

Abstract
The canal of Nuck is analogous to a patent processus vaginalis in a male, which normally loses its communication to the peritoneal cavity within the first year of life. Failure of obliteration of this tract can result in a hydrocele. We present a rare case of a 3-year-old girl with right-sided groin swelling over a year, diagnosed as hydrocele of canal of Nuck. Patient underwent surgical exploration and excision of hydrocelea. This entity should be considered in young females presenting with an inguinal swelling.
Keywords: Canal of Nuck, hydrocele, processus vaginalis
INTRODUCTION
In females, a peritoneal fold usually accompanies the round ligament as it descends into the labia major through the inguinal canal. Typically, this extension of peritoneum obliterates into a fibrous cord by the first year of life. Failure of obliteration results in a communication with the peritoneal cavity through a persistent Canal of Nuck resulting in inguinal hernia or hydrocele. This is analogous to a patent processus vaginalis in the male.
CASE REPORT
A 3-year-old girl presented to clinic with a nontender palpable swelling in the right inguinal region. On detailed history, the swelling had reduced in size over the past year with no further signs of any regression or progression in size. On physical examination, the swelling was nontender, cystic, and transilluminating. Patient underwent surgical exploration of the swelling through a right inguinal skin crease incision [Figure 1a and b]. After careful dissection through skin, subcutaneous tissues, Scarpa's fascia, and external oblique aponeurosis, the inguinal canal was exposed. The cystic swelling of the cord was identified and isolated. The swelling was confirmed to be an encysted hydrocele of cord with no evidence of associated inguinal hernia. After excision of hydrocele, the fibrous connection toward the deep inguinal ring was suture ligated and rest of the wound was closed in layers. Patient's postoperative follow-up at 6 weeks and 6 months revealed normally healed incision with no recurrence.
Figure 1.
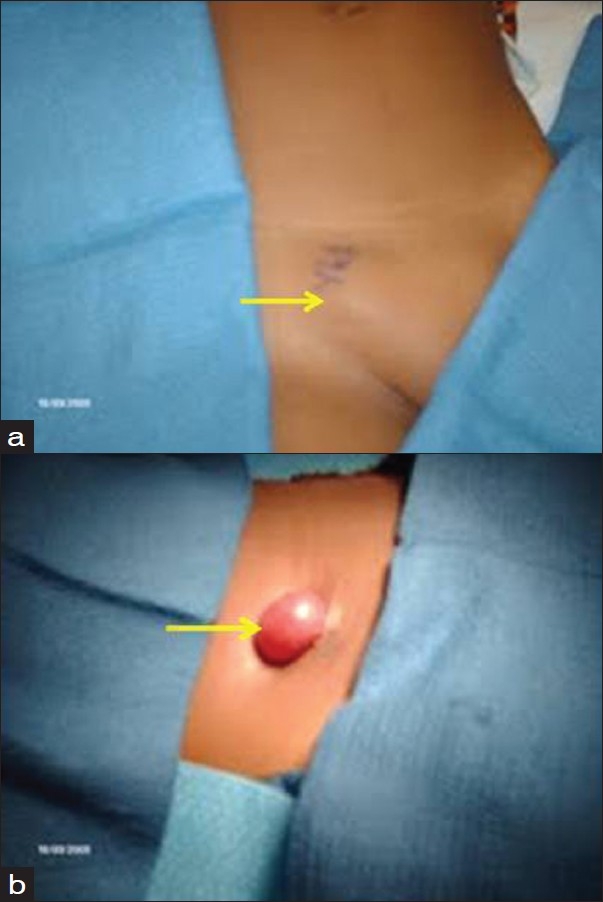
(a) Encysted hydrocele of canal of Nuck; (b) Operative finding—isolated cystic sac
DISCUSSION
During fetal development in the male, the testicle descends through the inguinal canal into the scrotum pulling along a sac-like extension of the peritoneum. By the first year of life, this extension condenses into a fibrous cord—the processus vaginalis, preventing the communication of peritoneal cavity with the scrotum. A thin membrane of this original extension remains surrounding the testicle which is named the tunica vaginalis. If this extension of peritoneum fails to close, based on the size of the defect, fluid or abdominal contents may enter the inguinal canal, resulting in a hydrocele or hernia. Congenital hernia or hydrocele, though more common in males, is rarely seen in females. In the female fetal development, round ligament of the uterus descends into the inguinal canal to the labium major. The peritoneal fold that descends the round ligament is named the canal of Nuck. If by the first year of life this communication fails to close, it can also result in an indirect hernia or a hydrocele.[1–3]
There are three types of a hydrocele of canal of Nuck. The most common type is one with no communication with peritoneal cavity forming an encysted hydrocele along the tract of descent, from the inguinal ring to the vulva. Second type results when there is a persistent communication with the peritoneal cavity. A third type is a combination of the two as a result of the inguinal ring constricting the hydrocele like a belt so that part is communicating and part is enclosed, giving this the name of hour glass type. However, any of these types of hydroceles are extremely rare in females.[4]
The differential diagnosis for an inguinal mass in a female includes indirect hernia, lymphadenopathy, Cold abscess, Bartholin's cyst, post-traumatic hematoma, rarely cystic lymphangioma, neuroblastoma metastasis in groin and ganglion.[1,5,6]
In conclusion, a hydrocele of the canal of Nuck though rare should be considered in the differential diagnosis in young females presenting with an inguinal swelling. Establishing a definitive diagnosis on clinical examination is challenging, radiological imaging may assist in diagnosis but surgical exploration is critical for final diagnosis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ortenberg J, Collins S, Roth CC. Pediatric Hydrocele and Hernia Surgery. [Last Updated on 2009 Sep 21]. Available from: http://emedicine.medscape.com/article/1015147-overview .
- 2.Park SJ, Lee HK, Hong HS, Kim HC, Kim DH, Park JS, et al. Hydrocele of the canal of Nuck in a girl: Ultrasound and MR appearance. Br J Radiol. 2004;77:243–4. doi: 10.1259/bjr/51474597. [DOI] [PubMed] [Google Scholar]
- 3.Jedrzejewski G, Stankiewicz A, Wieczorek AP. Uterus and ovary hernia of the canal of Nuck. Pediatr Radiol. 2008;38:1257–8. doi: 10.1007/s00247-008-0959-x. [DOI] [PubMed] [Google Scholar]
- 4.Counseller VS, Black BM. Hydrocele of the Canal of Nuck: Report of Seventeen Cases. Ann Surg. 1941;113:625–30. doi: 10.1097/00000658-194104000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Poenaru D, Jacobs DA, Kamal I. Unusual findings in the inguinal canal: A report of four cases. Pediatr Surg Int. 1999;15:515–6. doi: 10.1007/s003830050654. [DOI] [PubMed] [Google Scholar]
- 6.Pandit SK, Rattan KN, Budhiraja S, Solanki RS. Cystic lymphangioma with special reference to rare sites. Indian J Pediatr. 2000;67:339–41. doi: 10.1007/BF02820682. [DOI] [PubMed] [Google Scholar]