

Abstract
Background:
This prospective double-blind randomized study aims to study the hemodynamic changes following fluid preloading with Hydroxyethyl starch (HES) 6% (130/0.4) compared with normal saline (NS) in cardiac surgery patients.
Methods:
Forty patients undergoing coronary artery bypass grafting (CABG) were enrolled in this study, then they were divided in 2 equal groups, HES and NS. After fast administration of 10 mL/kg from either solutions over 5 min only, hemodynamic parameters, such as heart rate, mean arterial pressure (MAP), central venous pressure (CVP), pulmonary artery occlusion pressure (PAOP), mean pulmonary artery pressure, systemic vascular resistance, and pulmonary vascular resistance were measured every 5 min for the total duration of 40 minutes.
Results:
There were significant differences in the cardiac index measurements between both groups at 15 min onward; also PAOP was significantly higher in HES group at 10 min onward. CVP was higher in HES group but statistically significant at 10 min only. MAP was higher in HES group, but that was statistically significant at 40 min only. On the other hand PAP was significantly higher at 10 and 40 min.
Conclusion:
Fluid preloading with HES led to a significant increase in filling pressure of the left ventricle (PAOP) and cardiac index compared with NS. We believe that HES (130/0.4) could be a suitable solution for fluid preloading in CABG surgery patients. However, further studies are needed on different fluid preloading modalities with different dosing regimens.
Keywords: Cardiac surgery, hemodynamics, hydroxyethyl starch
INTRODUCTION
Proper volume management is important to maintain adequate cardiac output, tissue oxygenation, perfusion, and microcirculation in cardiac surgery patients. There is still a debate whether to administer crystalloids or colloids as preloading to improve the filling pressure. Crystalloid solution has to be given in a 4- to 5-fold amount compared with colloid to achieve similar circulatory effects. In an animal study, Otzuki et al. found an increase in tissue perfusion, oxygenation and better ventricular function with HES 6% compared with lactated ringer solution in a model of acute normovolemic hemodilution (ANH).[1]
The aim of this study is to evaluate the volume expansion secondary to preloading with either HES 6% or NS based on the measurement of hemodynamic parameters in CABG surgery patients.
No previous study in the literature was done with the same methodology, fast administration of HES 130/0.4, and assessing the effects on hemodynamics.
METHODS
After sample size calculation was done, ethics committee approval was obtained. Forty patients scheduled for CABG surgery were included after getting a written informed consent. Patient's randomization was computer generated. Inclusion criteria were:, CABG surgery patients with good left ventricular function. Exclusion criteria were: Patients with known hypersensitivity to HES, renal or hepatic disorders, coagulopathy, and redo-cardiac surgery.
In the operating room, a big lumen peripheral venous line, and an arterial line were inserted. Induction of anesthesia included: Midazolam 0.05–0.1 mg/kg, fentanyl 5–7 μg/kg, rocuronium 1 mg/kg, then maintenance of anesthesia was achieved with midazolam 14 μ/kg/h, fentanyl 2 μ/kg/h, and rocuronium 280 μ/kg/h. Afterwards, a pulmonary artery catheter and a triple lumen central venous catheter were inserted in the right internal jugular vein. Study solution was prepared and wrapped in a black cover by an assistant not contributing in the study, so that the investigator is blinded to the study solution. Ten milliliters per kilogram of either HES 6% or NS were infused over 5 minutes using a pressure bag. This dose was chosen because it is a fast infusion modality. After completing the infusion, readings of hemodynamic parameters were recorded every 5 min for the total duration of 40 min using continuous cardiac output Swan–Ganz catheter and monitor (Vigilance I, Edwards Life Science, CA, USA). During the study period, no additional fluids were infused. Student's t test was used to compare between the both groups, for different variables at different times. P<0.05 was considered statistically significant.
RESULTS
Demographic data of the patients in both groups are given in Table 1. The mean arterial pressure showed statistically significant difference between both groups at 40 min only (P<0.05). Central venous pressure was significantly higher in HES group at 10 min only, while PAP was significantly higher in HES group only at 40 min. PAOP was significantly higher in HES group at 10 min onward (P<0.05) [Figure 1]. Cardiac index was significantly higher in HES group at 15 min onward (P<0.05) [Figure 2]. There was no statistically significant difference between both groups regarding heart rate, systemic vascular resistance, and pulmonary vascular resistance.
Table 1.
Demographic data of the patients
Figure 1.
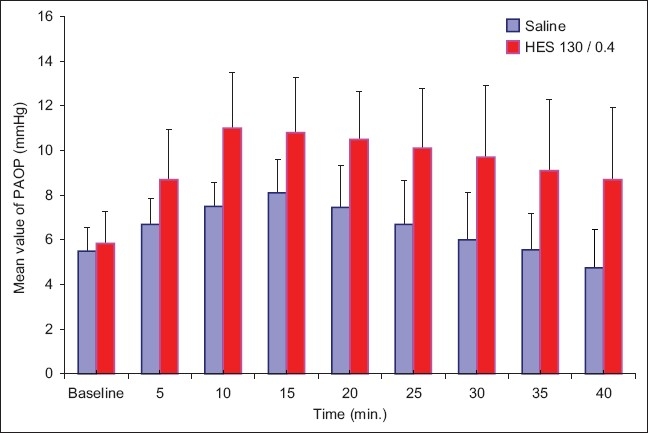
The mean values (mmHg) of pulmonary artery occlusion pressure (PAOP)
Figure 2.

The mean values (l/m2/min) of cardiac index (CI)
DISCUSSION
The significant increase of PAOP, which reflects filling pressure of the left ventricle, in the HES group denotes better improvement of the patient's volume status in this group. Moreover, the significant increase in cardiac index in the HES group is due to the improvement of PAOP, because other factors affecting it, as heart rate and systemic vascular resistance, did not change significantly.
In a study by Ickx et al., it was shown that administration of HES 130/0.4 or 200/0.5 in the setup of ANH led to a significant increase in PAOP but not CI.[2] Gallandt et al. compared the effects of HES 130/0.4 to HES 200/0.5 on hemodynamics, bleeding, and transfusion requirements in cardiac surgery, he showed that the hemodynamic parameters did not differ significantly between both HES groups, but HES 130/0.4 had less negative effect on hemostasis.[3]
In conclusion, HES 6% (130/0.4), led to a significant increase in cardiac index and filling pressure of the left ventricle compared to normal saline. We believe that preloading with HES precludes unstable hemodynamics in CABG surgical patients. However, further studies are needed on different fluid preloading modalities with different dosing regimens.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Otsuki DA, Fantoni DT, Margarido CB, Marumo CK, Intelizano T, Pasqualucci CA, et al. Hydroxyethyl starch is superior to Lactated Ringer as a replacement fluid in a pig model of acute normovolemic haemodilution. Br J Anaesth. 2007;98:29–37. doi: 10.1093/bja/ael312. [DOI] [PubMed] [Google Scholar]
- 2.Ickx BE, Bepperling F, Melot C, Schulman C, Van der Linden PJ. Plasma substitution effects of a new hydroxyethyl starch HES130/0.4 compared with HES 200/0.5 during and after extended acute normovolaemic haemodilution. Br J Anaesth. 2003;91:196–202. doi: 10.1093/bja/aeg159. [DOI] [PubMed] [Google Scholar]
- 3.Gallandat CG, Siemons AW, Baus D, Van Rooyen-Butijin WT, Haagenaars M, Van Oeveren W. A novel hydroxyethyl starch (Voluven®) for effective perioperative plasma volume substitution in cardiac surgery. Can J Anesth. 2000;47:1207–15. doi: 10.1007/BF03019870. [DOI] [PubMed] [Google Scholar]