 2000;82:340–4. doi: 10.1302/0301-620x.82b3.10099. [DOI] [PubMed] [Google Scholar]
- 5.Larson AN, Rizzo M. Locking plate technology and its applications in upper extremity fracture care. Hand Clin. 2007;23:269–78. doi: 10.1016/j.hcl.2007.02.004. vii. [DOI] [PubMed] [Google Scholar]
- 6.Orbay JL, Fernandez DL. Volar fixation for dorsally displaced fractures of the distal radius: a preliminary report. J Hand Surg. 2002;27:205–15. doi: 10.1053/jhsu.2002.32081. [DOI] [PubMed] [Google Scholar]
- 7.Arora R, Lutz M, Hennerbichler A, Krappinger D, Espen D, Gabl M. Complications following internal fixation of unstable distal radius fracture with a palmar locking-plate. J Orthop Trauma. 2007;21:316–22. doi: 10.1097/BOT.0b013e318059b993. [DOI] [PubMed] [Google Scholar]
- 8.Al-Rashid M, Theivendran K, Craigen MAC. Delayed ruptures of the extensor tendon secondary to the use of volar locking compression plates for distal radial fractures. J Bone Joint Surg Br. 2006;88:1610–2. doi: 10.1302/0301-620X.88B12.17696. [DOI] [PubMed] [Google Scholar]
- 9.Benson EC, DeCarvalho A, Mikola EA, Veitch JM, Moneim MS. Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop. 2006;451:218–22. doi: 10.1097/01.blo.0000223998.02765.0d. [DOI] [PubMed] [Google Scholar]
- 10.Drobetz H, Kutscha-Lissberg E. Osteosynthesis of distal radial fractures with a volar locking screw plate system. Int Orthop. 2003;27:1–6. doi: 10.1007/s00264-002-0393-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lee HC, Wong YS, Chan BK, Low CO. Fixation of distal radius fractures using AO titanium volar distal radius plate. Hand Surg. 2003;8:7–15. doi: 10.1142/s0218810403001339. [DOI] [PubMed] [Google Scholar]
- 12.Nana AD, Joshi A, Lichtman DM. Plating of the distal radius. J Am Acad Orthop Surg. 2005;13:159–71. doi: 10.5435/00124635-200505000-00003. [DOI] [PubMed] [Google Scholar]
- 13.Wong-Chung J, Quinlan W. Rupture of extensor pollicis longus following fixation of a distal radius fracture. Injury. 1989;20:375–6. doi: 10.1016/0020-1383(89)90019-3. [DOI] [PubMed] [Google Scholar]
- 14.Hirasawa Y, Katsumi Y, Akiyoshi T, Tamai K, Tokioka T. Clinical and microangiographic studies on rupture of the E.P.L. tendon after distal radial fractures. J Hand Surg. 1990;15:51–7. doi: 10.1016/0266-7681_90_90048-9. [DOI] [PubMed] [Google Scholar]
- 15.Maschke SD, Evans PJ, Schub D, Drake R, Lawton JN. Radiographic evaluation of dorsal screw penetration after volar fixed-angle plating of the distal radius: a cadaveric study. Hand. 2007;2:144–50. doi: 10.1007/s11552-007-9038-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pichler W, Grechenig W, Clement H, Windisch G, Tesch NP. Perforation of the third extensor compartment by the drill bit during palmar plating of the distal radius. J Hand Surg Eur. 2009;34:333–5. doi: 10.1177/1753193408099821. [DOI] [PubMed] [Google Scholar]