

Abstract
Disruption of the distal tibiofibular syndesmosis is frequently accompanied by rotational ankle fracture such as pronation-external rotation and rarely occurs without ankle fracture. In such injury, not only inadequately treated or misdiagnosed cases, but also correctly diagnosed cases can possibly result in a chronic pattern which is more troublesome to treat than an acute pattern. This paper reviews anatomical and biomechanical characteristics of the distal tibiofibular joint, the mechanism of chronic disruption of the distal tibiofibular syndesmosis, radiological and arthroscopic diagnosis, and surgical treatment.
Keywords: Ankle, Chronic injury, Distal tibiofibular joint, Distal tibiofibular syndesmosis, Surgical treatment
ANATOMY AND BIOMECHANICS OF THE DISTAL TIBIOFIBULAR SYNDESMOSIS
The distal tibiofibular joint, which is formed by the distal fibula with convex configuration and the lateral side of the distal tibia with concave configuration, has been defined as a syndesmotic articulation with no articular cartilage. In spite of a small amount of motion, this joint has a very important role in ankle joint motion. In previous publications, the intermalleolar distance increases by approximately 1.5 mm through full plantar flexion to the dorsal flexed position of the ankle[1], and this widening is brought about by rotation, translation and migration of the fibula[1,2]. The fibula migrates distally and translates medially in plantar flexion and rotates laterally and migrates proximally in dorsal flexion to accommodate a wide anterior part of the talus into the widened space[1,2].
The distal tibiofibular syndesmosis contains 5 ligaments, the anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), interosseous ligament (IOL), transverse tibiofibular ligament (TTFL), and the posterior intermalleolar ligament (PIML). Although the fibula has no contact with the weight bearing area of the talus, approximately 16% of the weight is transmitted through the fibula because of these strong syndesmosis ligaments[3]. The AITFL and PITFL have a role in holding the fibula tight to the tibia. The IOL represents the thickened distal part of the interosseous membrane[4] and the role of this ligament is still controversial[5-7]. Although Outland described this ligament as “the chief bond between the two bones”[5], some investigators have reported that this ligament was weaker than the AITFL and PITFL[6]. On the other hand, recent biomechanical experience has confirmed more stiffness and failure load of the IOL than those of the AITFL[7]. The TTFL is considered to be distal or located in a deep part of the PITFL and forms a part of the articular surface for the talus. This ligament deepens the articular surface of the distal tibia and prevents posterior translation of the talus. Although the PIML has been neglected in the anatomy literature, the existence of this ligament has been revealed recently to be a cause of posterior impingement syndrome which brings about posterolateral ankle pain during plantar flexion[8]. Furthermore, radiological study has demonstrated this ligament to be an almost invariably present anatomical entity[9-11], however, its anatomical role is still unknown.
RELATIONSHIP BETWEEN DIASTASIS OF THE DISTAL TIBIOFIBULAR SYNDESMOSIS AND MEDIAL STRUCTURES
Several cadaveric studies revealed the effect of disrupted medial structures of the ankle joint in diastasis of the distal tibiofibular syndesmosis[1,12-15]. Close sectioning of all the ligaments of the syndesmosis in the cadaver study showed that there was only a 2 mm widening of the mortise, however, when section of the deep deltoid ligament was added, the widening of the mortise reached up to 3.7 mm[1]. Rasmussen et al[12] performed complete cutting of the distal tibiofibular ligaments, which resulted in only minor abnormality in motion, however, external rotation was greatly increased by further cutting of the anterior part of the deltoid ligament. Boden et al[13] created two groups of the pronation-external rotation model which included disruption of the syndesmosis and interosseous membrane up to the level of the fibular fracture with different injury of medial structures. Group I mimicked rupture of the deltoid ligament and Group II mimicked internally fixed medial malleolus after fracture. Although Group II showed only minimum widening of the syndesmosis (1.4 ± 0.3 mm), Group I showed progressive widening of the syndesmosis (from 0.5 to 4.5 mm) as the level of disruption of the interosseous membrane increased from 1.5 to 15 cm proximal to the ankle[13]. Michelson and Waldman reported no significant change in motion of the talus even if there was a fibular fracture 4 cm above the plafond and disruption of the syndesmosis to 6 cm. When section of the deep deltoid ligament was added, the ankle dislocated in plantar flexion[14].
Although these studies did not reproduce exactly the condition of real ankle injury, the common results of these studies imply the involvement of medial structures, especially the deltoid ligament which is difficult to repair rigidly compared to the medial malleolar fracture on which it is possible to perform rigid internal fixation, to prevent diastasis of the distal tibiofibular syndesmosis. Burns et al[15] revealed in their cadaver study that there was a 39% reduction in the tibiotalar contact area and a 42% increase in the peak contact pressure in complete disruption of the syndesmosis with the addition of deltoid ligament sectioning.
MECHANISM OF INJURY
Although the mechanism of injury in the distal tibiofibular syndesmosis remains unclear, the correlation of external rotation force to the foot has been considered as a common mechanism[4,16]. This injury is accompanied frequently by some types of rotational ankle fracture such as pronation-external rotation and pronation-abduction fracture, and supination-external rotation fracture less frequently according to the Lauge-Hansen classification. Furthermore, rotational ankle injury with high fibular fracture which was named “Maisonneuve fracture” is well known to have a high complication rate[17,18]. In the case of acute syndesmosis injury, syndesmosis screw fixation continues to be a commonly used therapeutic option, and good results have been reported in several studies[4,16,19], although there are several controversies regarding the number, size, position and necessity for removal[4,16,19]. Recently, this information and the diagnostic methods for acute syndesmosis injury have been widely reported, however, there are still inadequately treated or misdiagnosed cases which result in a chronic pattern[20-24]. Furthermore, a recent study has reported that even if complicated syndesmosis injury had been diagnosed correctly and treated by means of syndesmosis screw fixation in an acute phase, malreduction of the tibiofibular syndesmosis could occur, which would also result in a chronic pattern[25].
The injury of distal tibiofibular syndesmosis without fracture has been rarely reported[26-31]. Edwards and DeLee described ankle diastasis without fracture in detail[26]. They defined “sprain” as tenderness over the deltoid and anterior syndesmosis ligaments but an intact deltoid ligament, and “diastasis” as similar tenderness with rupture of the deltoid and syndesmosis ligaments[26]. These were differentiated using stress roentgenography with external rotation and abduction stress[26]. Furthermore, they classified “diastasis” under two general types, one was latent diastasis which could not be diagnosed by routine radiographs but showed diastasis using stress radiography, and the other was frank diastasis which showed visible diastasis using routine radiography[26]. These injuries may be considered as slight injuries because radiography shows no fracture, however, if these injuries are misdiagnosed or inadequately treated, there is a possibility of advancement to a chronic pattern which is more troublesome to treat than an acute pattern.
CLINICAL SYMPTOMS
Patients with chronic disruption of the distal tibiofibular syndesmosis generally have persistent pain on weight bearing after their initial injuries of the ankle[21-23]. Pain is aggravated by a combination of dorsiflexion and external rotation force which enables the distal tibiofibular joint to stretch[22]. These patients also complain of instability of the syndesmosis as a giving way, especially when walking on uneven ground[32]. Physical examination generally reveals persistent swelling at the anterolateral region of the syndesmosis and restricted dorsiflexion of the talocrural joint[21-23].
DIAGNOSIS
Manual stress test
Hopkinson et al[29] reported on the efficacy of the squeeze test which could clinically diagnose syndesmosis sprain. The squeeze test was considered positive when compression of the fibula to the tibia above the midpoint of the calf produced distal pain in the area of the interosseous ligament or its supporting structures[29]. Biomechanical analysis confirmed motion at the distal tibiofibular joint by compressing the calf, and considered the cause of pain noted during a positive squeeze test, as tension in the remaining fibers of the syndesmosis ligament as the distal fibula moved away from the distal tibia[33]. Boytim et al[28] diagnosed syndesmotic ankle sprains by applying an external rotation stress test. This test was performed by applying an external rotation stress to the affected foot and ankle with the knee held at 90° of flexion and the ankle in a neutral position[28]. A positive test produced pain over the anterior or posterior tibiofibular ligament and over the interosseous membrane[28]. Ogilvie-Harris and Reed performed not only an external rotation stress test, but also a fibular translation test, which attempted to translate the fibula on the tibia in the anterior-posterior plane by grasping the fibula and the tibia directly to diagnose disruption of the ankle syndesmosis[34]. However, according to an evaluation by Beumer et al[35], these manual tests were not uniformly positive in chronic syndesmosis injury. Some investigators have reported on the usefulness of stress radiography to diagnose syndesmotic injury[36-38]. Recent studies have applied gravity stress to radiography to detect occult disruption of the deltoid ligament which may be accompanied by supination-external rotation fibular fracture[36,37]. Stoffel et al[38] compared the external rotation stress with the lateral stress in their cadaveric study to evaluate which stress was superior in detecting syndesmotic injury, and concluded that the lateral stress was the superior stress direction. However, these stress tests have practical difficulties as the procedures need sufficient anesthesia and are rarely used clinically.
Radiography
Generally, antero-posterior (AP), lateral and mortise views are evaluated for ankle disorders during radiographic examination, and three radiographic parameters have been established to evaluate diastasis of the distal tibiofibular joint: tibiofibular clear space[39,40], tibiofibular overlap[39,40] and medial clear space[41]. Tibiofibular clear space is the distance from the lateral border of the posterior malleolus in the distal tibia to the medial border of the fibula[39,40]. The measurement of this distance is performed at 1 cm above the plafond on AP and mortise views and defined as normal if the measurement is less than approximately 6 mm on both views[39]. Tibiofibular overlap is the distance from the medial border of the fibula to the lateral border of the anterior tibial prominence[39,40]. Although the measurement of this distance is also performed at the same level and using the same views as the tibiofibular clear space, normal criteria are different between these two views. On AP view, the measurement is defined as normal if the distance is greater than approximately 6 mm or 42% of fibular width[40]. On mortise view, the measurement is defined as normal if the distance is greater than approximately 1 mm[39]. Medial clear space is the distance from the lateral border of the medial malleolus to the medial border of the talus at the level of the talar dome on the mortise view, and the measurement of this distance is defined as abnormal if it is greater than 4 mm[41]. Another criterion often used, is whether the medial clear space is equal to or less than the superior clear space, which is the distance between the talar dome and the tibial plafond[41]. Although these three parameters are applied clinically, there is still controversy regarding the reliability of these parameters[41-43]. Pneumaticos et al[42] performed a cadaver study and concluded that the tibiofibular clear space on the AP view was the most reliable parameter because this parameter did not change significantly with rotation compared with tibiofibular overlap and medial clear space. On the other hand, Beumer et al[41] showed no optimal radiographic parameter which could assess syndesmotic integrity and tibiofibular overlap, and a comparison between medial and superior clear space was found to be the most useful in their cadaver study. Furthermore, Nielson et al[43] evaluated the accuracy of these parameters by means of magnetic resonance imaging (MRI), and observed no association between the tibiofibular clear space and overlap measurements on radiographs with syndesmotic injury on MRI. They emphasized the importance of a medial clear space greater than 4 mm to diagnose disruption of the deltoid and the distal tibiofibular ligaments[43].
Other radiological methods
Because of the controversial reliability of radiological parameters to diagnose disruption of the distal tibiofibular syndesmosis, other radiological assessments have been used[44-46]. Computed tomography (CT) scanning is more sensitive than radiography for detecting the minor degrees of syndesmotic injuries[44]. Furthermore, recent reports have revealed the diagnostic value of MRI for disruption of the distal tibiofibular syndesmosis[45,46]. Oae et al[45] demonstrated the efficacy of MRI in diagnosing injury of the tibiofibular syndesmosis, which had a sensitivity of 100% and a specificity of 94% for the diagnosis of AITFL disruption, and a sensitivity of 100% and a specificity of 100% for the diagnosis of PITFL disruption. Han et al[46] showed a sensitivity of 90.0% and a specificity of 94.8% for MRI in the diagnosis of chronic syndesmosis injury. Following these recent studies[44-46], CT and MRI have now replaced radiographic assessment in the preoperative diagnosis of chronic disruption of the distal tibiofibular syndesmosis.
Arthroscopy
Arthroscopic examination is very useful for the diagnosis of chronic disruption of the distal tibiofibular syndesmosis because it permits not only direct visualization of disrupted AITFL, PITFL and transverse ligament, but also direct visualization of instability by applying stress force to the ankle during examination[34,47,48]. Even in cases with the diagnosis of chronic disruption of the distal tibiofibular syndesmosis by radiological assessment, we routinely perform arthroscopic assessment at the same time as surgery to confirm the diagnosis directly. However, we have never performed arthroscopy alone as an examination to confirm the findings of other radiological examinations. For direct visualization, we use the anterolateral and anteromedial portal. The anteromedial portal is more suitable for best visualization of the disrupted AITFL, while the anterolateral portal is more suitable for the disrupted PITFL. To confirm instability of the distal tibiofibular syndesmosis, a stress test is performed by moving the ankle from the neutral position to external rotation. We consider that instability is present if an opening of 2 mm can be identified by rotation stress[47,48]. Arthroscopic assessment also provides information on the volume of the fibrous tissue which is interposed in the distal tibiofibular joint, and which should be debrided prior to open surgery. Furthermore, other intra-articular disorders such as osteochondral injury or synovitis which may accompany chronic disruption of the distal tibiofibular syndesmosis can be accessed and treated simultaneously. We consider arthroscopic examination to be the most reliable method for diagnosing disruption of the distal tibiofibular syndesmosis (Figure 1).
Figure 1.
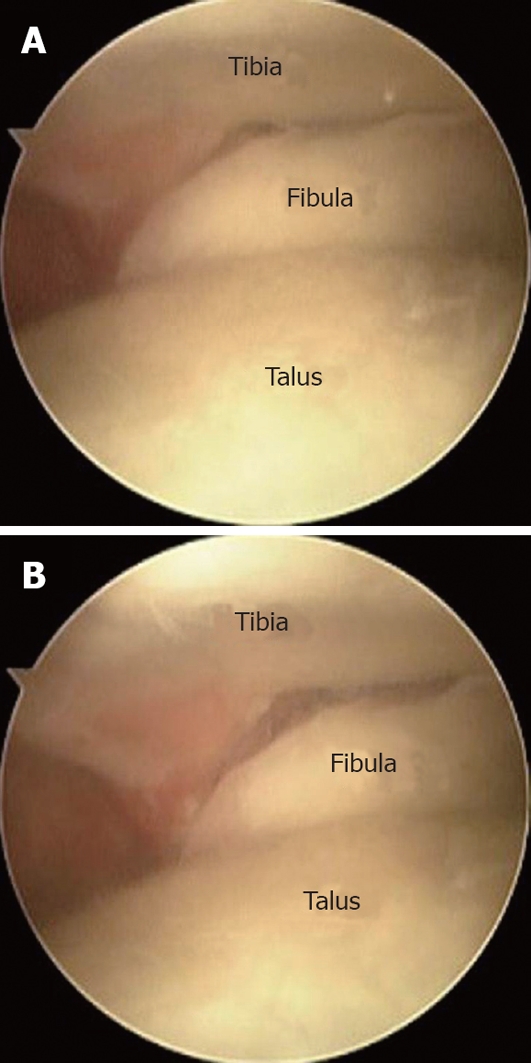
Arthroscopic findings of the anterior tibiofibular space in the neutral position (A) and under external rotation stress (B), which shows a widening of the anterior tibiofibular space of more than 2 mm.
Treatment
The symptoms caused by disruption of the distal tibiofibular syndesmosis may be controlled, to some degree, by conservative therapy, however, patients who do not respond to such therapy require surgical intervention. Although several techniques had been reported in previous publications[49-58], there is still no gold standard for the management of chronic disruption of the distal tibiofibular syndesmosis. Beals and Manoli reported a case of late syndesmosis disruption after rotational ankle fracture, and a good prognosis was achieved by debridement of the distal tibiofibular joint and medial gutter accompanied by syndesmosis screw fixation[49]. A similar technique was used by Harper, who performed syndesmosis screw fixation with or without syndesmosis debridement in 6 patients with chronic disruption after pronation - external rotation stage 4 fracture[50]. As an additional procedure at surgery, arthrodesis of the tibiofibular interval was performed in a patient due to residual incongruity[50]. In this series, 4 of 6 patients were completely satisfied by this procedure[50]. A recent report also demonstrated the efficacy of arthroscopic debridement of the distal tibiofibular syndesmosis and medial gutter with percutaneous fixation of the syndesmosis using screws as a less invasive technique[51].
Using another method, Beumer et al[52] introduced a medialized advancement of the insertion of the AITFL on the tibia with a bone block to tense a slack but continuous AITFL. During this procedure, syndesmosis screw fixation was added after fixation of the bone block using a small screw[52]. Mosier-LaClair et al[53] recommended syndesmosis screw fixation and repair of the AITFL using two suture anchors for late reconstruction of the distal tibiofibular joint. These techniques seem to be indicated for patients with continuous AITFL, but are not indicated for patients with attenuated or ruptured AITFL.
On the other hand, some reconstructive surgeries using local or free autogenous substitute have been reported[54,55]. Grass et al[54] reconstructed not only the AITFL and PITFL, but also the IOL using a split autologous peroneus longus tendon graft for chronic instability of the distal tibiofibular syndesmosis, and reported pain relief in 15 of 16 cases treated using this procedure. Morris et al[55] harvested a free hamstring autograft for reconstruction of the AITFL and IOL in the distal tibiofibular syndesmosis. They performed this procedure for 8 patients with chronic syndesmotic instability after ankle fracture in 4 patients, isolated injuries with no fracture in 2 patients and without obvious trauma in 2 patients, and all patients achieved good clinical results[55]. Although these two reports commonly emphasized the importance of reconstructing the IOL[54,55], there is still no clear evidence on which ligament should be reconstructed. Furthermore, no studies have examined the optimal substitute for such reconstructive surgery.
Some authors have recommended arthrodesis of the distal tibiofibular joint for chronic cases[56-58]. Katznelson et al[56] performed arthrodesis of the distal tibiofibular joint in 5 patients, 4 of whom were pain-free and achieved a full range of motion of the ankle joint at one year after surgery. Espinosa et al[57] defined a chronic syndesmosis injury as persistent syndesmotic widening 3 months after injury and recommended open arthrodesis for such cases. Pena and Coetzee[58] suggested arthrodesis for cases with significant incongruity evaluated by CT at more than 6 mo after initial injury. They stated as the author’s perception that final ankle function was definitely not sufficient to maintain an active athletic life[58]. It is unclear whether obliteration of distal tibiofibular joint motion will deteriorate ankle joint function in the future as there is no report which shows the clinical and functional results of arthrodesis of the distal tibiofibular joint after long term follow up.
Although each type of surgery has achieved good outcome and prognosis in previous publications[49-58], there are still some problems to be solved in order to establish a gold standard for the surgical management of chronic disruption of the distal tibiofibular joint.
Footnotes
Peer reviewers: Florian Kutscha-Lissberg, MD, Department for Trauma Surgery, Medical University of Vienna, Währinger Gürtel 18-20, A-1090 Vienna, Austria; Nelson F SooHoo, MD, Associate Professor, Department of Orthopaedic Surgery, UCLA School of Medicine, 10945 Le Conte Ave., Rm 3355 PVUB, Los Angeles, CA 90095, United States
S- Editor Cheng JX L- Editor Webster JR E- Editor Lin YP
References
- 1.Close JR. Some applications of the functional anatomy of the ankle joint. J Bone Joint Surg Am. 1956;38-A:761–781. [PubMed] [Google Scholar]
- 2.Weinert CR Jr, McMaster JH, Ferguson RJ. Dynamic function of the human fibula. Am J Anat. 1973;138:145–149. doi: 10.1002/aja.1001380202. [DOI] [PubMed] [Google Scholar]
- 3.Lambert KL. The weight-bearing function of the fibula. A strain gauge study. J Bone Joint Surg Am. 1971;53:507–513. [PubMed] [Google Scholar]
- 4.Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007;15:330–339. doi: 10.5435/00124635-200706000-00002. [DOI] [PubMed] [Google Scholar]
- 5.Outland T. Sprains and separations of the inferior tibiofibular joint without important fracture. Am J Surg. 1943;59:320–329. [Google Scholar]
- 6.Ogilvie-Harris DJ, Reed SC, Hedman TP. Disruption of the ankle syndesmosis: biomechanical study of the ligamentous restraints. Arthroscopy. 1994;10:558–560. doi: 10.1016/s0749-8063(05)80014-3. [DOI] [PubMed] [Google Scholar]
- 7.Hoefnagels EM, Waites MD, Wing ID, Belkoff SM, Swierstra BA. Biomechanical comparison of the interosseous tibiofibular ligament and the anterior tibiofibular ligament. Foot Ankle Int. 2007;28:602–604. doi: 10.3113/FAI.2007.0602. [DOI] [PubMed] [Google Scholar]
- 8.Hamilton WG. Foot and ankle injuries in dancers. Clin Sports Med. 1988;7:143–173. [PubMed] [Google Scholar]
- 9.Rosenberg ZS, Cheung YY, Beltran J, Sheskier S, Leong M, Jahss M. Posterior intermalleolar ligament of the ankle: normal anatomy and MR imaging features. AJR Am J Roentgenol. 1995;165:387–390. doi: 10.2214/ajr.165.2.7618563. [DOI] [PubMed] [Google Scholar]
- 10.Oh CS, Won HS, Hur MS, Chung IH, Kim S, Suh JS, Sung KS. Anatomic variations and MRI of the intermalleolar ligament. AJR Am J Roentgenol. 2006;186:943–947. doi: 10.2214/AJR.04.1784. [DOI] [PubMed] [Google Scholar]
- 11.Boonthathip M, Chen L, Trudell DJ, Resnick DL. Tibiofibular syndesmotic ligaments: MR arthrography in cadavers with anatomic correlation. Radiology. 2010;254:827–836. doi: 10.1148/radiol.09090624. [DOI] [PubMed] [Google Scholar]
- 12.Rasmussen O, Tovborg-Jensen I, Boe S. Distal tibiofibular ligaments. Analysis of function. Acta Orthop Scand. 1982;53:681–686. doi: 10.3109/17453678208992276. [DOI] [PubMed] [Google Scholar]
- 13.Boden SD, Labropoulos PA, McCowin P, Lestini WF, Hurwitz SR. Mechanical considerations for the syndesmosis screw. A cadaver study. J Bone Joint Surg Am. 1989;71:1548–1555. [PubMed] [Google Scholar]
- 14.Michelson JD, Waldman B. An axially loaded model of the ankle after pronation external rotation injury. Clin Orthop Relat Res. 1996:285–293. doi: 10.1097/00003086-199607000-00043. [DOI] [PubMed] [Google Scholar]
- 15.Burns WC 2nd, Prakash K, Adelaar R, Beaudoin A, Krause W. Tibiotalar joint dynamics: indications for the syndesmotic screw--a cadaver study. Foot Ankle. 1993;14:153–158. doi: 10.1177/107110079301400308. [DOI] [PubMed] [Google Scholar]
- 16.Dattani R, Patnaik S, Kantak A, Srikanth B, Selvan TP. Injuries to the tibiofibular syndesmosis. J Bone Joint Surg Br. 2008;90:405–410. doi: 10.1302/0301-620X.90B4.19750. [DOI] [PubMed] [Google Scholar]
- 17.Pankovich AM. Maisonneuve fracture of the fibula. J Bone Joint Surg Am. 1976;58:337–342. [PubMed] [Google Scholar]
- 18.Merrill KD. The Maisonneuve fracture of the fibula. Clin Orthop Relat Res. 1993:218–223. [PubMed] [Google Scholar]
- 19.van den Bekerom MP, Raven EE. Current concepts review: operative techniques for stabilizing the distal tibiofibular syndesmosis. Foot Ankle Int. 2007;28:1302–1308. doi: 10.3113/FAI.2007.1302. [DOI] [PubMed] [Google Scholar]
- 20.Beals TC, Manoli A 2nd. Late syndesmosis reconstruction: a case report. Foot Ankle Int. 1998;19:485–488. doi: 10.1177/107110079801900712. [DOI] [PubMed] [Google Scholar]
- 21.Harper MC. Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int. 2001;22:15–18. doi: 10.1177/107110070102200103. [DOI] [PubMed] [Google Scholar]
- 22.Grass R, Rammelt S, Biewener A, Zwipp H. Peroneus longus ligamentoplasty for chronic instability of the distal tibiofibular syndesmosis. Foot Ankle Int. 2003;24:392–397. doi: 10.1177/107110070302400503. [DOI] [PubMed] [Google Scholar]
- 23.Morris MW, Rice P, Schneider TE. Distal tibiofibular syndesmosis reconstruction using a free hamstring autograft. Foot Ankle Int. 2009;30:506–511. doi: 10.3113/FAI.2009.0506. [DOI] [PubMed] [Google Scholar]
- 24.Schuberth JM, Jennings MM, Lau AC. Arthroscopy-assisted repair of latent syndesmotic instability of the ankle. Arthroscopy. 2008;24:868–874. doi: 10.1016/j.arthro.2008.02.013. [DOI] [PubMed] [Google Scholar]
- 25.Gardner MJ, Demetrakopoulos D, Briggs SM, Helfet DL, Lorich DG. Malreduction of the tibiofibular syndesmosis in ankle fractures. Foot Ankle Int. 2006;27:788–792. doi: 10.1177/107110070602701005. [DOI] [PubMed] [Google Scholar]
- 26.Edwards GS Jr, DeLee JC. Ankle diastasis without fracture. Foot Ankle. 1984;4:305–312. doi: 10.1177/107110078400400606. [DOI] [PubMed] [Google Scholar]
- 27.Marymont JV, Lynch MA, Henning CE. Acute ligamentous diastasis of the ankle without fracture. Evaluation by radionuclide imaging. Am J Sports Med. 1986;14:407–409. doi: 10.1177/036354658601400514. [DOI] [PubMed] [Google Scholar]
- 28.Boytim MJ, Fischer DA, Neumann L. Syndesmotic ankle sprains. Am J Sports Med. 1991;19:294–298. doi: 10.1177/036354659101900315. [DOI] [PubMed] [Google Scholar]
- 29.Hopkinson WJ, St Pierre P, Ryan JB, Wheeler JH. Syndesmosis sprains of the ankle. Foot Ankle. 1990;10:325–330. doi: 10.1177/107110079001000607. [DOI] [PubMed] [Google Scholar]
- 30.Taylor DC, Englehardt DL, Bassett FH 3rd. Syndesmosis sprains of the ankle. The influence of heterotopic ossification. Am J Sports Med. 1992;20:146–150. doi: 10.1177/036354659202000209. [DOI] [PubMed] [Google Scholar]
- 31.Miller CD, Shelton WR, Barrett GR, Savoie FH, Dukes AD. Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med. 1995;23:746–750. doi: 10.1177/036354659502300618. [DOI] [PubMed] [Google Scholar]
- 32.van den Bekerom MP, de Leeuw PA, van Dijk CN. Delayed operative treatment of syndesmotic instability. Current concepts review. Injury. 2009;40:1137–1142. doi: 10.1016/j.injury.2009.03.011. [DOI] [PubMed] [Google Scholar]
- 33.Teitz CC, Harrington RM. A biochemical analysis of the squeeze test for sprains of the syndesmotic ligaments of the ankle. Foot Ankle Int. 1998;19:489–492. doi: 10.1177/107110079801900713. [DOI] [PubMed] [Google Scholar]
- 34.Ogilvie-Harris DJ, Reed SC. Disruption of the ankle syndesmosis: diagnosis and treatment by arthroscopic surgery. Arthroscopy. 1994;10:561–568. doi: 10.1016/s0749-8063(05)80015-5. [DOI] [PubMed] [Google Scholar]
- 35.Beumer A, Swierstra BA, Mulder PG. Clinical diagnosis of syndesmotic ankle instability: evaluation of stress tests behind the curtains. Acta Orthop Scand. 2002;73:667–669. doi: 10.1080/000164702321039642. [DOI] [PubMed] [Google Scholar]
- 36.Gill JB, Risko T, Raducan V, Grimes JS, Schutt RC Jr. Comparison of manual and gravity stress radiographs for the evaluation of supination-external rotation fibular fractures. J Bone Joint Surg Am. 2007;89:994–999. doi: 10.2106/JBJS.F.01002. [DOI] [PubMed] [Google Scholar]
- 37.Schock HJ, Pinzur M, Manion L, Stover M. The use of gravity or manual-stress radiographs in the assessment of supination-external rotation fractures of the ankle. J Bone Joint Surg Br. 2007;89:1055–1059. doi: 10.1302/0301-620X.89B8.19134. [DOI] [PubMed] [Google Scholar]
- 38.Stoffel K, Wysocki D, Baddour E, Nicholls R, Yates P. Comparison of two intraoperative assessment methods for injuries to the ankle syndesmosis. A cadaveric study. J Bone Joint Surg Am. 2009;91:2646–2652. doi: 10.2106/JBJS.G.01537. [DOI] [PubMed] [Google Scholar]
- 39.Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989;10:156–160. doi: 10.1177/107110078901000308. [DOI] [PubMed] [Google Scholar]
- 40.Pettrone FA, Gail M, Pee D, Fitzpatrick T, Van Herpe LB. Quantitative criteria for prediction of the results after displaced fracture of the ankle. J Bone Joint Surg Am. 1983;65:667–677. [PubMed] [Google Scholar]
- 41.Beumer A, van Hemert WL, Niesing R, Entius CA, Ginai AZ, Mulder PG, Swierstra BA. Radiographic measurement of the distal tibiofibular syndesmosis has limited use. Clin Orthop Relat Res. 2004:227–234. doi: 10.1097/01.blo.0000129152.81015.ad. [DOI] [PubMed] [Google Scholar]
- 42.Pneumaticos SG, Noble PC, Chatziioannou SN, Trevino SG. The effects of rotation on radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle Int. 2002;23:107–111. doi: 10.1177/107110070202300205. [DOI] [PubMed] [Google Scholar]
- 43.Nielson JH, Gardner MJ, Peterson MG, Sallis JG, Potter HG, Helfet DL, Lorich DG. Radiographic measurements do not predict syndesmotic injury in ankle fractures: an MRI study. Clin Orthop Relat Res. 2005:216–221. doi: 10.1097/01.blo.0000161090.86162.19. [DOI] [PubMed] [Google Scholar]
- 44.Ebraheim NA, Lu J, Yang H, Mekhail AO, Yeasting RA. Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: a cadaver study. Foot Ankle Int. 1997;18:693–698. doi: 10.1177/107110079701801103. [DOI] [PubMed] [Google Scholar]
- 45.Oae K, Takao M, Naito K, Uchio Y, Kono T, Ishida J, Ochi M. Injury of the tibiofibular syndesmosis: value of MR imaging for diagnosis. Radiology. 2003;227:155–161. doi: 10.1148/radiol.2271011865. [DOI] [PubMed] [Google Scholar]
- 46.Han SH, Lee JW, Kim S, Suh JS, Choi YR. Chronic tibiofibular syndesmosis injury: the diagnostic efficiency of magnetic resonance imaging and comparative analysis of operative treatment. Foot Ankle Int. 2007;28:336–342. doi: 10.3113/FAI.2007.0336. [DOI] [PubMed] [Google Scholar]
- 47.Takao M, Ochi M, Naito K, Iwata A, Kawasaki K, Tobita M, Miyamoto W, Oae K. Arthroscopic diagnosis of tibiofibular syndesmosis disruption. Arthroscopy. 2001;17:836–843. doi: 10.1016/s0749-8063(01)90007-6. [DOI] [PubMed] [Google Scholar]
- 48.Takao M, Ochi M, Oae K, Naito K, Uchio Y. Diagnosis of a tear of the tibiofibular syndesmosis. The role of arthroscopy of the ankle. J Bone Joint Surg Br. 2003;85:324–329. doi: 10.1302/0301-620x.85b3.13174. [DOI] [PubMed] [Google Scholar]
- 49.Beals TC, Manoli A 2nd. Late syndesmosis reconstruction: a case report. Foot Ankle Int. 1998;19:485–488. doi: 10.1177/107110079801900712. [DOI] [PubMed] [Google Scholar]
- 50.Harper MC. Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int. 2001;22:15–18. doi: 10.1177/107110070102200103. [DOI] [PubMed] [Google Scholar]
- 51.Schuberth JM, Jennings MM, Lau AC. Arthroscopy-assisted repair of latent syndesmotic instability of the ankle. Arthroscopy. 2008;24:868–874. doi: 10.1016/j.arthro.2008.02.013. [DOI] [PubMed] [Google Scholar]
- 52.Beumer A, Heijboer RP, Fontijne WP, Swierstra BA. Late reconstruction of the anterior distal tibiofibular syndesmosis: good outcome in 9 patients. Acta Orthop Scand. 2000;71:519–521. doi: 10.1080/000164700317381243. [DOI] [PubMed] [Google Scholar]
- 53.Mosier-LaClair S, Pike H, Pomeroy G. Syndesmosis injuries: acute, chronic, new techniques for failed management. Foot Ankle Clin. 2002;7:551–565, ix. doi: 10.1016/s1083-7515(02)00022-0. [DOI] [PubMed] [Google Scholar]
- 54.Grass R, Rammelt S, Biewener A, Zwipp H. Peroneus longus ligamentoplasty for chronic instability of the distal tibiofibular syndesmosis. Foot Ankle Int. 2003;24:392–397. doi: 10.1177/107110070302400503. [DOI] [PubMed] [Google Scholar]
- 55.Morris MW, Rice P, Schneider TE. Distal tibiofibular syndesmosis reconstruction using a free hamstring autograft. Foot Ankle Int. 2009;30:506–511. doi: 10.3113/FAI.2009.0506. [DOI] [PubMed] [Google Scholar]
- 56.Katznelson A, Lin E, Militiano J. Ruptures of the ligaments about the tibio-fibular syndesmosis. Injury. 1983;15:170–172. doi: 10.1016/0020-1383(83)90007-4. [DOI] [PubMed] [Google Scholar]
- 57.Espinosa N, Smerek JP, Myerson MS. Acute and chronic syndesmosis injuries: pathomechanisms, diagnosis and management. Foot Ankle Clin. 2006;11:639–657. doi: 10.1016/j.fcl.2006.07.006. [DOI] [PubMed] [Google Scholar]
- 58.Peña FA, Coetzee JC. Ankle syndesmosis injuries. Foot Ankle Clin. 2006;11:35–50, viii. doi: 10.1016/j.fcl.2005.12.007. [DOI] [PubMed] [Google Scholar]