

Abstract
Aim
The first step in the management of Temporomandibular Disorders (TMD) is usually noninvasive, especially if the disorder is in the early stages. Clinically, pain and clicking are early signs and symptoms of TMD. The management of TMD usually includes “splint therapy” and analgesics. In this study, we report our long-term outcomes in the treatment of patients suffering from early TMD.
Materials and Methods:
We assessed the records of 138 patients who were referred for management of TMD. Selection was based on pain and/or clicking of the Temporomandibular Joint (TMJ), no pathologic lesions of the TMJ, no anterior disc displacement without reduction (closed lock), no Degenerative Joint Disease, no history of migraine, trauma, osteoarthritis, metabolic disease, or malocclusion (deep bite, cross bite, jaw deformity, etc). The patients were treated with an acrylic maxillary Interocclusal Splint (IOS) cuspid-rise type and were told to refrain from biting, yawning and chewing hard food. The outcome of the treatment, potential etiologic factors (Bruxism), signs and symptoms and patient demographics (such as age, sex, treatment duration, etc.) were assessed. The data were analyzed using the Chi-square test to correlate significance.
Results:
One hundred thirty-eight patients (26 males and 112 females) with early signs and symptoms of TMD (pain and/or click of the TMJ) were treated from 2001 to 2010; 81% were females and 19% were males. All the 138 patients used the IOS at night only. The patients were followed-up for 1–9 years. Data analysis showed that 64% of the patients were completely relieved of signs and symptoms; 22% were moderately relieved (decreased severity of signs and symptoms) and 14% had no noticeable post-treatment changes in clicking or pain (P = 0.001). Patients with bruxism and those presenting with both pain and clicking showed a better response to IOS treatment (P = 0.046 and P = 0.001, respectively). The results also showed that age, sex, severity of symptoms and duration of the treatment did not influence treatment results in this group of patients with early TMD.
Conclusion:
In this population, TMD was significantly higher in females. Treatment of early TMD with IOS was effective and moderately effective in long-term in over 80% of the patients during the follow-up period of 1–9 years. Bruxism had a significant etiologic role in TMD; occlusal attrition of the dentition, pain of all the teeth, early morning pain of the masticatory muscles and the TMJ are signs and symptoms to suspect nocturnal bruxism. Use of an IOS is recommended to prevent potential damage to the dentition, periodontium and the TMJ in early TMD.
Keywords: Bruxism, clicking, interocclusal splint, pain, TMD
INTRODUCTION
Masticatory muscle pain, limitation or interference in mandibular movement and joint sounds, such as clicking or popping, clinically signify Temporomandibular Disorders (TMD).[1] The prevalence of TMD is high. The prevalence of joint pain and clicking in the study population is between 6% and 12%.[2,3] Females comprise 80%–95% of the treated cases.[4] According to the existing reports, success of clinical management is 70%-90% and failure of treatment is 15%.[5] Current management for TMD is divided into 2 groups: conservative and invasive.[5] Common conservative management is “splint therapy” using an IOS also known as the Fox appliance, centric relation appliance, stabilization splint, night guard and Michigan splint.[6] In 2003, Ekberg et al. reported more reduction in joint pain in TMD patients treated with “IOS” than in the control group (P = 0.028).[7] In 2005, Al-Ani also reported better results with “IOS” management than any other conservative managements.[6] The aim of this study was to evaluate the long-term results of IOS in patients suffering from early signs and symptoms of TMD (pain and clicking).
MATERIALS AND METHODS
This 9-year study (2001–2010) assessed records of 138 patients who were referred for management of TMD. Selection was based on pain and/or clicking of the Temporomandibular Joint (TMJ), no pathologic lesions of the TMJ, no anterior disc displacement without reduction (closed lock), no Degenerative Joint Disease, no history of migraine, trauma, osteoarthritis, metabolic disease, or malocclusion (crossbite, deepbite, jaw deformity, etc.). Severity of initial symptoms was divided into 3 groups: mild, moderate and severe. All had tried analgesics and relaxants for several months before starting splint therapy. The patients were treated with an acrylic maxillary Interocclusal Splint (IOS) cuspid-rise type and were told to refrain from biting, yawning and chewing hard food. The outcome of treatment, potential etiologic factors (trauma, skeletal deformities and bruxism), signs and symptoms and patient demographics (such as age, sex, treatment duration, etc.) were assessed.
Patients with obvious contributing factors, that is, occlusal status (partially dentulous, edentulous, deep bite, cross bite), were excluded. Our study was a retrospective chart review study exempt from our institution review board and ethics committee. The data were analyzed using the Chi-square test to correlate significance.
RESULTS
One hundred thirty-eight patients (26 males and 112 females) with early signs and symptoms of TMD (pain and/or click of the TMJ) and a mean age of 30.2 years were treated from 2001 to 2010; 81% were females and 19% were males. In these patients, 10/138 (7.2%) of those who suffered from click only, 46/138 (33.3%) patients who suffered from pain only and 82/138 (59.4%) patients suffered from pain + click at the start of the treatment were relieved of symptoms; 87/138 (63.0 %) patients had bruxism. All the 138 patients used IOS at night only. The patients were followed-up for 1–9 yrs. Data analysis showed that 64% of patients were completely relieved (loss of signs and symptoms), 22% were moderately relieved (decreased severity of signs and symptoms) and 14%had no noticeable post-treatment changes (P = 0.001). The results showed that the patients with bruxism and those with pain and clicking had a better response to IOS treatment (P = 0.046 and P = 0.001, respectively). The results also showed that age, sex, severity of symptoms and duration of the treatment did not influence the treatment results [Figures 1 and 2].
Figure 1.
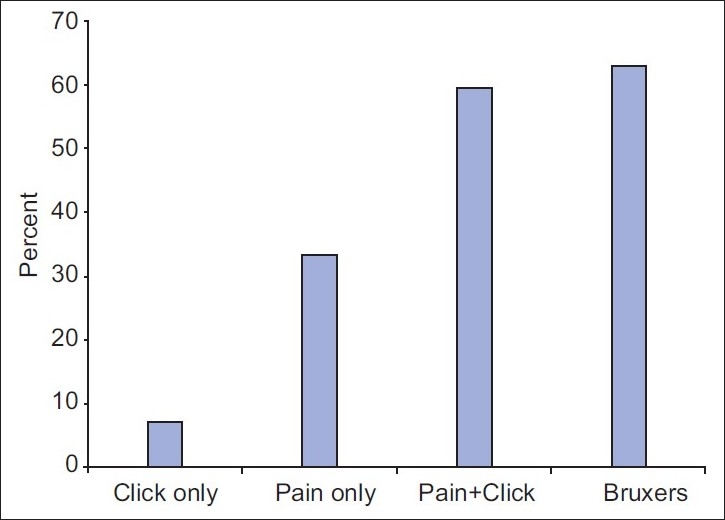
Response to treatment relative to signs and symptoms of patients with temporomandibular disorders
Figure 2.
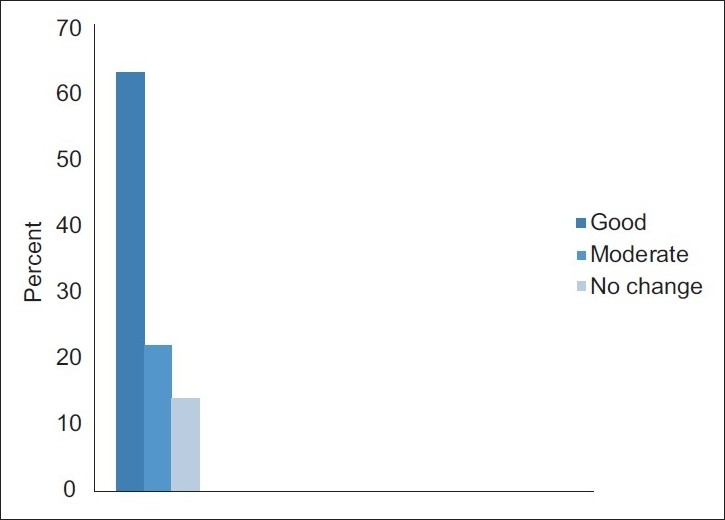
Overall response of the patients to interocclusal splint treatment
DISCUSSION
One of the significant findings of this study was that 63% of the patients had bruxism. Nocturnal bruxism is an oral habit consisting of involuntary rhythmic or spasmodic nonfunctional grinding or clenching of teeth, in other than chewing movements of the mandible, which may lead to occlusal trauma.[8–12] The IOS was effective in this regard as results showed that patients with bruxism showed a significantly better response to IOS treatment. Bruxism is considered one of the main causes of TMD.[12,13] Our study also showed that early onset TMD is reversible with IOS being effective in over 80% of the patients during the follow-up period (P = 0.001). According to our study, TMD patients with pain + clicking were treated significantly better than those who had just one of these findings (P = 0.001). As would be expected, however, assessment of factors, such as age, sex and severity of initial symptoms, did not show significant correlation with outcomes.
IOS effect on pain
The effect of the oral splint on pain is important. In 2003, Ekberg et al. reported a significant reduction of pain in IOS patients (P = 0.028).[7] Conti et al. showed faster improvement with IOS use with an 83.4% healing rate.[8] Johansson also reported pain reduction with IOS (P < 0.001).[14] Badel et al. reported pain reduction in 69.2% of patients with anterior disc displacement with reduction.[9] Bergstrom et al. reported long-term follow-up (18–20 years) of reduction of pain in 50% of TMD patients.[15] In 2006, Conti et al. reported faster improvement rate in IOS patients than in controls with TMD.[8] In 2009, Badel et al. reported 69.2% pain reduction in a study with inclusion criteria similar to our study.[9]
IOS effect on click
Clicking results from anterior disc displacement. Conti et al. reported reduction of joint click after the use of IOS.[8] Wassel et al. showed that after treatment of early onset TMD with IOS for 6 weeks, the mean reduction of symptoms was significant; however, clicking and improvement of clicking required a minimum of 5 months of IOS therapy.[16] Thus, elimination of clicking needs more time to heal than other symptoms of TMD. In our study, in 50%of the patients clicking was eliminated completely.
During recall appointments, some patients had remarked that IOS increased their cognizance of parafunction; occlusal coverage and tooth contacts on splints are important factors that change tongue position and increase patient awareness of parafunctional activity. Patient reassurance is an important factor in the treatment of TMD. Generally TMD is stated to be a self-limiting disorder and that improvement is achieved without invasive treatment, especially if it is early in the course provided that the cause of TMD is eliminated.[17] The patients in our study were treated with IOS only after drug therapy and the rest were ineffective and there was no improvement of symptoms after 1–2 months. Our study was effective in treating pain and/or click of TMJ in patients devoid of destructive joint lesions confirmed by radiography and MRI.
CONCLUSION
In this population, TMD was significantly higher in females. Treatment of early TMD with IOS was effective and moderately effective in long-term in over 80% of the patients during the follow-up period of 1–9 years. Bruxism had a significant etiologic role in TMD; occlusal attrition of the dentition, pain of all the teeth, early morning pain of the masticatory muscles and the TMJ are signs and symptoms to suspect nocturnal bruxism. Use of an IOS is recommended to prevent damage to the dentition, periodontium and the TMJ in early TMD.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Le Resche L, Von Kroff MR. Research diagnostic criteria. J Craniomandib Disord. 1992;6:301–35. [PubMed] [Google Scholar]
- 2.Larach Dc, Lipton JA. Responses to persistent jaw, face and burning mouth pain in the United States. J Dent Res. 1993;72:313. [Google Scholar]
- 3.Von Korff M, Wagner EH, Dworkin SF. Chronic pain and use of ambulatory health care. Psychosom Med. 1991;53:61–79. doi: 10.1097/00006842-199101000-00006. [DOI] [PubMed] [Google Scholar]
- 4.De Kanter RJ, Truin GJ, Burgersdik RC. Prevalence in the Dutch adult population and a meta-analysis of signs and symptoms of temporomandibular disorder. J Dent Res. 1993;72:1509–18. doi: 10.1177/00220345930720110901. [DOI] [PubMed] [Google Scholar]
- 5.Linde C, Issacsson G, Jonsson BG. Outcome of 6 week treatment with transcutaneous electrical nerve stimulation compared with splint on symptomatic temporomandibular joint disc displacement without reduction. Acta Odontol Scanda. 1995;53:92–8. doi: 10.3109/00016359509005953. [DOI] [PubMed] [Google Scholar]
- 6.Al-Ani Z, Gray RJ, Davies SJ, Sloan P. Stabilization splint therapy for the treatment of temporomandibular myofascial pain: A systematic review. J Dent Educ. 2005;69:1242–50. [PubMed] [Google Scholar]
- 7.Ekberg EC, Vallon D, Nilner M. The efficacy of appliance therapy in patients with temporomandibular disorders of mainly myogenous origin. A randomized, controlled, short term study. J Orofac pain. 2003;17:133–9. [PubMed] [Google Scholar]
- 8.Conti PC, dos Santos CN, Kogawa EM, de Castro Ferreira Conti AC, de Araujo Cdos R. The treatment of painful temporomandibular joint clicking with oral splints.A randomized clinical trial. J Am Dent Assoc. 2006;8:1108–14. doi: 10.14219/jada.archive.2006.0349. [DOI] [PubMed] [Google Scholar]
- 9.Badel T, Marotti M, Kern J, Laskarin MA. Quantitative analysis of splint therapy of displaced temporomandibular joint disc. Ann Anat. 2009;191:280–7. doi: 10.1016/j.aanat.2008.12.004. [DOI] [PubMed] [Google Scholar]
- 10.Proff P. A Michigan type occlusal splint with spring loaded mandibular protrusion functionality for treatment of anterior disc dislocation with reduction. Ann Anat. 2007;189:362–9. doi: 10.1016/j.aanat.2007.02.026. [DOI] [PubMed] [Google Scholar]
- 11.Cane L, Schieroni MP, Ribero G, Ferrero M, Carossa S. Effectiveness of the Michigan splint in reducing functional cervical disturbances: A preliminary study. J Craniomand pract. 1997;15:132–5. doi: 10.1080/08869634.1997.11746003. [DOI] [PubMed] [Google Scholar]
- 12.Porter R, Poyser N, Briggs P, Kelleher M. Demolition Experts: Management of the parafunctional patient: 1. Diagnosis and Prevention. Dent Update. 2007;34:198–207. doi: 10.12968/denu.2007.34.4.198. [DOI] [PubMed] [Google Scholar]
- 13.Linde C, Issacsson G, Jonsson BG. Outcome of 6-week treatment with transcutaneous electric nerve stimulation compared with splint on symptomatic temporomandibular joint disk displacement without reduction. Acta Odontol Scand. 1995;53:92–8. doi: 10.3109/00016359509005953. [DOI] [PubMed] [Google Scholar]
- 14.Johansson A, Wenneberg B, Wagersten C, Haraldson T. Acupuncture in treatment of facial muscular pain. Acta Odontol Scand. 1991;49:153–8. doi: 10.3109/00016359109005900. [DOI] [PubMed] [Google Scholar]
- 15.Bergstrom I, List T, Magnusson T. A follow up study of subjective symptoms of temporomandibular disorders in patients who received acupuncture and /or interocclusal appliance therapy 18-20 years earlier. Acta Odontol Scand. 2008;66:88–92. doi: 10.1080/00016350801978660. [DOI] [PubMed] [Google Scholar]
- 16.Wassel RW, Adams N, Kelly P. The treatment of temporomandibular disorders with stabilizing splints in general dental practice. One-year follow-up, J Am Dent Assoc. 2006;137:108–98. doi: 10.14219/jada.archive.2006.0347. [DOI] [PubMed] [Google Scholar]
- 17.Fein JS, Lund JP. An assessment of the efficacy of physical therapy and physical modalities for the control of chronic musculoskeletal pain. Pain. 1997;71:5–23. doi: 10.1016/s0304-3959(96)03287-3. [DOI] [PubMed] [Google Scholar]