

Abstract
Mandibular nerve block is often performed for diagnostic, therapeutic and anesthetic purposes for surgery involving mandibular region. Advantages of a nerve block include excellent pain relief and avoidance of the side effects associated with the use of opiods or Non-steroidal anti-inflammatory drug (NSAIDs). A patient with maxillo facial trauma was scheduled for open reduction and internal fixation of right parasymphyseal mandibular fracture. The mandibular nerve was approached using the lateral extraoral approach with an 18-gauge i.v. cannula under general anesthesia. He received 4 ml boluses of 0.25% plain bupivacaine for intraoperative analgesia and 12 hourly for 48 h post operatively. VAS scores remained less than 4 through out observation period. The only side effect was numbness of ipsilateral lower jaw line, which subsided after local anesthetic administration was discontinued. Patient was discharged after four days.
Keywords: Epidural catheter, mandibular nerve block, maxillo facial injuries, pain
INTRODUCTION
Maxillofacial injuries have the potential to cause airway compromise and are associated with pain and swelling causing difficulty in mouth opening, chewing and deglutition. Mandibular nerve block is still an underutilized modality of pain management. It helps in intraoperative pain relief and also helps in early post operative rehabilitation of Maxilla facial trauma patients. Literature search does not reveal many such case reports. Mandibular nerve block is often performed for diagnostic, therapeutic and anesthetic purposes for surgery involving mandibular region. We report a case where intraoperative and post-operative pain in a case of unilateral fracture mandible was effectively managed through intermittent mandibular nerve block via a catheter.
CASE REPORT
A 30-year-old male with right sided parasymphyseal fracture mandible was scheduled for open reduction and internal fixation. The patient had difficulty in opening the mouth due to pain (3 cm). General physical examination and laboratory investigations were within normal limits. Informed written consent for the nerve block was obtained and visual analogue scale (VAS) of 0-10, was explained to patient.
In the operation theater, standard monitoring was established. Anesthesia was induced with thiopentone and tracheal intubation was facilitated with succinylcholine. Neuromuscular blockade was achieved with vecuronium and anesthesia was maintained with O2 and N2O using controlled ventilation. The right side of the face was prepared for mandibular nerve block with lateral extraoral approach [Figure 1].
Figure 1.
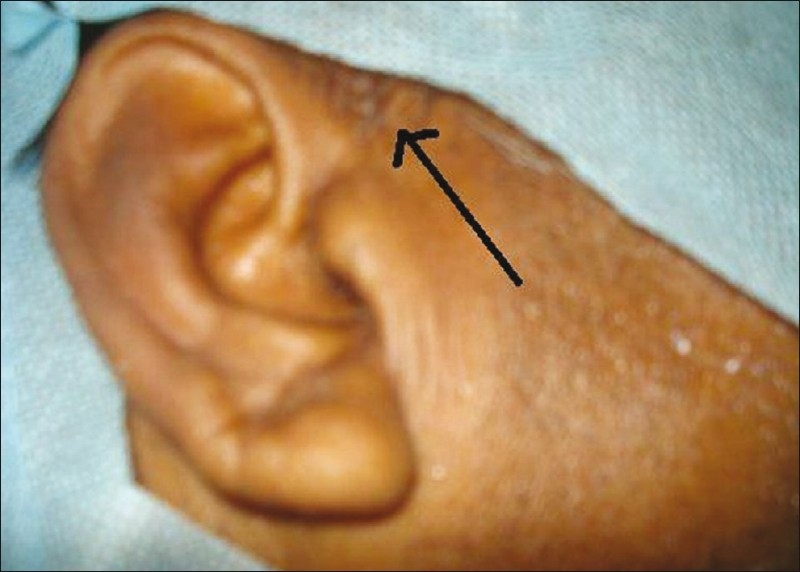
Arrow showing skin site of epidural needle insertion for mandibular nerve block
An 18-gauge i.v. cannula was inserted at midpoint of lower border of the zygomatic arch and was advanced perpendicular to face until it contacted the lateral pterygoid plate. The length of the cannula outside the skin was marked and cannula was redirected slightly posterior to reach behind the posterior border and was advanced further by 0.5 cm. The needle from the cannula was withdrawn and 18G epidural catheter was threaded. Catheter was tunnelled subcutaneously and the filter was attached to its other end [Figure 2]. For surgical analgesia, a bolus dose of 4 ml of 0.25% bupivicaine was given through the catheter. Fentanyl 1mg/ kg i.v. was given only when there was more than 20% increase in heart rate or blood pressure above base line. The surgery lasted for 2 h. At the end of surgery, neuromuscular blockade was reversed and the trachea extubated. Following extubation, the patient was conscious and pain free and then shifted to ward. Post Operatively, he received 4 ml of 0.25% bupivacaine through the epidural catheter every 12 h for two days. VAS score was measured immediately after surgery and thereafter at 1, 2, 4, 6, 12, 24, and 48 h respectively. Patient was observed for numbness at the surgical site, need for rescue analgesia, complications (nausea, vomiting). The patient's vitals remained stable throughout the period of observation. His VAS score ranged between 2 and 4 with pain free jaw opening. There were no complications and he did not require any rescue analgesia. The catheter was removed after two days. There was no evidence of infection at the exit site. Numbness in area of lower jaw line was present throughout the period but subsided after discontinuation of local anesthetic through epidural catheter. He was discharged on fourth post operative day with advice for follow up in O.P.D.
Figure 2.

Epidural catheter used for intermittent mandibular nerve block
DISCUSSION
Mandibular nerve block can be used to manage intra as well as post operative pain in cases of fracture mandible. It can be performed via lateral extraoral[1] or intraoral approach. We performed lateral extra oral approach because of restricted mouth opening and the need to retain the catheter for post operative analgesia. 18G cannula instead of epidural needle was used to minimize the bleeding from pterygoid plexus of veins. The cannula was advanced further after contacting lateral pterygiod plate so that the catheter comes in vicinity of mandibular nerve and there is no displacement during jaw movements.[2] The catheter was further tunnelled subcutaneously to prevent dislodgement and filter was used to prevent infection. Proper precautions were taken to prevent skin infection, kinking and obstruction of catheter.[3] There was excellent post operative analgesia achieved with this technique as shown in decreased pain scores, both static as well as dynamic. The hospital stay was also reduced.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Wedel DJ, Brown DL. Nerve Blocks. In: Miller RD, editor. anaesthesia. 3rd ed. New York: Churchill-Livingstone; 1990. pp. 1407–37. [Google Scholar]
- 2.Singh B, Srivastava SK, Dang R, Gombar KK, Gombar S. Anatomic considerations in relation to the mandibular nerve block. Reg Anesth. 1993;18:181–3. [PubMed] [Google Scholar]
- 3.Singh B, Bhardwaj V. Continuous mandibular nerve block for pain relief: A report of two cases. Can J Anaesth. 2002;49:951–3. doi: 10.1007/BF03016881. [DOI] [PubMed] [Google Scholar]