

Introduction
Mirror movement refers to simultaneous contralateral, involuntary, identical movements that accompany voluntary movements. Erlenmeyer first used this term in 1879. The definition of mirror movement as involuntary, synkinetic mirror reversals of an intended movement of opposite side was coined by Cohen et al. in 1991.[1] These movements are soft, neurologic signs, seen uncommonly in clinical practice. Examination of patients for the presence or absence of mirror movements does not normally form part of a routine neurological assessment, but can give important clues in some cases.
Method of Examination
The examiner is required to observe both hands during voluntary fine finger movements of each hand in turn; e.g., sequentially pressing each finger against the thumb of one hand while the other hand is relaxed. Mirroring occurs when there are visible involuntary movements of the “relaxed” hand that appear to replicate the timing and type of movement being carried out by the voluntarily activated hand. These movements occur exclusively or predominantly in the hands, especially fingers. Distal movements mirror more strongly than the proximal ones. These movements are generally of lesser amplitude compared with voluntary activity. With efforts, there is increase in the mirror movements. Mirroring is generally more obvious on one side compared with the other. These movements can be partially suppressed.
Illustrative case
A 22-year-old lady was evaluated for writing funny’. While writing, her left hand mimicked the right. This had always been the case for her, a topic of jest for her sibs. Examination showed some limitation of neck movements, but she was otherwise normal. On asking to write, mirror movements were seen. As seen in the video, the left thumb movements are replications of the right and, on tapping, the left forefinger goes in synchronous movements. The comparatively proximal movement of pronation and supination mirrors minimally. The magnetic resonance imaging (MRI) [Figure 1] and computed tomography [Figure 2] confirmed complex craniovertebral anomaly consisting of blocked cervical vertebrae, atlantoaxial dislocation and minimal basilar invagination. This case illustrates mirror movements in craniovertebral anomaly.
Figure 1.

Magnetic resonance imaging of the cervical spine showing fusion of the C5,C6 vertebrae and basilar invagination
Figure 2.
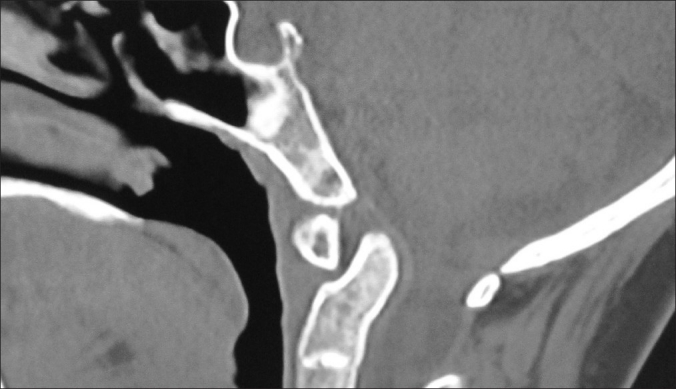
Computed tomography of the spine showing atlantoaxial dislocation
Pathophysiology
In a normal infant, there is tendency for movements of one limb to be accompanied by similar involuntary movement of the opposite limb. This tends to disappear before 10 years of age, coincident with myelination of corpus callosum. Persistence of this involuntary, synkinetic movement of one side of the body, usually the hands, which occurs as mirror reversal of movements of the opposite limb, is considered pathologic. Mirror activity is the electrical concomitant of mirror movements and has been observed in normal individuals during marked physical activity or with severe fatigue.
Gardner[2] has put forth his theory of physiological cross-talk via formation of false synapses (enlapses). It can be produced in the laboratory by mechanical pressure on a nerve (similar to the mechanism for hemifacial spasm), and proposed similar effects of hindbrain herniation on the pyramidal decussation. Schott and Wyke[3] proposed deficiencies in the pyramidal decussation at the brainstem level in particular, requiring development of alternate less-specific pathways, as one of the cause. Mirror movements in patients with dysgenetic or absent corpus callosum were attributed to deficient contralateral cortical inhibition. Farmer et al.[4] performed a detailed study using EMG and transcranial magnetic stimulation and concluded, based on timing, that the impulse for the movements arose from a single source and therefore indicated abnormal fibers with bilateral branching. These and few other theories in the persistence or occurrence of mirror movements are evolving in the era of functional imaging.
Clinical setting
Mirror movements have been described in association with several neurologic conditions like cerebral palsy, cervicomedullary junction anomaly (klippel Feil syndrome in particular),[4] cerebrovascular disease, Parkinson's disease,[5] certain symptomatic epilepsies, Friedreich's ataxia, phenylketonuria, amyotrophic lateral sclerosis,[6] Kallman's syndrome, high cervical spinal cord malformation, in association with alien hand syndrome (vascular lesion) and in certain psychiatric conditions like obsessive compulsive disorder and schizophrenia. Familial cases have been described with an autosomal-dominant or autosomal-recessive inheritance. DCC (deleted in colorectal cancer) is the receptor for netrin, a protein that guides axon migration of developing neurons across the body's midline. Mutations in the DCC gene were recently identified in two families with congenital mirror movements.[7]
Mirror box therapy
A mirror box is a box with two mirrors in the center (one facing each way), invented by Vilayanur S. Ramachandran, designed to alleviate phantom limb pain, in which patients keep having a feeling of presence of amputated limb. The patient places the good limb into one side and the stump into the other. The patient then looks into the mirror on the side with good limb and makes “mirror symmetric” movements as we do when we clap our hands. As the subject is seeing the reflected image of the good hand moving, it appears as if the phantom limb is also moving. Through the use of this artificial visual feedback, it becomes possible for the patient to “move” the phantom limb and to unclench it from potentially painful positions. The use of the mirror box has also been used in the rehabilitation of hemiparesis, or paralysis one side of the body, due to stroke.[8] complex regional pain syndrome and to rehabilition of spatial neglect.[9]
Mirror writing is an unusual script, in which the writing runs in the opposite direction to the normal with individual letters reversed so that it is most easily read using a mirror. This is seen in people having focal lesions affecting the left hemisphere, as has been documented with Leonardo da Vinci's famous mirror paintings.[10] Mirror writing is always undertaken with the left hand and in those whose languages are written leftwards.
Significance
Mirror movements are the soft neurological signs that are rarely encountered in routine clinical practice and are bound to be missed if not specifically sought for. Persistent movements warrant further investigations. Most familial and congenital mirror movement disorders improve with age. Patients having disabling symptoms interfering in daily activities should be offered training to reduce the severity. Evolution of advanced neuroimaging techniques such as functional MRI are providing us with exciting inputs that can used in developing newer treatment modalities like mirror therapy.
Videos Available Online
Footnotes
Source of Support: Nil,
Conflict of Interest: Nil
References
- 1.Cohen LG, Meer J, Tarkka I, Bierner S, Leiderman DB, Dubinsky RM, et al. Congenital Mirror Movements.Abnormal organization of motor pathway in two patients. Brain. 1991;114:381–403. doi: 10.1093/brain/114.1.381. [DOI] [PubMed] [Google Scholar]
- 2.Gardner WJ. Klippel-Feil syndrome, iniencephalus, anencephalus, hindbrain hernia and mirror movements: Over distension of the neural tube. Childs Brain. 1979;5:361–79. doi: 10.1159/000119832. [DOI] [PubMed] [Google Scholar]
- 3.Schott GD, Wyke MA. Congenital mirror movements. J Neurol Neurosurg Psychiatry. 1981;44:586–99. doi: 10.1136/jnnp.44.7.586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Farmer SF, Ingram DA, Stephens JA. Mirror movements studies in a patient with Klippel-Feil syndrome. J Physiol. 1990;428:467–84. doi: 10.1113/jphysiol.1990.sp018222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Espay AJ, Li JY, Johnston L, Chen R, Lang AE. Mirror movements in parkinsonism: Evaluation of a new clinical sign. J Neurol Neurosurg Psychiatry. 2005;76:1355–8. doi: 10.1136/jnnp.2005.062950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wittstock M, Meister S, Walter U, Benecke R, Wolters A. Mirror movements in amyotrophic lateral sclerosis. Amyotroph Lateral Scler. 2011;12:393–7. doi: 10.3109/17482968.2011.577223. [DOI] [PubMed] [Google Scholar]
- 7.Depienne C, Cincotta M, Billot S, Broachard V, Flamand C, Groppa S, et al. A novel DCC mutation and genetic heterogeneity in congenital mirror movements. Neurology. 2011;76:260–4. doi: 10.1212/WNL.0b013e318207b1e0. [DOI] [PubMed] [Google Scholar]
- 8.Altschuler EL, Wisdom SB, Stone L, Foster C, Galasko D, Llewellyn DM, et al. “Rehabilitation of hemiparesis after stroke with a mirror”. Lancet. 1999;353:2035–6. doi: 10.1016/s0140-6736(99)00920-4. [DOI] [PubMed] [Google Scholar]
- 9.Ramachandran VS, Altschuler EL, Stone L, Al-Aboudi M, Schwartz E, Siva N. “Can mirrors alleviate visual hemineglect?”. Medical Hypotheses. 1999;52:303–5. doi: 10.1054/mehy.1997.0651. [DOI] [PubMed] [Google Scholar]
- 10.Schott GD. Some neurological observations on Leonardo da Vinci's handwriting. J Neurol Sci. 1979;42:321–9. doi: 10.1016/0022-510x(79)90165-5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.