

Abstract
The objective of this study was to evaluate the efficacy of aquadissection technique to reduce the blood loss in myomectomy and to assess the benefits and feasibility of the use of barbed suture for myometrial defect closure. Vasopressin is diluted with saline as 10 units of vasopressin for every 100 ml of saline. For a fibroid of about 8 cm size, 40 units of vasopressin is diluted in 400 ml of normal saline. The whole of 400 ml of this saline is injected in the myometrium. Incision is made on the uterus with just simple scissors (no energy source is required). As the uterus is cut, instead of bleeding, saline leakage takes place. This helps to keep the field clear and it is easier to get the correct plane between the fibroid and the myometrium. The separation of the fibroid is helped due to the dissection of the correct plane by the saline injection.
Keywords: Aquadissection, barbed suture, laparoscopy, myomectomy, saline, vasopressin
MODI'S AQUADISSECTION TECHNIQUE
The concept
Large quantity of saline is injected in the myometrium with a laparoscopic injection needle. This saline enters the myometrium and the blood in the myometrial tissue is replaced by saline. Thus, when myometrium is cut, only saline oozes out, almost no bleeding occurs and the field is further cleared by the saline which oozes out.
The vasopressin injected causes vasoconstriction of myometrial vessels, which helps to hold the saline within the myometrium for a period of about 45–60 min which is sufficient for the myometrial suturing to be completed.
The saline and vasopressin solution follows the path of least resistance and enters the plane between the myometrium and the myoma, which helps in enucleation of myoma; hence, the name aquadissection.
The technique
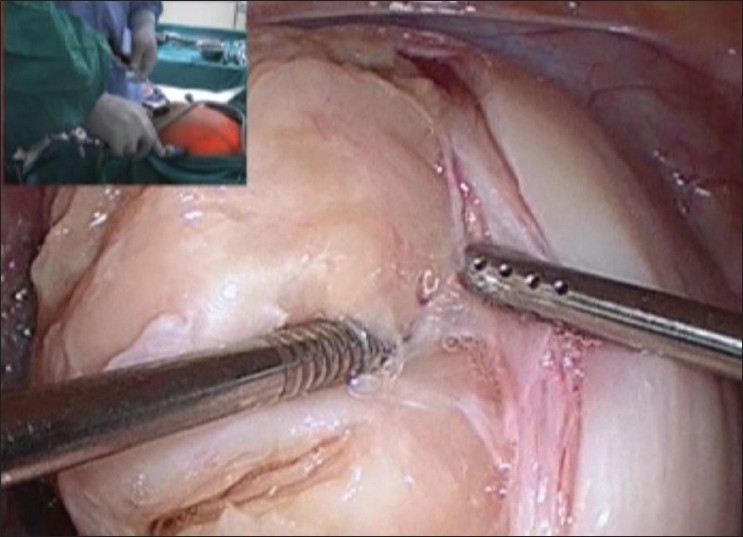
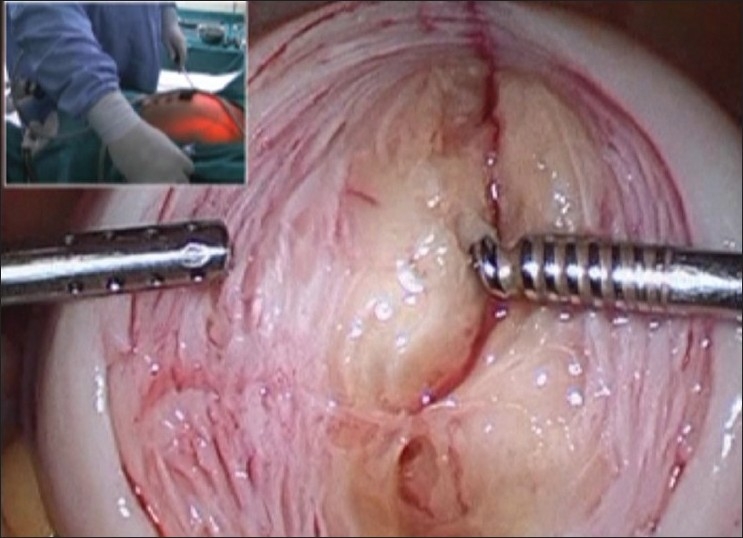
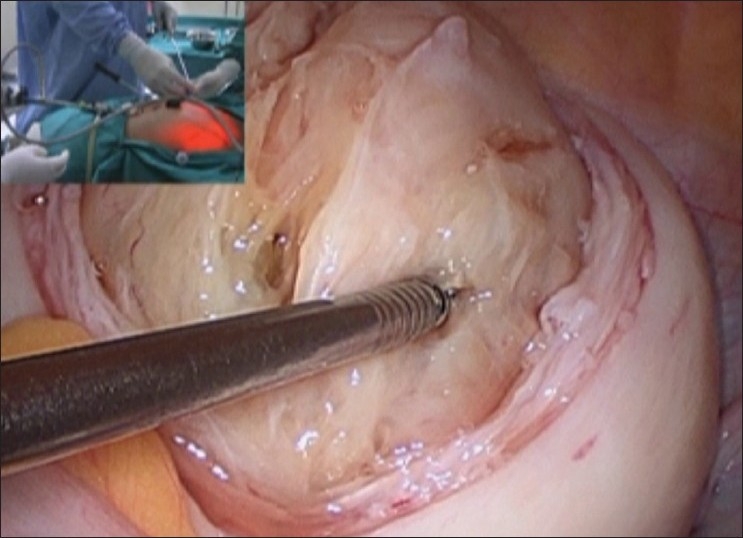
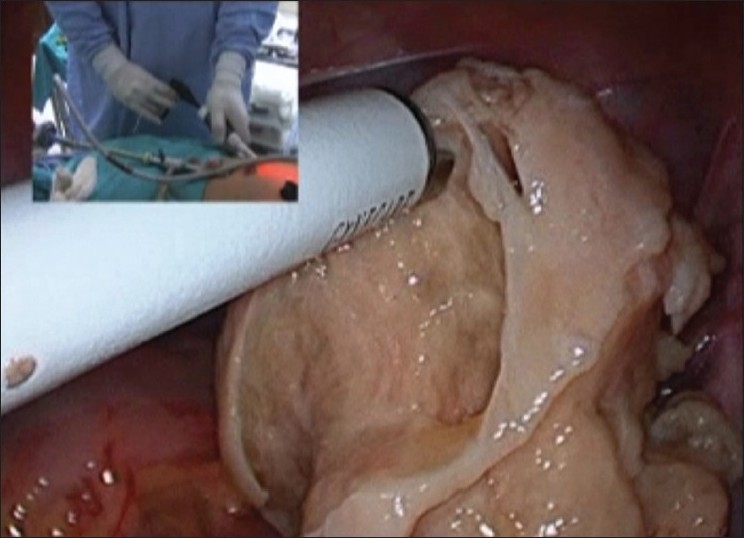
Vasopressin is diluted with saline as 10 units of vasopressin for every 100 ml of saline. For a fibroid of about 8 cm size, 40 units of vasopressin is diluted in 400 ml of normal saline. The whole of 400 ml of this saline is injected in the myometrium. Using a 10-ml syringe and a laparoscopic injection needle, from the 5 mm port, the injection needle is inserted between the uterus and the myoma. Needle is inserted to a depth of about 1 inch. Single insertion is sufficient in most cases. If needed, position of the needle may be changed once. Multiple sites will cause the injected saline to ooze out from the previous punctures. (Maintenance of cold chain of vasopressin inj. is essential.) As the effect of aquadissection with saline and vasopressin is achieved, the color of uterus changes from pink to white or marble like appearance [Figures 1 – 3]. Incision is made on the uterus with just simple scissors (no energy source is required).
Figure 1.
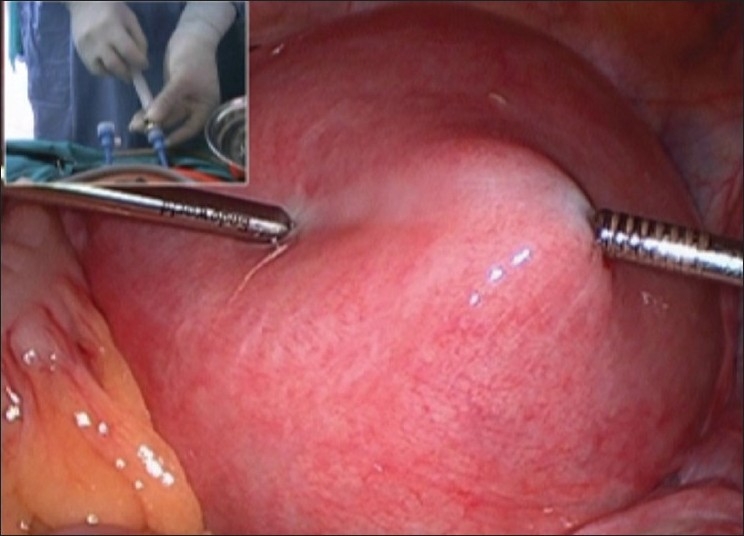
Before saline injection
Figure 3.

Injection needle
Figure 2.
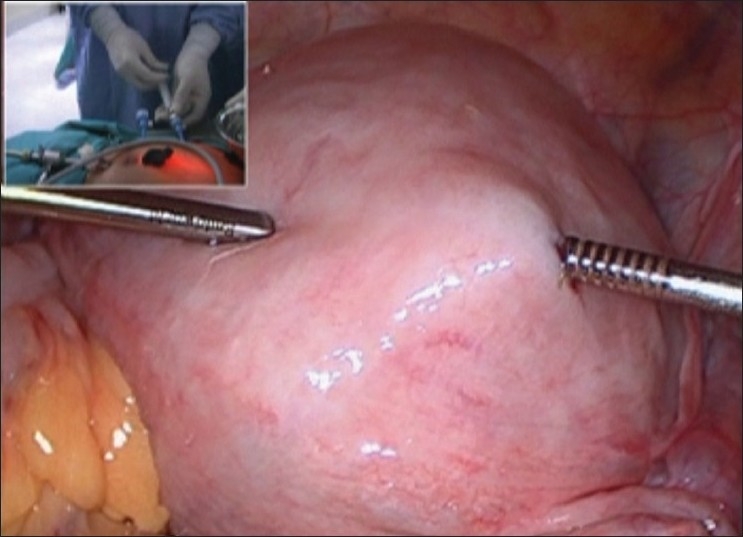
Whiteness after saline injection
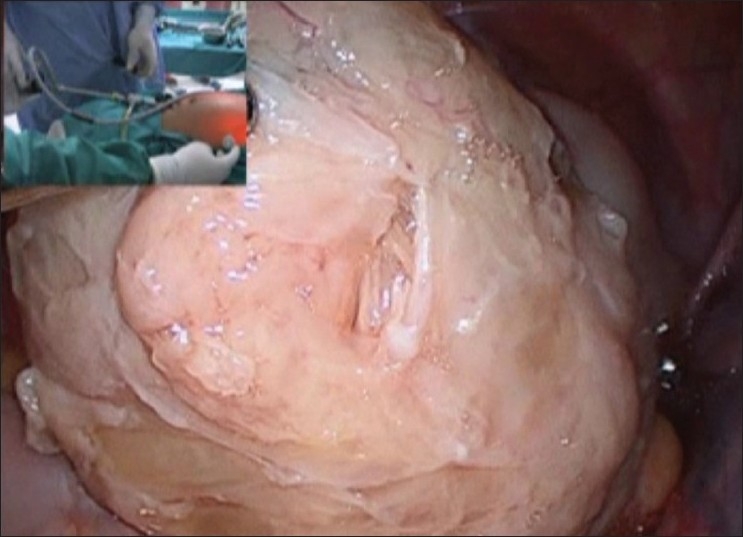
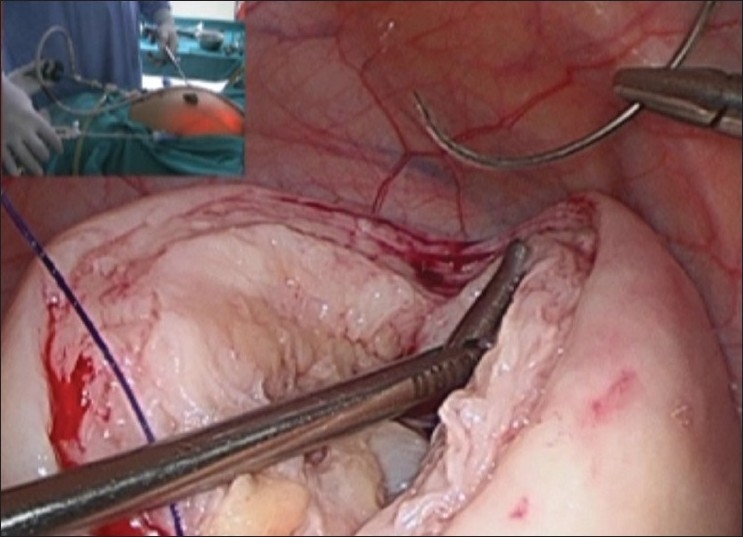
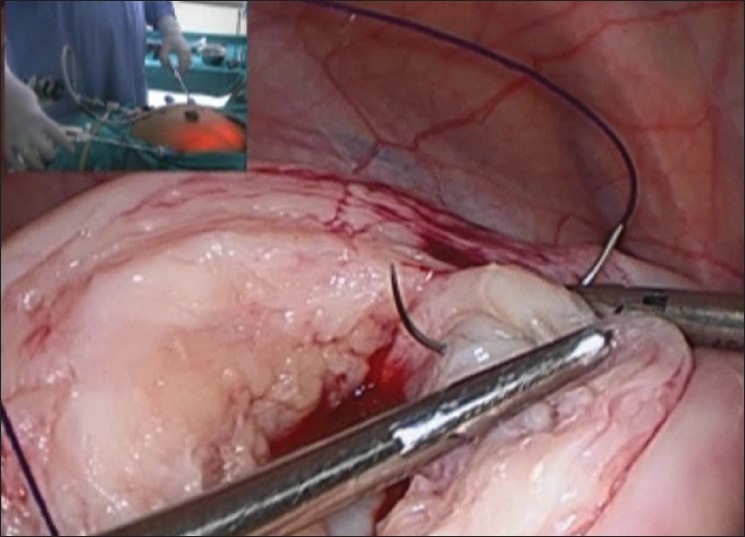
As the uterus is cut, instead of bleeding, saline leakage takes place. This helps to keep the field clear and it is easier to get the correct plane between the fibroid and the myometrium. The separation of the fibroid is helped due to the dissection of the correct plane by the saline injection [Figures 4–7]. For enucleation of fibroid, traction is given with a myoma screw and countertraction given with a suction cannula or a toothed needle holder [Figures 8 and 9].
Figure 4.

Cutting only with scissors
Figure 7.
No bleeding from myometrium
Figure 8.
Large anterior wall fibroid removed
Figure 9.
No bleeding from base
Figure 5.
Plane easily identifiable
Figure 6.
No bleeding in separation
Mainstay of hemostasis in laparoscopic myomectomy is suturing. Once the fibroid is separated, myometrium is sutured by barbed suture material [Figures 10–13].
Figure 10.
Barbed suture first layer continuous
Figure 13.
Morcellation
Figure 11.
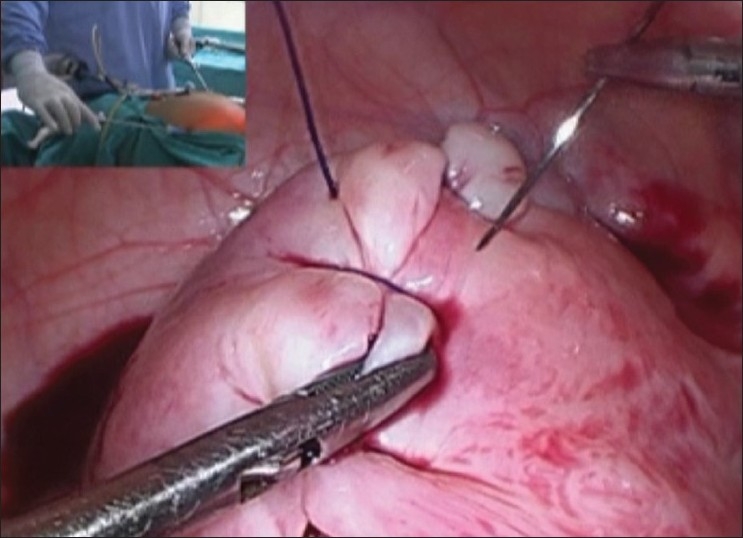
Barbed suture second layer continuous
Figure 12.
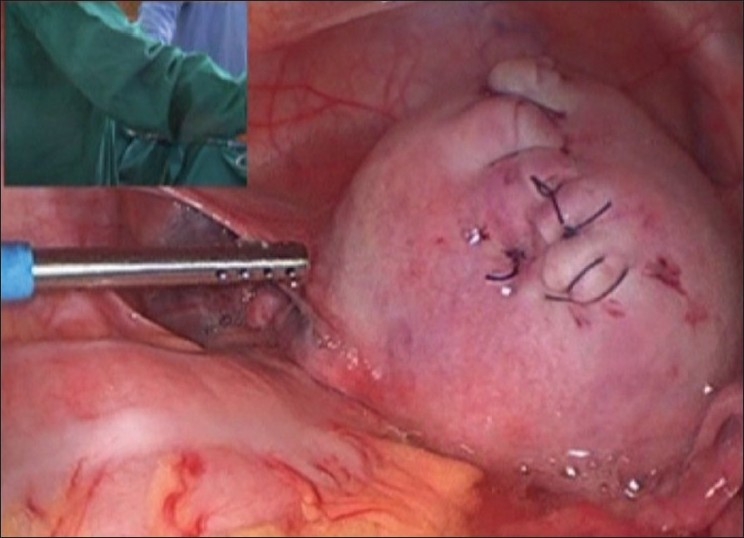
Suturing completed in two layers
The barbed suture
It is a monofilament absorbable suture with barbs on it. Suture has needle on both ends. Barbs on one side of the center are in one direction and on the other side of the center are in the opposite direction. These barbs make the suture grip the tissue, without allowing the suture to slip back or become loose. Barbs allow the suture to be pulled in one direction only till the center of the suture is reached. Suture cannot be pulled back in the reverse direction, so this helps in excellent approximation of myometrial edges without any need to follow the suture material to hold it tight. Continuous suturing thus becomes very easy. There is no need to tie a knot in the end. There are two patterns in which the defect can be closed: first is the shoelace pattern starting from one end of the defect and the second one is to start from the center of the defect and go up with one end of the suture and down with the other end. Another advantage of Quill is that it distributes the tension within the wound. The entire suture line grips the myometrial tissue. Tension is not just at the knots, but along the entire length of the suture.
By the time suturing is completed, the effect of vasopressin and saline is partially worn off. We see that the uterus regains its color, indicating that the blood flow which was temporarily reduced to the myometrium has returned. But no bleeding occurs from the suture line due to good approximation of myometrial edges and excellent hemostasis.
The advantages
Myomectomy without energy source: Only a pair of simple scissors is used to cut the myometrium. Neither a monopolar hook nor a harmonic is used. As no energy source is used for cutting or coagulation, no dead or scarred tissue is left behind. Thus, there is better tissue healing, better scar integrity and less chances of scar dehiscence.
Enucleation of myoma is easy as the saline and vasopressin solution partially dissects the myoma–myometrial interface.
Chances of endometrial avulsion reduced: In cases of intramural myomas, those with a submucus component, the incidence of avulsion of endometrium is minimized. The saline–vasopressin solution enters the plane between the myoma and endometrium and pushes the endometrium down and away and thus the myoma is easily peeled off.
Reduced blood loss: Usually 300–400 ml of blood loss may be seen during a myomectomy, but with the use of aquadissection technique, this figure is reduced to less than 100 ml which holds a lot of significance for both patient and surgeon.
Easy suturing of myometrial defect: As the field is very clear due to almost no bleeding, myometrial defect closure becomes very convenient, and the surgeon need not hurry to place the sutures for hemostatic purpose.
The concerns
The main concern with the use of vasopressin is that it causes sudden rise in blood pressure, if it is accidentally injected directly into a blood vessel. This complication can be avoided by simply aspirating before injecting.
There are concerns regarding the cardiac effect of vasopressin. Myocardial vessel constriction may mimic transient myocardial ischemia. This will manifest as ST segment depression on ECG monitoring. This may last for upto 20 min, till the effect of vasopressin wears off. However, ECG changes were not seen intraoperatively with the use of vasopressin at our center. Sometimes, severe transient peripheral vasoconstriction occurs with the use of vasopressin. In this case, pulse oximeter may not show proper reading for a short period.
If we only use 400 ml of saline without vasopressin, then the effect of hemostasis will only be effective for 5–10 min, during which time it is washed out from the tissues and bleeding starts while the surgery is still on.
OBSERVATIONS
A total of 157 patients with fibroid, who underwent laparoscopic myomectomy at this center in the last 18 months with the use of technique of aquadissection and barbed suture, were evaluated.
It was found that the blood loss ranged from 20 to 250 ml. The operating time was 50-100 mins. No hemorrhagic complication occurred in any patient during surgery or postoperatively. In none of the cases, blood transfusion was required during or after surgery. There was neither any bowel or bladder injury nor any anesthetic complication. None of the patients required readmission or any repeat surgical or medical intervention postoperatively.
With the use of barbed suture, the closure of myometrial defect was very easy and comfortable. The approximation of myometrial edges was very good and the total time required to close the defect was decreased significantly.
As a routine, transvaginal sonography was done after 3 months of surgery which revealed normal sized uterus with no collection or hematoma. Four of the myomectomy patients conceived and delivered by cesarean section. No adhesions were found on the myomectomy scar.
CONCLUSION
Aquadissection technique for myomectomy is effective in markedly reducing blood loss during surgery. It reduces the time taken for myomectomy. It shortens the recovery time. It also ensures better wound healing postoperatively.
The use of barbed sutures decreases the total time taken for myometrial defect closure.
REVIEW OF LITERATURE
Use of vasoconstrictive agent
Aquadissection is a technique where for a myoma size of 8 cm, 40 units of inj. vasopressin is diluted in 400 ml of normal saline and injected between the uterus and the myoma. Vasopressin has been used for myomectomy for a long time now.
Local administration of vasopressin to the uterus is a safe and effective hemostatic technique for controlling regional blood flow from the utrine artery to peripheral blood vessels, without having a significant effect on systemic circulatory dynamics. Shimanuki et al.[1] studied the effect of vasopressin on local and general circulation during laparoscopic surgery. Systolic/diastolic blood pressure tended to increase immediately after vasopressin administration, but the increase was not significant.
Vasopressin is effective in preventing blood loss and reducing the need for blood transfusion during myomectomy. Frederick et al.[2] conducted a study as early as in 1994 to assess the efficacy of intramyometrial vasopressin for minimizing bleeding and its sequelae at myomectomy. A randomized placebo-controlled trial was done. Myomectomy was done after the intramyometrial injection of either 20 units vasopressin diluted to 20 ml in normal saline or placebo (20 ml NS). The use of vasopressin resulted in median blood loss of 225 ml compared to 675 ml in the placebo group.
Sizzi et al.[3] conducted an Italian multicenter study of complications in 2050 laparoscopic myomectomies, which had the use of vasoconstrictive agent in 37% cases to reduce the operative time. The conclusion was that the operating time for the enucleation of a fibroid was reduced with the use of vasoconstrictive agent. Laparoscopic myomectomy, when performed by an experienced surgeon, can be considered a safe technique with an extremely low failure rate and good results in terms of pregnancy outcome.
The injection of Bupivacaine plus epinephrine during laparoscopic myomectomy is also effective in reducing blood loss, total operative and enucleation time, degree of surgical difficulty and postoperative pain. Zullo Fulvio et al.[4] enrolled 60 premenopausal women with uterine leiomyomas in a randomized controlled design and intraoperatively treated them with injection of Bupivacaine plus epinephrine (Group A) or saline solution (Group B) during laparoscopic myomectomy. Blood loss, total operative and enucleation time, and degree of surgical difficulty were significantly (P<0.05) lower in group A than in group B. The number of vials of pain medication used postoperatively was significantly (P<0.05) lower in group A than in group B.
Assessment of different hemostatic methods used in laparoscopic intramural myomectomy was done by Lin et al.[5] in China in 2008. The study was conducted in 280 women. Four groups were formed: group A: underwent fibroid pedicle ligation; group B: injected 12 IU diluted vasopressin around myoma; group C: injected 20 IU oxytocin with pedicle ligation; group D: vasopressin with pedicle ligation. The amount of blood loss in group A (171±146 ml) and group C (184±140 ml) both were significantly higher than those in group B (115±70 ml) and group D (106±73 ml). They concluded that vasopressin (12 IU) injection around myoma is a simple, effective and safe hemostatic procedure during laparoscopic myomectomy.
There are concerns regarding use of vasopressin in laparoscopic myomectomy. Local intramyometrial infiltration of low-dose vasopressin may cause lethal cardiopulmonary complications. Hobo et al.[6] reported bradycardia and cardiac arrest caused by intramyometrial injection of vasopressin during a laparoscopically assisted myomectomy. Vasopressin was used at a total dose of 11 units (0.2 units/ml). The patient was successfully resuscitated.
In another case report by Kitamura et al.,[7] vasopressin injection for laparoscopic myomectomy caused sudden fall in blood pressure and heart rate. ECG showed ST segment depression and premature ventricular contractions. Patient was administered nicorandil 3 mg followed by continuous infusion at a rate of 3 mg/hr, and lidocaine 60 mg, intravenously. The ST depression and premature ventricular contraction disappeared immediately. Intramyometrial injection may cause increase in blood concentration of vasopressin which might cause vasoconstriction of coronary arteries, increase in afterload and/or myocardial depression, resulting in decreased cardiac output.
Laparoscopic myometrial defect closure
Einarsson et al.[8] conducted a retrospective analysis of 138 consecutive laparoscopic myomectomies performed by a single surgeon over 3 years. Use of bidirectional barbed suture was found to significantly shorten the mean (SD) duration of surgery.
The advent of barbed suture is a landmark in laparoscopic myometrial defect closure. Greenberg et al.[9] in 2008 reported the bidirectional barbed suture as the new design that incorporates tiny barbs spaced evenly along the length of the suture cut facing in opposite directions from the midpoint. Unlike the smooth-textured traditional suture, the bidirectional barbs on this new product introduce a new paradigm in which wound tension is evenly distributed across the length of the suture line rather than at the knotted end. No knots are required with bidirectional barbed suture.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Shimanuki H, Takeuchi H, Kitade M, Kikuchi I, Kumakiri J, Kinoshita K. The effect of vasopressin on local and general circulation during laparoscopic surgery. J Minim Invasive Gynecol. 2006;13:190–4. doi: 10.1016/j.jmig.2006.01.015. [DOI] [PubMed] [Google Scholar]
- 2.Frederick J, Fletcher H, Simeon D, Mullings A, Hardie M. Intramyometrial vasopressin as a haemostatic agent during myomectomy. Br J Obstet Gynaecol. 1994;101:435–7. doi: 10.1111/j.1471-0528.1994.tb11918.x. [DOI] [PubMed] [Google Scholar]
- 3.Sizzi O, Rossetti A, Malzoni M, Minelli L, La Grotta F, Soranna L, et al. Italian multicenter study on complications of laparoscopic myomectomy. J Minim Invasive Gynecol. 2007;14:453–62. doi: 10.1016/j.jmig.2007.01.013. [DOI] [PubMed] [Google Scholar]
- 4.Zullo F, Palomba S, Corea D, Pellicano M, Russo T, Falbo A, et al. Bupivacaine plus epinephrine for laparoscopic myomectomy: A randomized placebo-controlled trial. Obstet Gynecol. 2004;104:243–9. doi: 10.1097/01.AOG.0000132801.41880.e8. [DOI] [PubMed] [Google Scholar]
- 5.Lin XN, Zhang SY, Fang SH, Wang MZ, Lou HY. Assessment of different homeostatic methods used in laparoscopic intramural myomectomy. Zhonghua Yi Xue Za Zhi. 2008;88:905–8. [PubMed] [Google Scholar]
- 6.Hobo R, Netsu S, Koyasu Y, Tsutsumi O. Bradycardia and cardiac arrest caused by intramyometrial injection of vasopressin during a laparoscopically assisted myomectomy. Obstet Gynecol. 2009;113:484–6. doi: 10.1097/AOG.0b013e318187e795. [DOI] [PubMed] [Google Scholar]
- 7.Kitamura T, Saito Y, Yamada Y. Severe hypotension as a complication of intramyometrial injection of vasopressin: A case report. Masui. 2008;57:1517–20. [PubMed] [Google Scholar]
- 8.Einarsson JI, Chavan NR, Suzuki Y, Jonsdottir G, Vellinga TT, Greenberg JA. Use of bidirectional barbed suture in laparoscopic myomectomy: Evaluation of perioperative outcomes, safety, and efficacy. J Minim Invasive Gynecol. 2011;18:92–5. doi: 10.1016/j.jmig.2010.10.003. [DOI] [PubMed] [Google Scholar]
- 9.Greenberg JA, Einarsson JI. The use of bidirectional barbed suture in laparoscopic myomectomy and total laparoscopic hysterectomy. J Minim Invasive Gynecol. 2008;15:621–3. doi: 10.1016/j.jmig.2008.06.004. [DOI] [PubMed] [Google Scholar]