

Abstract
Congenital lingual cystic masses are challenging entities that can be detected prenatally or are discovered in various forms after birth. Foregut duplication cyst of tongue is an extremely rare condition. Here we present the eleventh case in literature on foregut duplication cyst in tongue lined with gastric mucosa. Complete excision was curative with no recurrence on followup.
Keywords: Foregut, duplication cyst, lingual swelling
INTRODUCTION
A lingual cystic mass in a newborn is an interesting challenge for the pediatric surgeons. Although most cases are brought to attention following birth, some are detected prenatally. Some of these masses present with respiratory distress requiring emergency intervention.[1,2] Among the different lesions that can arise in the tongue, the foregut duplication cyst is of special interest because of its rarity, variable characteristics, and its puzzling embryogenesis. Until now, only ten cases of intralingual foregut duplication cysts lined with gastric mucosa have been reported in the literature [Table 1].[3–9]
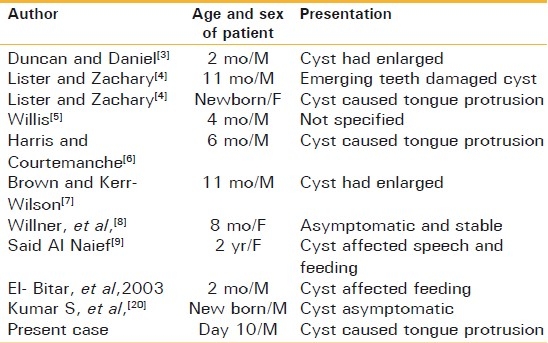
Table 1.
Reported cases of gastric variety of intralingual foregut duplication cyst
REVIEW REPORT
This neonate presented with mass in tongue on tenth day of life [Figure 1], which was diagnosed as tongue lymphangioma in anomaly scan at the 8th month of gestation. Fullterm child with 3kg birth weight was not able to take breast feed and was on spoon feeding. On examination, his right side of the tongue and floor of mouth was diffusely enlarged, and a bulge was noted at the right submandibular region. On palpation, cystic, nonpulsatile mass was felt in the body of the tongue. Ultrasound revealed a 4 × 4 × 2.2 cm mixed cystic mass, probably lymphangioma. Computed tomography (CT) scan detected a 3.6 × 3.4 × 4.2 cm solid mass with cystic areas confined to the tongue with involvement of floor of mouth. There was diagnostic dilemma between lymphangioma and cystic variety of teratoma. Malignancy workup was negative. Marspulisation and wedge biopsy was taken as complete excision was not possible. Histopathology was suggestive of mucous retention cyst and ruled out malignant lesion.
Figure 1.

Tongue mass
Postoperatively the mass gradually increased in size and by the age of 2.5 months he began exhibiting difficulty in feeding. Magnetic resonance imaging (MRI) revealed multicystic purely tongue-based lesion with involvement of floor of mouth and with no involvement of other surrounding structures [Figure 2]. Patient underwent surgery under general anesthesia with nasotracheal intubation and throat pack [Figure 3]. The cyst was excised completely. The cyst wall was thick and adherent to the lingual muscles. The lesion extended to the base of the tongue [Figure 4]. The excised mass measured 3 × 2.4 × 1.2 cm. Postoperative course was uneventful [Figure 5].
Figure 2.
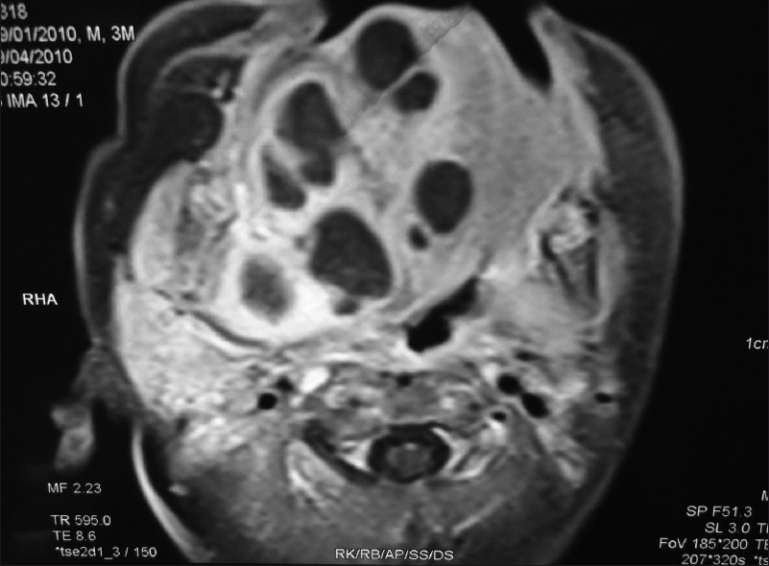
Magnetic resonance imaging
Figure 3.

Pre op
Figure 4.
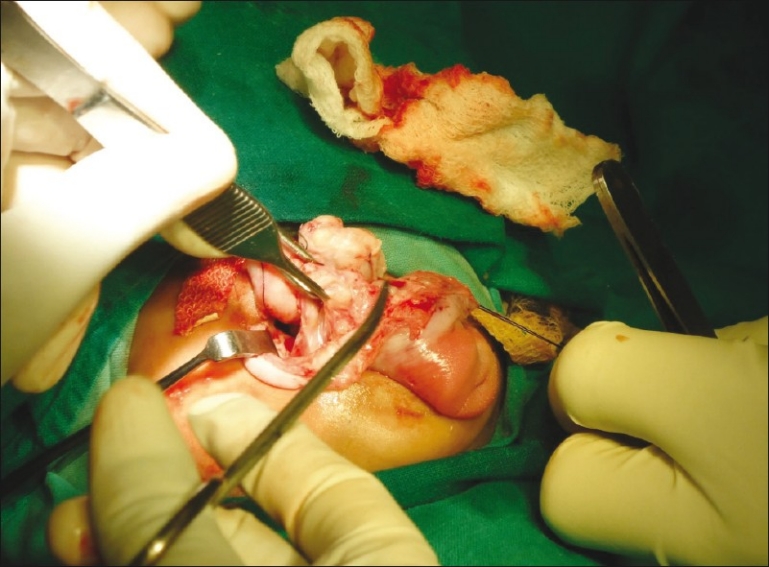
Intra op
Figure 5.

Postop appearance
Histopathology revealed oral cystic lesion lined by gastric type of epithelium. It featured an outer smooth-muscle layer (muscularis propria, with circular and longitudinal layers), submucosa, and areas of mucosal lining that contained pits and glands and were consistent with gastric mucosa. Other areas of the mucosa were of the simple columnar type [Figure 6].
Figure 6.
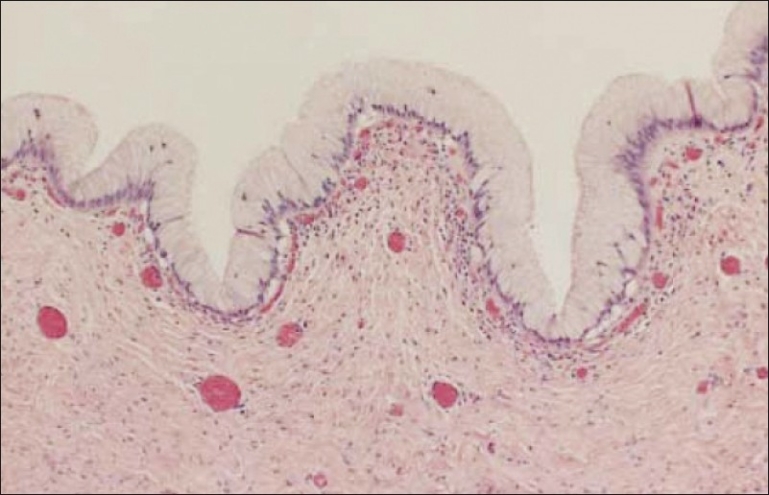
Histopathological picture
DISCUSSION
A cystic mass in the anterior two-thirds of the tongue in a newborn can represent ranula, lymphangima, haemangioma, and dermoid cyst.[4,10,11] Since first reported by Duncan and Daniel[9] in 1942, cysts lined with gastric and/or intestinal mucosa have rarely been seen in the tongue or the floor of the mouth. These cysts have usually been reported along the alimentary tract, from the esophagus to the colon,[10,12] and in the gallbladder, pancreas, lungs, larynx, and urinary bladder.[13]
Congenital gastric and intestinal cysts of the oral cavity are more common in boys than in girls.[2,8,9,14] These masses involve the anterior aspect of the tongue in 60% of cases.[9,10] Some are asymptomatic, and some cause various degrees of feeding and breathing difficulties or manifest in unexpected ways, such as recurrent bleeding[13] or a brownish discharge from a lingual sinus.[10] Most of these cysts are solitary, but in some cases more than one cyst has been present.[14,15]
These lesions have been given several names, including cystic choristoma, heterotopic gastrointestinal cyst, enterocystoma, and duplication cyst.[9] Our case fulfilled Rickham's diagnostic criteria for duplication cysts including the presence of a smooth-muscle coat, an attachment of the cyst to a part of the alimentary tract, and the presence of a mucosal lining from the alimentary tract.[4,7,8,11,16]
Extensive research revealed only ten cases of which only two were multilocular.[3–9,17] Lingual foregut duplication cysts are believed to arise from endodermal cells that become trapped during the fusion of the lateral lingual swelling (distal tongue bud) and the tuberculum impar (median tongue bud) in the 3- to 4-mm embryo.[2,10,14] These cells are believed to derive from the stomodeum.[18] These pluripotential cells can differentiate into various types of epithelium, including gastric, intestinal, colonic, and even respiratory [Figure 7].
Figure 7.
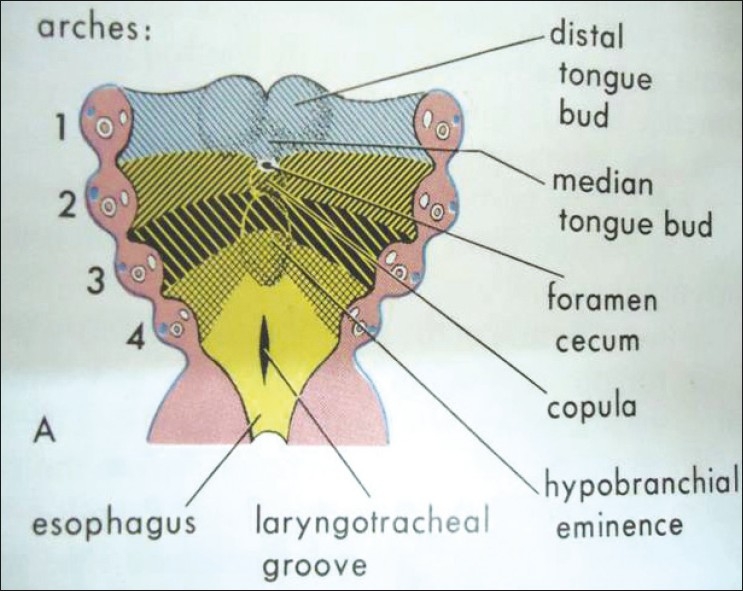
Developmental picture
In addition to a clinical examination,[10,13] the initial evaluation of a newborn with a lingual mass can include ultrasonography, Computed tomography(CT), and/or magnetic resonance imaging(MRI).[8,9] Clinical examination alone cannot differentiate among the wide variety of possible lesions. Anomaly scan is also a useful tool for antenatal diagnosis of the lesion.
Excising an intralingual cyst whose wall adheres to the surrounding muscles is a tedious exercise, especially in an infant with a large cyst. Total, if not possible then subtotal excision is curative.[15,17,19,20]
CONCLUSION
Intralingual foregut duplication cyst should be considered in the differential diagnosis of a lingual cystic mass in an infant. Early surgical excision in a symptomatic patient is desirable in order to avoid failure-to-thrive, respiratory distress, or more extensive surgery later.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Chen MK, Gross E, Lobe TE. Perinatal management of enteric duplication cysts of the tongue. Am J Perinatol. 1997;14:161–3. doi: 10.1055/s-2007-994119. [DOI] [PubMed] [Google Scholar]
- 2.Grime PD. Giant enterocystoma within an infant's tongue. J Laryngol Otol. 1990;104:814–8. doi: 10.1017/s0022215100113982. [DOI] [PubMed] [Google Scholar]
- 3.Duncan GW, Daniel RA., Jr Cystic tumor of the tongue: Report of an unusual case. Arch Surg. 1942;44:164–9. [Google Scholar]
- 4.Lister J, Zachary RB. Cystic duplications in the tongue. J Pediatr Surg. 1968;3:491–3. doi: 10.1016/0022-3468(68)90671-4. [DOI] [PubMed] [Google Scholar]
- 5.Willis RA. Some unusual developmental heterotopias. Br Med J. 1968;3:267–72. doi: 10.1136/bmj.3.5613.267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Harris CN, Courtemanche AD. Gastric mucosal cyst of the tongue: Case report. Plast Reconstr Surg. 1974;54:612–3. doi: 10.1097/00006534-197411000-00020. [DOI] [PubMed] [Google Scholar]
- 7.Brown S, Kerr-Wilson R. Intra-oral duplication cyst. J Pediatr Surg. 1978;13:95–6. doi: 10.1016/s0022-3468(78)80222-x. [DOI] [PubMed] [Google Scholar]
- 8.Willner A, Feghali J, Bassila M. An enteric duplication cyst occurring in the anterior two-thirds of the tongue. Int J Pediatr Otorhinolaryngol. 1991;21:169–77. doi: 10.1016/0165-5876(91)90149-6. [DOI] [PubMed] [Google Scholar]
- 9.Said-Al-Naief N, Fantasia JE, Sciubba JJ, Ruggiero S, Sachs S. Heterotopic oral gastrointestinal cyst: Report of 2 cases and review of the literature. Oral Surg Oral Med Oral-Pathol Oral Radial Endod. 1999;88:80–6. doi: 10.1016/s1079-2104(99)70197-6. [DOI] [PubMed] [Google Scholar]
- 10.Lipsett J, Sparnon AL, Byard RW. Embryogenesis of enterocystomas-enteric duplication cysts of the tongue. Oral Surg Oral Med Oral Pathol. 1993;75:626–30. doi: 10.1016/0030-4220(93)90238-y. [DOI] [PubMed] [Google Scholar]
- 11.Mirchandani R, Sciubba J, Gloster ES. Congenital oral cyst with heterotopic gastrointestinal and respiratory mucosa. Arch Pathol Lab Med. 1989;113:1301–2. [PubMed] [Google Scholar]
- 12.Ohbayashi Y, Miyake M, Nagahata S. Gastrointestinal cyst of the tongue: A possible duplication cyst of foregut origin. J Oral Maxillofac Surg. 1997;55:626–8. doi: 10.1016/s0278-2391(97)90497-3. discussion 629-30. [DOI] [PubMed] [Google Scholar]
- 13.Parikh DH, Ibrahim SK, Cook RC. Peptic ulceration in a lingual sinus. J Pediatr Surg. 1991;26:99–100. doi: 10.1016/0022-3468(91)90440-5. [DOI] [PubMed] [Google Scholar]
- 14.Mir R, Weitz J, Evans J, Coren C. Oral congenital cystic choristomas: A case report. Pediatr Pathol. 1992;12:835–8. doi: 10.3109/15513819209024240. [DOI] [PubMed] [Google Scholar]
- 15.Satish Kumar KV, Joshi M, Vishwanath N, Akhtar T, Oak SN. Neonatal lingual gastric duplication cyst: A rare case report. J Indian Assoc Pediatr Surg. 2006;11:97–8. [Google Scholar]
- 16.Rickham PP, Lister J, Irving IM. London: Butterworths; 1978. Neonatal surgery. [Google Scholar]
- 17.Eaton D, Billings K, Timmons C, Booth T, Biavati JM. Congenital foregut duplication cysts of the anterior tongue. Arch Otolaryngeal Head Neck. 2001;127:1484–7. doi: 10.1001/archotol.127.12.1484. [DOI] [PubMed] [Google Scholar]
- 18.Gorlin RJ, Kalnius V, Izant RJ. Occurrence of heterotopic gastric mucosa in the tongue. J Pediatr. 1964;64:604–6. doi: 10.1016/s0022-3476(64)80356-5. [DOI] [PubMed] [Google Scholar]
- 19.Thomas MR, Nofal F, Cave AP. Dermoid cyst in the mouth: Value of ultrasound. J Laryngol Otol. 1990;104:141–2. doi: 10.1017/s0022215100112083. [DOI] [PubMed] [Google Scholar]
- 20.Aydogan B, Kiroglu M, Soylu L, Aydin O, Satar M, Kiroðlu F, et al. Gastric cyst of the oral cavity. Int Pediatr Otorhinolaryngol. 1995;45:255–8. doi: 10.1016/s0165-5876(98)00107-4. [DOI] [PubMed] [Google Scholar]