

A 70-year-old man presented at the emergency room with right-sided chest pain. The patient had known situs inversus totalis and dextrocardia, together with a 20-year history of type 2 diabetes mellitus. A right-sided electrocardiogram revealed 1-mm ST-segment elevation in the inferior leads. A chest radiograph confirmed dextrocardia and situs inversus. His troponin level was 8.1 ng/mL upon his admission to the emergency room. The patient was transferred to the cardiac catheterization laboratory for primary angioplasty. The door-to-balloon time was 75 minutes. The left coronary artery was engaged with a 6F Judkins left 4 diagnostic catheter without difficulty. The anatomic left anterior descending coronary artery displayed a 70% proximal lesion, followed by occlusion at the mid segment. The large diagonal coronary artery had a 60% stenosis at the proximal segment (Fig. 1). The left circumflex coronary artery was angiographically normal (Fig. 2).
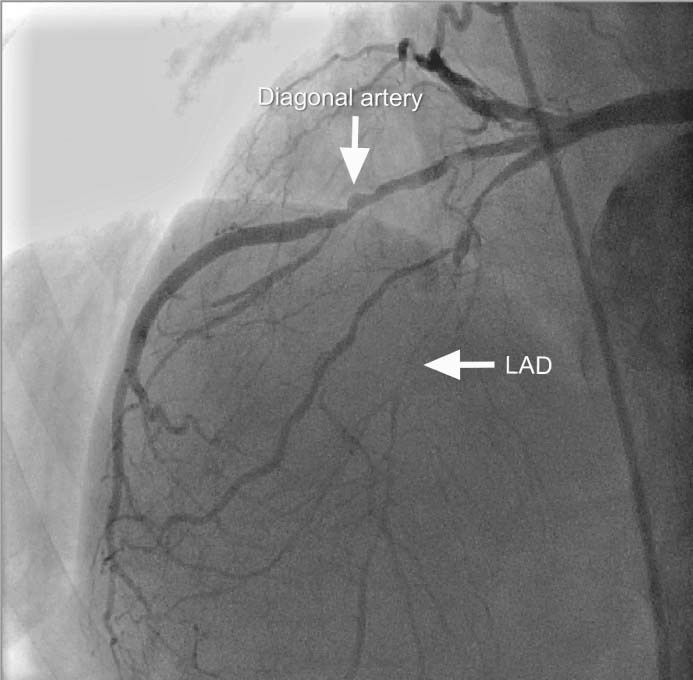
Fig. 1 Left coronary angiogram (right anterior oblique view) shows the occluded left anterior descending coronary artery (LAD) and a 60% stenosis of the diagonal artery.
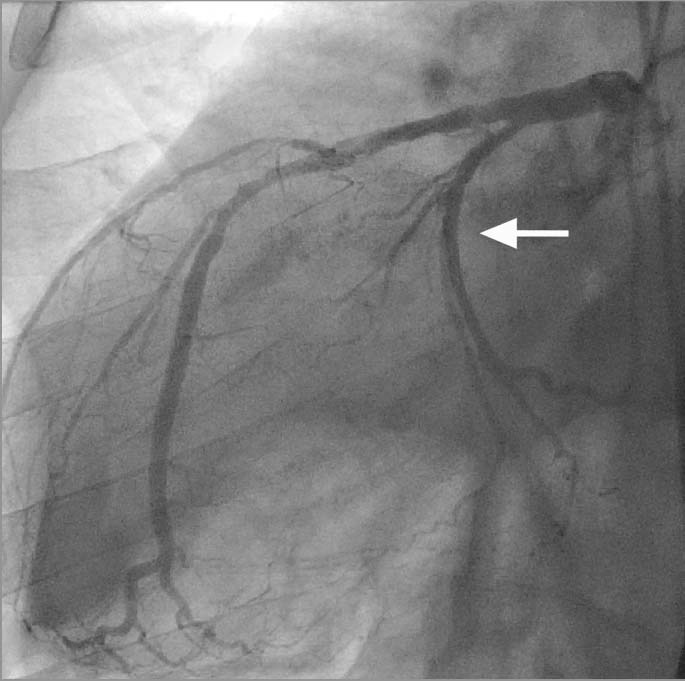
Fig. 2 Left coronary angiogram (left anterior oblique view) shows a normal left circumflex coronary artery (arrow).
An attempt was made to engage the right coronary artery (RCA) by counterclockwise rotation of a 6F Judkins right 4 diagnostic catheter, but the vessel was occluded and impassable at the proximal segment (Fig. 3). Therefore, a multipurpose catheter was used in the RCA as a guiding catheter. The RCA lesion was crossed with a floppy guidewire and dilated with a 2 × 20-mm semicompliant balloon catheter, after which a 3.5 × 18-mm stent was successfully deployed (Fig. 4).
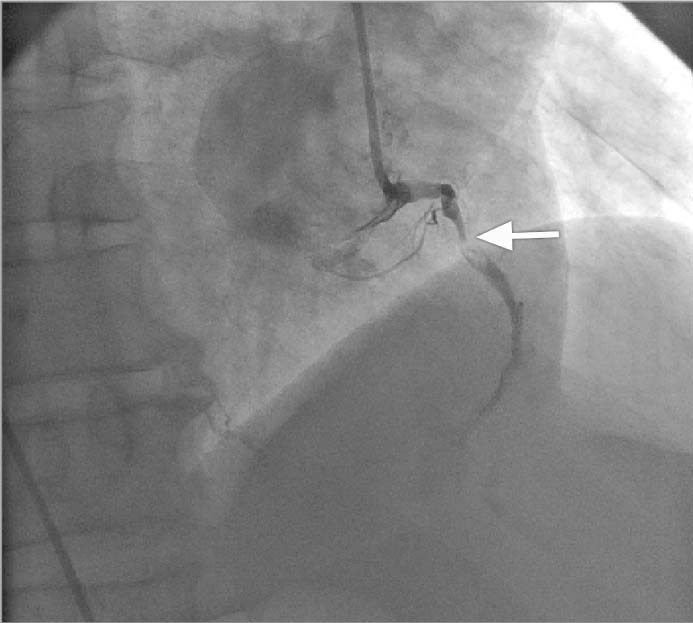
Fig. 3 Right coronary angiogram (right anterior oblique view) shows occluded right coronary artery (arrow).
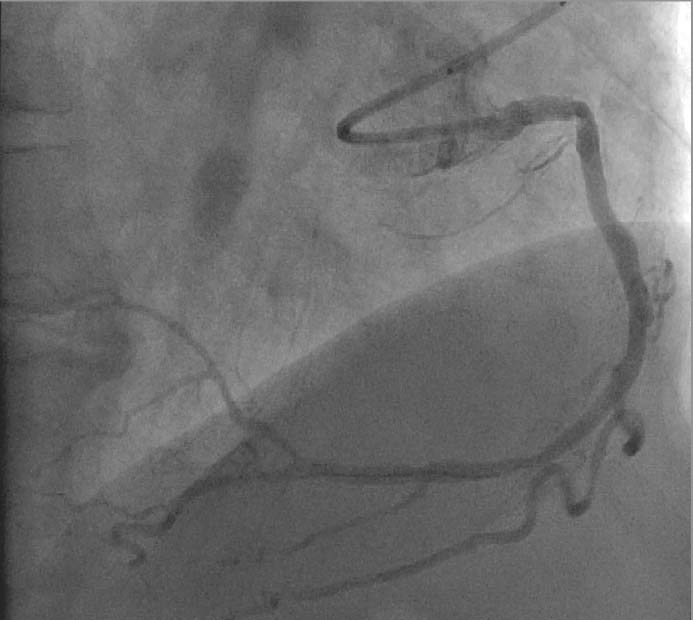
Fig. 4 Right coronary angiogram (right anterior oblique view) shows final result after stent deployment.
Comment
Situs inversus with dextrocardia is a rare congenital anomaly that occurs in approximately 1 per 10,000 individuals.1 Primary angioplasty can be technically difficult in patients with dextrocardia because mirror-image angulation is necessary during coronary angiography and percutaneous coronary intervention.2 Hence, the catheter manipulations should be opposite in direction from those applied to the normal cardiac anatomy (that is, counterclockwise rotation might be necessary to engage the RCA). In our patient, RCA cannulation was difficult both for diagnostic angiography and for angioplasty. For this reason, we used a multipurpose guiding catheter for the angioplasty. The technique of primary percutaneous coronary intervention in a patient with dextrocardia is rarely reported.3,4 Here, we report an instance of dextrocardia and multivessel coronary artery disease in a patient who presented with inferior-wall myocardial infarction and underwent successful primary angioplasty, with stenting of an occluded RCA.
Footnotes
Address for reprints: Sukru Aksoy, MD, Barbaros Mah. Veysi Pasa Sok. Atalar Sitesi 11. Blok D.13 Kosuyolu, 34662 Istanbul, Turkey
E-mail: drsukruaksoy@gmail.com
Section Editor: Raymond F. Stainback, MD, Department of Adult Cardiology, Texas Heart Institute at St. Luke's Episcopal Hospital, 6624 Fannin St., Suite 2480, Houston, TX 77030
References
- 1.Rosenberg HN, Rosenberg IN. Simultaneous association of situs inversus, coronary heart disease and hiatus hernia; report of a case and review of literature. Ann Intern Med 1949;30(4): 851–9. [DOI] [PubMed]
- 2.Shah RP, Lau KW. Coronary arteriography in the presence of dextrocardia and situs inversus. Ann Acad Med Singapore 1996;25(5):759–60. [PubMed]
- 3.Jauhar R, Gianos E, Bagai K, Roethel M, Kaplan BM. Primary angioplasty in a patient with dextrocardia. J Interv Cardiol 2005;18(2):127–30. [DOI] [PubMed]
- 4.Dhanjal TS, Davison P, Cotton JM. Primary percutaneous coronary intervention for acute myocardial infarction in a patient with dextrocardia. Cardiol J 2009;16(2):168–71. [PubMed]