

Abstract
The calcifying epithelial odontogenic tumor is a rare benign odontogenic tumor that was first described by Pindborg in 1955. It accounts for less than 1% of all odontogenic neoplasms. The tumor is characterized histologically by the presence of polygonal epithelial cells, calcification, and eosinophilic deposits resembling amyloid. Noncalcifying Pindborg tumor is very rare and only three cases have been documented in the English language literature so far. We present an additional case of noncalcifying Pindborg tumor and review the previously reported cases. Because noncalcifying Pindborg tumor is believed to be an aggressive variant, a definitive resection of the tumor with tumor-free surgical margins and long-term follow-up is recommended.
Keywords: Amyloid, calcifications, mandible, odontogenic tumors, Pindborg tumor
INTRODUCTION
Calcifying epithelial odontogenic tumor (CEOT) or Pindborg tumor is a rare odontogenic neoplasm that was first described by Pindborg in 1955.[1] This benign tumor is reported to comprise less than 1% of all odontogenic neoplasms. The most common mode of presentation is as a slow-growing intraosseous mass in the mandible in the fourth to fifth decade of life. There is no gender predilection. The etiology is unknown, and no predisposing factors have been identified. Histopathology is the gold standard for diagnosis of CEOT. Characteristic features on histology are polygonal epithelial cells, calcification, and eosinophilic deposits resembling amyloid.[2] Noncalcifying Pindborg tumor is very rare, with only three cases reported in the English language literature to date.[3–5] We present an additional case of a noncalcifying Pindborg tumor, and highlight the atypical microscopic features of this rare tumor.
CASE REPORT
A 57-year-old man presented with history of difficulty in speaking for 1½ months. On radiographic examination, a unilocular lesion measuring 8 × 4 cm was found over the right lower jaw, involving the angle of mandible. His medical history and physical examination were noncontributory. On intraoral examination, there was no clinical expansion, discharge, or numbness. MRI [Figure 1] revealed a lesion in the right mandible involving the body and ramus.
Figure 1.
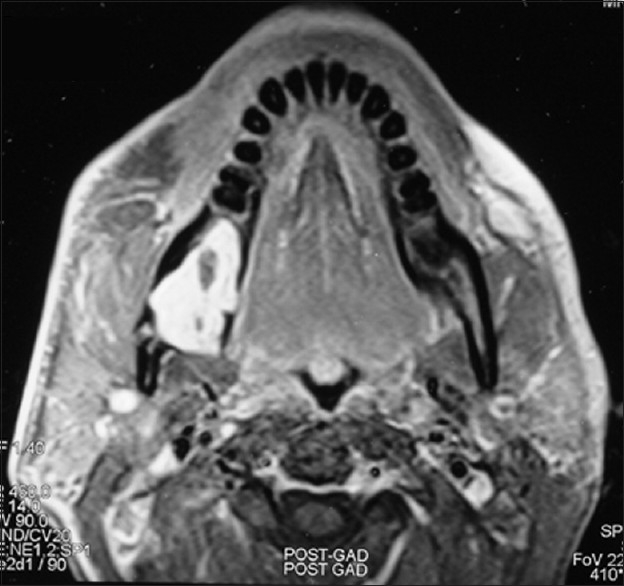
MRI showing the tumor in the right mandible
An incisional biopsy performed from the lesion revealed an epithelial odontogenic neoplasm composed of nests and islands of polygonal cells having centrally-placed nuclei and eosinophilic cytoplasm [Figure 2a]. Occasionally the cells formed a pseudoglandular pattern [Figure 2b]. The nuclei were vesicular and had inconspicuous nucleoli [Figure 2b]. Mitotic figures and areas of necrosis were not seen. Interspersed amidst the tumor cells was amorphous, acellular, eosinophilic, amyloid-like material, which showed metachromasia with crystal violet and green birefringence on Congo red staining [Figures 2c and 2d]. No areas of calcification were seen. On immunohistochemical evaluation, the tumor cells showed positivity for cytokeratin [Figure 3].
Figure 2.
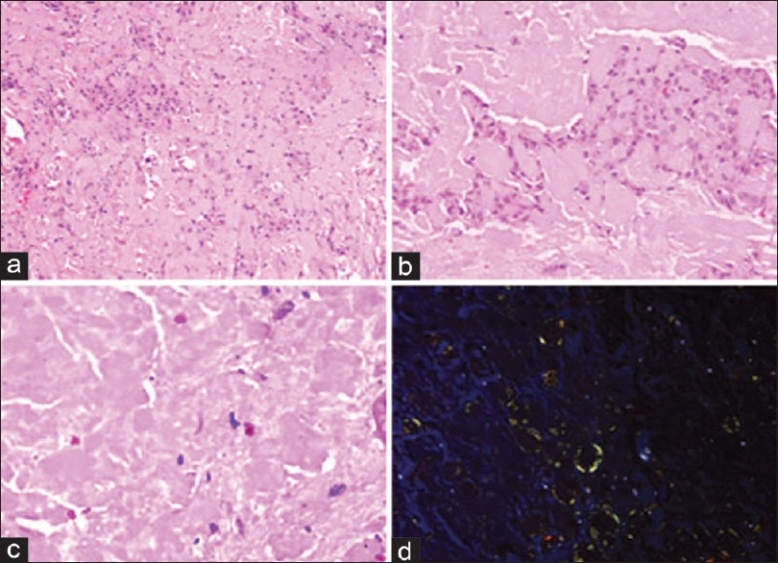
Photomicrograph showing polygonal epithelial cells amidst amyloid-like material; note the absence of calcification (a) (H and E, ×100). Cells showing pseudoglandular pattern (b) (hematoxylin and eosin; ×200). Higher magnification of amyloid-like material (c) (H and E, ×400). Congo red staining showing green birefringence of amyloid (d) (polarizing microscop, ×200)
Figure 3.
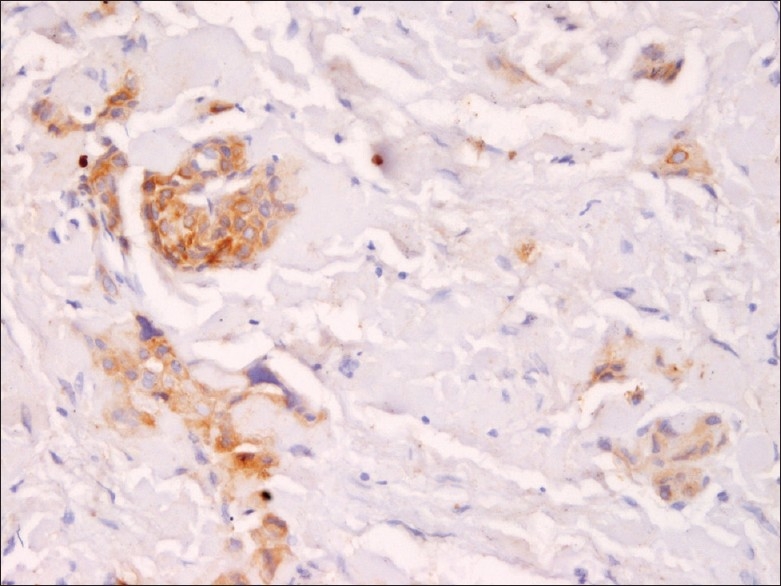
Photomicrograph showing immunopositivity of epithelial cells for cytokeratin (immunoperoxidase, ×200)
Based on the histological and immunohistochemical findings, a diagnosis of noncalcifying epithelial odontogenic tumor was suggested. The patient refused to undergo en bloc resection of the tumor. Excision of the lesion was therefore done and histopathology confirmed the diagnosis of noncalcifying CEOT. The patient continues to be on regular follow-up and the tumor has not recurred 1 year after excision.
DISCUSSION
Since its original description by Pindborg in 1955, the clinical features and histopathology of CEOT has been well described in literature.[6,7] Classically, CEOT presents as a painless slow-growing mass in the mandible. The mean age of presentation is 40 years, with equal incidence in men and women.[8] CEOT may present as an intraosseous (central) or extraosseous (peripheral) tumor.[8] Intraosseous CEOT is the more common type, accounting for more than 85% of the cases and presenting most commonly at the mandible. The incidence of extraosseous CEOT is reported to be about 6%. It occurs most commonly at the gingiva.[8] The presentation of both intraosseous and extraosseous types is similar and both have similar histological features. Radiologically, intraosseous CEOT shows radiolucent areas with occasional calcification, while the extraosseous type shows bone erosion near the tumor.[9] The histogenesis of the intraosseous tumor is believed to be from the stratum intermedium of enamel, whereas the extraosseous type is derived from dental lamina epithelial rests or the basal cells of gingival epithelium.[2] Intraosseous CEOT is more aggressive, with a reported recurrence rate of 14%.[9]
Histopathologically, CEOT is characterized by the presence of epithelial cells, homogenous eosinophilic amyloid-like material, and calcification. The epithelial cells are arranged in nests and sheets and are polygonal, with clear to eosinophilic cytoplasm and vesicular nuclei having prominent nucleoli. A cribriform and pseudoglandular pattern of epithelial cells is also described. While moderate pleomorphism can be seen, necrosis and atypical mitosis is uncommon. Rounded, pale, eosinophilic material resembling amyloid is seen interspersed amidst tumor cells and is a characteristic finding of CEOT. Although the exact origin of this amyloid is not known it is believed to be derived from filamentous degradation of keratin filaments secreted by tumor epithelial cells.[2] The presence of calcification is another defining feature of Pindborg tumor. The extent and shape of calcification can vary from minimal small round concretions to Liesegang rings and large aggregates.
According to Krolls and Pindborg, the presence or absence of calcification in CEOT has prognostic implications. A lack of calcification indicates less tumor differentiation and hence favors more chance of recurrence.[10] Pindborg has also reported recurrence after removal in a CEOT that had minimal calcifications (Pindborg, J.J: Personal communication, 1974).
Total absence of calcification in CEOT has been reported in English language literature in only three cases previously.[3–5] The first case was of a 68-year-old man who presented with a slow-growing swelling in the mandible.[3] In the second case, a 58-year-old man presented with an intraosseus tumor in left maxillary canine and premolar region. Histopathology revealed small islands of epithelial cells, spherical eosinophilic deposits, and fibromyxoid stroma, along with S-100–positive Langerhans cells.[4] The third case was a 61-year-old man having a tumor in the anterior maxilla, which on histopathology showed total absence of calcification.[5] While the first case did not show any evidence of recurrence 1 year after surgical excision, follow-up in the other two cases is not documented. In the present case, the tumor was located in the mandible and showed diffuse amorphous eosinophilic deposits, along with interspersed epithelial cells; Langerhans cells were however not seen. No areas of clear-cell morphology were identified (the clear-cell variant of CEOT is known to have aggressive behavior).[9] Our patient is on regular follow-up and the tumor has not recurred 1 year after surgical excision.
The absence of calcification not only posed difficulties in diagnosing this rare tumor but also warranted an aggressive treatment approach. This case highlights the unusual microscopic feature of this rare tumor. Prompt recognition of this variant can guide surgical management and alert the clinician to the need for extended follow-up.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Pindborg JJ. Calcifying epithelial odontogenic tumour. Acta Pathol Microbiol Scand. 1955;7:111. doi: 10.1111/apm.1966.68.2.169. [DOI] [PubMed] [Google Scholar]
- 2.Aviel-Ronen S, Liokumovich P, Rahima D, Polak-Charcon S, Goldberg I, Horowitz A. The amyloid deposit in calcifying epithelial odontogenic tumor is immunoreactive for cytokeratins. Arch Pathol Lab Med. 2000;124:872–6. doi: 10.5858/2000-124-0872-TADICE. [DOI] [PubMed] [Google Scholar]
- 3.Aufdermaur M. Pindborg tumour. J Cancer Res Clin Oncol. 1981;101:227–30. doi: 10.1007/BF00413317. [DOI] [PubMed] [Google Scholar]
- 4.Takata T, Ogawa I, Miyauchi M, Ijuhin N, Nikai H, Fujita M. Non-calcifying Pindborg tumor with Langerhans cells. J Oral Pathol Med. 1993;22:378–83. doi: 10.1111/j.1600-0714.1993.tb01093.x. [DOI] [PubMed] [Google Scholar]
- 5.Hafian H, Mauprivez C, Furon V, Pluot M, Lefevre B. Pindborg tumour: A poorly differentiated form without calcification. Rev Stomatol Chir Maxillofac. 2004;105:227–30. doi: 10.1016/s0035-1768(04)72313-x. [DOI] [PubMed] [Google Scholar]
- 6.Patiño B, Fernández-Alba J, Garcia-Rozado A, Martin R, López-Cedrún JL, Sanromán B. Calcifying epithelial odontogenic (pindborg) tumour: A series of 4 distinctive cases and a review of the literature. J Oral Maxillofac Surg. 2005;63:1361–8. doi: 10.1016/j.joms.2005.05.302. [DOI] [PubMed] [Google Scholar]
- 7.Maiorano E, Renne G, Tradati N, Viale G. Cytogical features of calcifying epithelial odontogenic tumor (Pindborg tumor) with abundant cementum-like material. Virchows Arch. 2003;442:107–10. doi: 10.1007/s00428-002-0722-x. [DOI] [PubMed] [Google Scholar]
- 8.El-Labban NG. Cementum-like material in a case of Pindborg tumor. J Oral Pathol Med. 1990;19:166–9. doi: 10.1111/j.1600-0714.1990.tb00818.x. [DOI] [PubMed] [Google Scholar]
- 9.Hicks MJ, Flaitz CM, Wong ME, McDaniel RK, Cagle PT. Clear cell variant of calcifying epithelial odontogenic tumor: Case report and review of the literature. Head Neck. 1994;16:272–7. doi: 10.1002/hed.2880160311. [DOI] [PubMed] [Google Scholar]
- 10.Krolls SO, Pindborg JJ. Calcifying epithelial odontogenic tumor. A survey of 23 cases and discussion of histomorphologic variations. Arch Pathol. 1974;98:206–10. [PubMed] [Google Scholar]