

Abstract
Objectives
The UAE has undergone remarkable economic and social transformations over the past few decades. We present findings on the prevalence of overweight and obesity, dietary and activity patterns among Emiratis in 2009/10, and explore associated urbanization and wealth factors.
Methods
A cross-sectional study was conducted in 628 randomly-selected households in all seven emirates. Sociodemographics, 24-hour dietary recalls, physical activity and anthropometric data were collected from adult females (≥19y), adolescents (11-18y) and children (6-10y) in each family via in-person interviews using validated questionnaires.
Results
In 2009/10, 65% of adult women, 28% of male adolescents and 40% of female adolescents, 25% of male children and 41% of female children were overweight or obese. 43% of girls and 38% of boys (6-10y) consumed more calories than their estimated energy requirements. Snacking represents a major source of Emirati caloric intake (>20%) of total calories. In addition, caloric beverages account for 8-14% of total calories. Meanwhile, physical activity levels are low, especially among females Emiratis and those living in urban areas.
Conclusions
These trends represent the potential risk for severe cardio-metabolic problems in the UAE. The significant gender differentials among children and adolescents are driven by diet and activity differences. More attention should be paid to educate the public on nutrition (e.g., limit the consumption of sugared sodas, fruit drinks and whole milk, promote water and low-fat/skim milk consumption instead) and encourage physical activity from a young age, especially among females. Built environments and social support for improved lifestyle choices by individuals are needed.
Keywords: Nutrition transition, obesity, diet, activity, UAE
INTRODUCTION
The countries in the Arabian Gulf region – Bahrain, Kuwait, Qatar, Oman, Saudi Arabia, and the United Arab Emirates (UAE) – have experienced a rapid transition from a traditional semi-urbanized life to a modern and urbanized society following major discoveries of oil since the 1960s (International Monetary Fund 2009) with a concomitant rise in the prevalence of obesity, and other cardio-metabolic problems (Ng 2010). Minimal research has focused on dietary and physical activity patterns in the region, despite large numbers of studies on obesity (Ng 2010).
The UAE presents a number of factors that contribute to the rising rates of obesity and nutrition related non-communicable diseases (NR-NCDs). Among the dietary causes noted are frequent snacking (Amine and Samy 1996, Musaiger and Radwan 1995), the replacement of traditional foods with energy-dense fast foods, and water with soft drink consumption (Amine and Samy 1996, Kerkadi 2003, Musaiger and Abuirmeileh 1998, Rabbia et al 2004, UAE-GSHS 2005, UAEHALS 2000) and low fruit and vegetable intake (Rabbia et al 2004, UAE-GSHS 2005, Zaghloul et al In press). In addition, reduced physical activity due to inactive occupations, rare participation in sports and sedentary leisure have been blamed (Rabbia et al 2004, UAE-GSHS 2005, UAEHALS 2000, Wasfi et al 2008).
A nationally representative survey undertaken in the UAE in 2009/10 describes the estimated prevalence of overweight and obesity and the dietary and activity patterns for adult females, children and adolescents. We also explore how some underlying factors (e.g., urbanization and wealth) are associated with the shift from a presumably healthier lifestyle to one linked with an advanced stage of the nutrition transition.
METHODS
This study was approved by the Institutional Review Boards (IRB) of UNC and the UAE University Faculty of Medicine. Interviews were conducted in Arabic, with study questionnaires and informed consents written in both Arabic and English.
Study sample
This study used a nationally representative random sample of urban and rural Emirati households from all seven Emirates (Abu Dhabi, Dubai, Sharjah, Fujairah, Ras al Khaimah, Ajman, and Umm al Quwain). The 14 strata were divided into primary sampling units (PSUs), which consisted of a census enumeration area in the urban areas or a village in the rural areas. All Emirati households residing in PSUs with at least eight Emirati households were considered the target population. Using the May 2005 and 2008 UAE census, the Ministry of Economy (MOE) randomly selected 200 PSUs. The study teams approached 827 Emirati households; 628 households (3,820 Emirati citizens) agreed to participate, with a household response rate of 75%.
Data collection
All survey materials and protocols were piloted and adjusted over the 6-months prior to survey implementation, including three weeks of training for all staff. Collection of nutrition-related data (diet recall, physical activity and anthropometry) was obtained from one female adult (≥ 19y), one adolescent (11-18y) and one child (6-10y), who were randomly selected from each household. In the case of children (6-10y), the mother or primary caregiver provided information regarding physical activity and diet. We did not collect nutrition-related data from adult males due to their involvement in other aspects of the survey, which might have deterred them from agreeing to allow other household members to participate.
Physical activity
The International Physical Activity Questionnaire (IPAQ) short form asks about the frequency (days during the last 7 days) and duration of three types of activities: walking, moderate-intensity activities (e.g., jumping rope, tennis, bicycling at a regular pace) and vigorous-intensity activities (e.g., fast bicycling or aerobics) (Booth 2000). To ensure relevance, we provided examples that were more reflective of the region and appropriate for the various age groups (6-10y, 11-18y, ≥ 19y). The IPAQ sitting question is an additional indicator variable of time spent in sedentary activity to provide a separate construct regarding lifestyle since inactivity is not merely the opposite of activity (Dietz 1996). The IPAQ has been used in surveys globally, including the WHO World Health Surveys (WHO), and has been validated for a number of different populations, including those from the Arabian Gulf (Al-Hazzaa 2007, Craig et al 2003, Hagströmer et al 2006, Hallal and Victora 2004, Qahoush et al 2010). Our analysis of the data followed the “Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire” (IPAQ Research Committee 2005).
Dietary data collection
The 24-hour dietary recall and data processing procedures were based on methods developed in Kuwait. Dieticians brought food models, measuring cups, spoons, bowls and plates to help respondents determine portion sizes and used a specially designed Food Instruction Booklet (Kuwait Institute for Scientific Research 2010), which follows the US Department of Agriculture’s five-steps multiple pass method (Moshfegh et al 2008, Raper et al 2004). The method standardizes data collection by using a sequence of probing questions to guide the respondent through the 24-hour reference period more than once; this procedure gives the respondent several opportunities to remember food details, amounts, and additional foods. All data were cross-checked by supervisory staff, and respondents were re-contacted (if necessary) before data entry. Data coders used the ESHA Research Food Processor® SQL and ESHAPort® SQL software, which already contained a food composition database of over 35,000 food items with data from more than 1,500 sources, including the latest USDA Standard Reference database, items from the US individual consumption survey databases, manufacturer’s data, data from fast food companies and data from literature sources (ESHA Research 2006). The team updated this with detailed nutritional information from over 100 composite Kuwaiti dishes that underwent nutritional analysis by the Kuwait Institute for Scientific Research (Al-Amiri et al 2009, Dashti et al 2003, Dashti et al 2004, Dashti et al 2001, Kuwait Institute for Scientific Research 1998) to provide data coders with a culturally representative collection of food items. In addition, additional local Emirati recipes and dishes collected during the pilot and throughout the data collection process were added. All entered data were checked in the UAE and by senior project staff (Kuwait and US) before it was finalized. Based on the final data, total calories, macronutrient and micronutrient content of the foods consumed by food group, by meal and for each individual were derived.
Anthropometry
Height, weight and waist circumference were measured by trained nurses using easily portable medical equipment (stadiometers, digital floor scales, and girth measuring tapes). Nurses took at least two measurements each for height, weight and waist circumference. A third measurement was taken if the difference between first two was greater than 0.5cm for height, 0.5kg for weight, and 1.0cm for waist circumference, following standard protocols. WHO cutoffs were used for adults (WHO 2000) with overweight defined as 25 ≤ BMI < 30, and obesity defined as BMI ≥ 30. Among children and adolescents (<19y), the International Obesity Task Force (IOTF) cutoffs (Cole et al 2000) were used.
Sociodemographic measures
Location of residence was based on census classifications. For all adults, location of the respondent at birth, timing of migration, household income and education of each individual respondent were also obtained. Using a collection of measures on household income, assets, housing type and household size, we conducted Principal Component Analysis to create a wealth index (Vyas and Kumaranayake 2006) and categorized households into quintiles (Q1= least wealthy; Q5=wealthiest).
Analyses
All analyses results were corrected using sampling weights, clustered by PSUs, and took into account the two strata sampling design. The analyses excluded the disabled (e.g., missing limb) and women who were pregnant or lactating at the time of the survey. Analyses were conducted in Stata version 11 (StataCorp 2009) using the -svy- commands.
RESULTS
Of those selected for interviews, 478 women (91%), 276 adolescents (83%) and 253 children (100%) completed dietary recalls, physical activity and anthropometry components of the study.
Obesity prevalence estimates
Table 1 shows that in 2009/10, 65% of adult Emirati women in the UAE are overweight or obese. Only 30% of adult Emirati women in the UAE are normal weight, and 5% are underweight. Among Emirati adolescents, 20.5% of females are overweight and 19.7% are obese; 16.2% of adolescent males are overweight and 11.7% are obese. Among Emirati children, 40.7% of female children and 25% of male children are overweight or obese.
Table 1. Survey weighted descriptive statistics by gender-age group, survey weighted means (SE).
| Gender-age group | Adult Female (≥19y) |
Adolescent (11-18y) |
Child (6-10y) |
||
|---|---|---|---|---|---|
| Female | Male | Female | Male | ||
| Anthropometry | |||||
| % Underweight (BMI ≤18.5) | 4.6 | 14.3 | 12.0 | 16.5 | 17.4 |
| % Normal weight (18.5≤BMI <25) | 29.7 | 45.5¥ | 60.1 | 42.8¥ | 56.6 |
| % Overweight (25≤BMI <30) | 31.4 | 20.5¥ | 16.2 | 23.6¥ | 9.1 |
| % Obese (BMI ≥30) | 34.2 | 19.7¥ | 11.7 | 17.1 | 15.9 |
| % High waist circumference (≥88cm) | 53.2 | - | - | - | - |
| Mean BMI (kg/m2) | 28.8 (0.8) |
23.5 (1.1) |
21.9 (0.6) |
17.3 (0.6) |
17.5 (0.5) |
|
| |||||
| Diet | |||||
| Total caloric intake (kcal) | 1725.8 (56.0) |
1791 .2¥ (79.6) |
1954.4 (119.7) |
1649.4 (108.6) |
1696.9 (66.7) |
| % Energy from fat | 24.8 | 27.8 | 25.8 | 25.6 | 26.3 |
| % Energy from protein | 16.7 | 14.9 | 16.0 | 15.3 | 14.4 |
| % Energy from carbohydrates | 59.2 | 58.2 | 59.1 | 60.5 | 60.4 |
| % over-consume relative to EER | 32.1 | 33.5¥ | 15.9 | 43.2¥ | 38.2 |
|
| |||||
| Physical Activity/Inactivity | |||||
| % low physical activity level | 58.8 | 46.7¥ | 22.5 | 34.9¥ | 18.9 |
| % moderate physical activity level | 25 | 35.6¥ | 24.8 | 26.8¥ | 19.8 |
| % high physical activity level | 16.2 | 17.8¥ | 52.7 | 38.3¥ | 61.3 |
| Mean | 254 (50) |
360 (101) |
246 (90) |
392¥ (46) |
212 (23) |
| Minutes spent sitting/ weekday | |||||
| 25 %tile | 180 | 300 | 120 | 210 | 90 |
| Median | 240 | 420 | 240 | 390 | 210 |
| 75 %tile | 360 | 570 | 480 | 480 | 300 |
|
| |||||
| Other characteristics (among adult women only) | |||||
| % urban 60.6 | - | - | - | - | |
| Household size | 7.9 (0.8) |
- | - | - | - |
| % Household income <30,000 AED | 60.6 | - | - | - | - |
| % Household income 30,000-50,000 AED | 15.4 | - | - | - | - |
| % Household income 50,000-100,000 AED | 10.9 | - | - | - | - |
| % Household income >100,000 | 13.1 | - | - | - | - |
| % Married | 52.2 | - | - | - | - |
| % Employed outside home | 24.2 | - | - | - | - |
| % Currently a student | 12.5 | - | - | - | - |
| % with University education or higher | 34.4 | - | - | - | - |
|
| |||||
| Sample Size | 478 | 143 | 133 | 126 | 127 |
Notes: Figures in parentheses are standard errors based on survey weights.
Significantly different (p<0.05) from males from the same age group
Dietary factors
Caloric intake
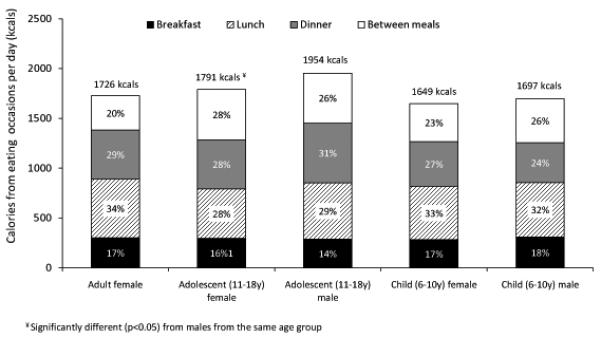
From dietary recalls, total calories and sources of calories consumed by participants showed that the average daily total caloric intake is highest for adolescent Emirati boys (1,954 kcal/day), while young Emirati girls have the lowest daily caloric intake (1,649 kcals/day). Using standard formulas to estimate energy requirements (EER) based on age, gender, physical activity score, height and weight (Institute of Medicine 2002), we determined the proportion of respondents that consumed more calories than their estimated energy requirements. We found that a large percentage of Emirati children (43.2% of girls and 38.2% of boys 6-10y) consumed more calories than needed. About a third of Emirati adolescents and adult females also consume more calories than needed; 16% of adolescent males do so. In addition, a significantly higher proportion of female Emirati adolescents and children over-consumed compared to their male counterparts (p<0.05).
Snacking
Across all gender-age groups, the norm appears to be around four eating occasions a day with an average of 1.5 snacks. As shown in Figure 1, snacking represents a major source of Emirati caloric intake, making up 500 kcal (26-28%) of total calories consumed by Emirati adolescents. Among Emirati children, 23-26% of all calories are consumed between meals, and among adult Emirati women 20% of calories are consumed between meals.
Figure 1. Calories consumed at different eating occasions by gender-age group.
Caloric beverages
Calories from beverages appear to be one of the major contributors to total calories, comprising 8% of total calories for adult Emirati women but up to 14% for male Emirati children. Figure 2 shows that sugared sodas and fruit drinks (e.g., cola, root beer, orange squash) account for the majority (40-71%) of liquid beverages. In addition, whole milk, as opposed to low-fat milk, contributes to a higher proportion of the total daily liquid caloric intake among Emirati children (44-69 kcals/day from whole milk versus 3-6 kcals/day from low-fat milk).
Figure 2. Calories from beverages by gender-age groups.
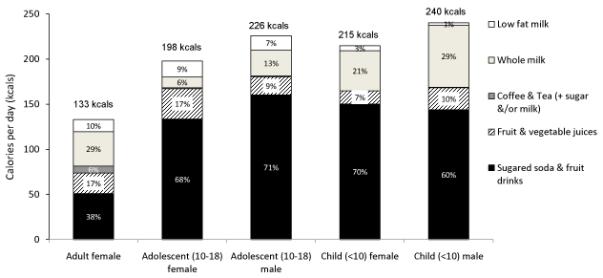
Note: Low fat milk include plain or flavored milks that contained skim milk and ≤2% milk fat; Whole milk include plain or flavored milks that contain >2% milk fat; Coffee & tea includes beverages that are primarily coffee or tea, and includes these beverages when sugar and/or milk have been added; Fruit and vegetable juices include 100% juice, and juice mixes, nectars (25-99% juice) either from concentrate, reconstituted or not-from-concentrate (freshly squeezed); Sugared soda and fruit drinks included carbonated and non-carbonated sweetened drinks such as colas and fruit drinks (<25% juice) or fruit flavor drinks (without any juice).
Physical activity factors
Activeness
Table 1 also shows the breakdown of low-moderate-high physical activity levels by gender-age groupings. Only 41% of the adult Emirati women have moderate or high levels of physical activity. A significantly lower proportion of Emirati girls engage in moderate and high levels of physical activity compared with boys (53-63% versus 77-81%, p<0.05). Physical activity levels are decreasing across age groupings (from children to adolescents to adults) for females.
Sedentariness
This study found that female Emirati children and adolescents spend more time sitting compared to male Emirati children and adolescents on average. The 25th percentile of time spent sitting indicates that 75% of female Emirati adolescents spent >5 hours sitting per weekday compared to less than 50% of male Emirati adolescents who do so (Table 1). Meanwhile, the 75th percentile of time spent sitting indicates that 25% of adult Emirati females sit for >6 hours/weekday, 25% of adolescent females sit for >9.5 hours/weekday, and 25% of female children sit for >8 hours/weekday.
Underlying factors
Urbanization
Among adult Emirati women, urban residents have lower caloric intake compared to those living in rural areas (by 115 kcals/day), but the overall compositions are similar (Table 2). Adult Emirati women living in urban areas are far less likely to engage in moderate to high levels of physical activity. However, when location and history of residency (5 years ago) were taken into consideration, a slightly different picture emerges. Those who always lived in villages had the lowest total caloric intake and lowest proportion of diet comprised of fat. Otherwise, among the other groups, total calories and diet composition did not vary greatly. Similarly, women who remained in villages, relocated from settlements/villages to towns, or relocated from towns or cities to settlements/villages had much higher levels of physical activity. Meanwhile, female respondents who remained in small or large towns or cities, and those who relocated into cities had considerably lower levels of moderate or high physical activity and higher prevalence rates of overweight and obesity (Table 2).
Table 2. Weight Status, diet and physical measures by residence and wealth quintile among adult Emirati women 19-50y, survey weighted means (SE).
| Urban | Rural | Stayed in village‡ |
Stayed within town/ city‡ |
Relocated from settlement /village to town‡ |
Relocated from settlement/ village to city‡ |
Relocated from town to city‡ |
Relocated from town or city to village‡ |
Q1 (Poorest 20%) |
Q2 (20-40 %tile) |
Q3 (40-60 %tile) |
Q4 (60-80 %tile) |
Q5 (Wealthiest 20%) |
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weight Status | |||||||||||||
| % Underweight (BMI ≤18.5) | 3.1 | 7.7¥ | 9.3 | 1.8 | 12.8 | 7.8 | 0.0 | 40.7 | 3.3 | 1.0 | 8.7§ | 4.5 | 4.6 |
| % Normal weight (18.5≤BMI <25) | 29.8 | 28.5 | 21.7 | 35.9 | 36.5 | 0.5 | 23.4 | 39.9 | 24.0 | 29.1 | 18.5§ | 18.4§ | 48.9 |
| % Overweight (25≤BMI <30) | 40.0 | 25.2¥ | 25.5 | 31.3 | 1.4 | 50.2 | 64.2 | 6.4 | 44.4 | 31.3 | 38.3§ | 38.1§ | 20.6 |
| % Obese (BMI ≥30) | 27.1 | 38.5¥ | 43.4 | 31.0 | 49.2 | 41.4 | 12.4 | 13.0 | 28.3 | 38.6 | 34.5 | 39.0§ | 25.9 |
| Diet | |||||||||||||
| Total calories (kcal) | 1680.4 (76.4) |
1795.4¥ (79.4) |
1449.6 (104.2) |
1769.4 (82.8) |
1661.4 (128.7) |
1786.8 (213.3) |
1907.1 (191.7) |
2055.3 (425.1) |
1819.9 (125.8) |
1521.6 (124.9) |
1475.0§ (111.1) |
1514.4 (74.6) |
1953.9 (108.4) |
| % Energy from fat | 24.9 | 24.6 | 22.1 | 25.0 | 24.3 | 28.4 | 25.4 | 27.5 | 25.1 | 22.9 | 22.8 | 25.9 | 24.8 |
| % Energy from protein | 17.0 | 16.1 | 16.5 | 16.7 | 13.5 | 17.3 | 17.7 | 16.3 | 17.9 | 16.9 | 14.9 | 15.8 | 17.1 |
| % Energy from carbohydrates | 58.6 | 60.2 | 62.3 | 58.9 | 63.2 | 56.1 | 57.7 | 56.4 | 57.6 | 60.8 | 63.0 | 58.8 | 58.8 |
| Leisure-time Physical Activity | |||||||||||||
| % Low level | 62.9 | 52.2¥ | 33.7 | 64.3 | 28.4 | 74.2 | 76.3 | 21.4 | 73.5 | 45.9§ | 49.4§ | 49.0§ | 76.7 |
| % Moderate level | 24.1 | 26.5 | 28.0 | 23.9 | 55.8 | 20.5 | 22.2 | 38.2 | 10.5 | 32.1§ | 26.8 | 28.5 | 17.7 |
| % High level | 13.0 | 21.3¥ | 38.3 | 11.9 | 15.8 | 5.3 | 1.5 | 40.4 | 16.0§ | 21.9§ | 23.8§ | 22.5§ | 5.5 |
| Mean Sitting (min) | 321.3 (25.8) |
314.6 (24.8) |
246.4 (34.3) |
280.3 (30.6) |
426.5 (103.4) |
324.8 (33.1) |
260.1 (58.9) |
376.9 (69.7) |
193.9§ (14.2) |
232.0 (25.0) |
327.4 (41.3) |
347.4 (38.4) |
287.4 (29.8) |
| Median Sitting (min) | 240 | 240 | 240 | 240 | 360 | 270 | 285 | 255 | 180 | 240 | 240 | 270 | 240 |
|
| |||||||||||||
| Sample size | 188 | 151 | 60 | 191 | 29 | 18 | 26 | 18 | 59 | 75 | 70 | 62 | 86 |
Notes: Excludes women who were pregnant, lactating or disabled during the survey. Figures in parentheses are standard errors based on survey weights.
Significantly different (p<0.05) from urban adult Emirati women. In looking at the difference among rural and urban adult women by the 19-34y and the 35-50y age groups, there are significant differences for women living in urban areas by these age groups for the prevalence of normal weight (43% vs. 15%) and obesity (19% vs. 46%), but no differences with regards to diet and physical activity. For women living in rural areas, the prevalence of overweight (22% vs. 36%) and obesity (29% vs. 53%) were significantly different between the 19-34y and the 35-50y women, but none of the diet or physical activity measures were significantly different by age groups.
Significantly different (p<0.05) from Q5 - wealthiest 20%
Residency categorizations were based on population size, and were set by the Statistics Center of Abu Dhabi. Settlements/villages were areas ≤10,000 people; Towns included small towns (10,000-24,999 people) and large towns (25,000-49,999 people); and Cities included those >50,000 people.
Wealth
In the UAE, all Emiratis receive benefits including education, housing, subsidized utilities, and monthly stipends from the government. Thus, the wealth associations may not be as prominent as elsewhere. We found that total calories declined with wealth until the second highest wealth quintile (Q4), where the proportion of energy from fat was the highest (Table 2). In addition, the wealthiest households had the highest caloric intake while, women from households with the 40th to 60th percentile of wealth had the lowest average caloric intake, and the highest proportion of their diets coming from carbohydrates. For physical activity, similar U-shaped associations between household wealth and high physical activity, and with sedentariness exist. Adult Emirati women from the poorest (Q1) and wealthiest (Q5) households have very low levels of moderate to high physical activity. In addition, inactivity measured by time spent sitting increases with wealth until the 4th wealth quintile (Table 2).
DISCUSSION
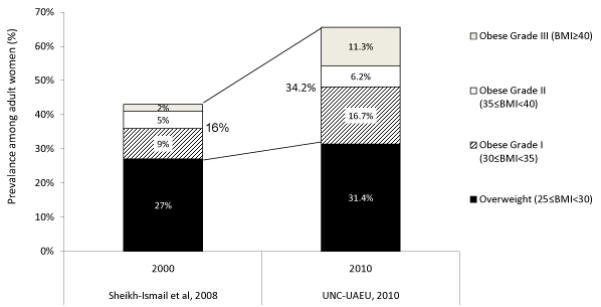
The UAE has undergone a remarkable economic and social transformation in a short 30-40 year period. Meanwhile, the prevalence of obesity and overweight in the Emirati population is high and has increased over time. Among adult Emirati women, 65% are currently overweight or obese, and compared to 2000 estimates (Sheikh-Ismail et al 2008) (Figure 3). While the overweight prevalence increased slightly from 27% to 31%, obesity nearly doubled from 16% to 34%, with grade III obesity (BMI ≥ 40) rising the most dramatically from 2% in 2000 to over 11% in 2010 (Figure 3). Indeed, the prevalence of overweight, and various grades of obesity among women in the UAE are comparable to women in the US, which was estimated to be 64% overweight or obese, 36% obese, 18% with grade I obesity, 11% with grade II obesity and 7% with grade III obesity in 2008 (Flegal et al 2010).
Figure 3. Adult female overweight and obese prevalence (2000 vs. 2010).
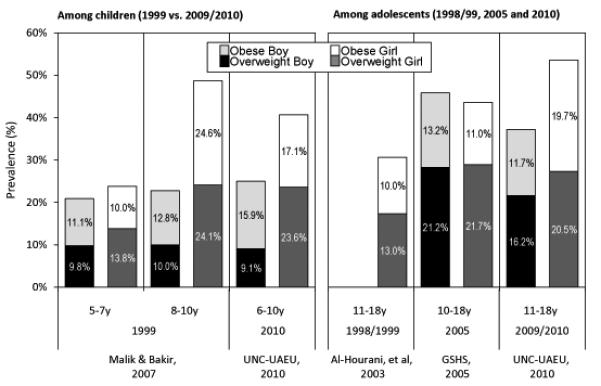
Compared to findings from the 1998-1999 study (Al-Hourani et al 2003) and the 2005 Global School-based Student Health Survey (UAE-GSHS 2005), the present study shows that the prevalence of overweight rose among Emirati adolescent girls from 1999 to 2005 but has stayed around 21% since. Obesity has risen dramatically, particularly from 2005 to 2009/10, when it almost doubled (Figure 4). Among Emirati adolescent boys, both overweight and obesity declined slightly in 2010 compared to 2005 estimates. The gender difference, which did not exist in 2005, appeared between boys and girls in 2009/10 and is much larger compared to other countries, such as the United States (Ogden et al 2010). Other Arabian Gulf countries have also observed similar gender differential in prevalence of overweight and obesity between male and female across most age groups (Ng 2011), suggesting that the context of the Arabian Gulf may be particularly conducive for females to be overweight or obese. Among children, this study’s estimates for girls are similar to past estimates based on 1999 data (Malik and Bakir 2007), and exhibit slight increases in the prevalence of overweight and obesity among boys (Figure 4).
Figure 4. Prevalence of overweight and obesity among adolescents and children by gender.
A number of factors at the individual, home, community, societal, economic and environmental levels might contribute to the rising rates of overweight, obesity and nutrition related non-communicable diseases. At the individual level, increased snacking, high levels of caloric beverages, and reduced activities are likely factors that account for these trends. Snacking presents a very large proportion of calories for Emirati. Even though respondents reported only 1.5 snacks/day, these numbers reflect a level of caloric intake from snacks as high as the United States (Piernas and Popkin 2010a, Piernas and Popkin 2010b), even though Americans have twice the number of eating occasions compared to Emiratis. This may reflect more calorically dense foods consumed as snacks, or longer time periods spent eating that has been categorized into one snacking episode. In addition, caloric beverages account for 8% to 14% of total calories, which are below that found for in the US, UK, and Mexico, among countries with national studies on these beverages (Barquera et al 2008, Popkin 2010a, Popkin 2010b). While these levels are relatively low for adult females, excessive sugar-sweetened beverages (soda and fruit drinks) and replacing whole milk with low-fat milk consumption among children and adolescents, represent targets for calorie reduction.
Currently, physical activity levels are low among Emiratis, especially among females and those living in urban areas. Only 41% of Emirati women undertake moderate or high levels of physical activity, compared with 82% of U.S. women (Kruger et al 2007) and 65% of Saudi women (Al-Hazzaa 2007). Past studies in the UAE have alluded to possible societal and institutional reasons that account for low physical activity levels among Emiratis of all ages (Carter et al 2003, Musaiger et al 2003a, Wasfi et al 2008), but particularly among females (Ali et al 2008, Berger and Peerson 2009, Kerkadi et al 2005, Musaiger et al 2003b, Wasfi et al 2008). Explanations for low engagement in physical activity include strong socio-cultural norms that create obstacles for sport involvement, a lack of role models, and for females, the additional limited access to sporting venues and appropriate attire (Berger and Peerson 2009). Females therefore tend to spend a large part of their time indoors, while socializing or television watching frequently involve eating and snacking on high fat or sugared foods (Kerkadi et al 2005). Even home activities like preparation of food and household chores are lacking as these are often done by maids or cooks (Al-Hourani et al 2003, Mabry et al 2009), the presence of which is significantly associated with BMI and obesity (Al-Isa and Moussa 1999, Al-Kandari 2006). These will have intergeneration effects as Emirati children are likely to emulate the lifestyle behaviors of family members. Certainly, other individual level factors such as motivation or personal preferences that interact with these socio-cultural and environmental factors are also important, but this was beyond the scope of this study, and is a research gap, particularly in the Arab Gulf context.
Environmental factor such as cities not designed for walking has made Emiratis heavily reliant on automobiles (Musaiger et al 2003b). Indeed, it appears that the more urbanized areas may be more obesogenic, based on our findings that women who relocated into cities in the past 5 years had the highest prevalence rates for overweight and obesity and were the least active. The arid hot climate, dusty conditions along with exposure to indoor and second-hand smoke are additional underlying factors linked with a high prevalence of asthma (Al Frayh et al 2001, Ibrahim et al 2006, Yeatts et al working paper), which discourage exercise or being outdoors.
With just a cross-sectional survey, it is not possible to reach conclusions about causality. Detailed analyses with efforts to track these measures longitudinally will allow for more definitive conclusions. Moreover, it is possible that women in the poorest households might appear to have lower levels of physical activity because the IPAQ only asks about leisure activities, not work-related activities which may be higher for this subpopulation. In addition, the dietary estimates are based on a snapshot of a 24-hour period and might therefore not be a good reflection of overall diet or usual intake, which might vary substantially daily or seasonally. Mis-reporting of consumption might have also occurred (particularly on snacks and possibly among the obese), but the use of the five-step multiple pass method should have minimized these potential biases.
Nonetheless, it is clear that a combination of various initiatives that make healthier diet choice and physical activity less difficult to achieve is needed. These include working to create a more positive built environment and provide social support for improved lifestyle choices by individuals. As the UAE continues to urbanize, health officials should also work with planners to ensure that communities have access to exercise facilities and design communities that promote active transport, are safe for exercise, and also cater to females within their cultural context. Access to a larger variety of healthier food options, limiting access to or increasing the costs of less healthy options may also help improve diets. These environmental changes along with targeted public nutrition education (e.g., limit the consumption of calorically dense sugared soda, fruit drinks and whole milk, while encourage consumption of water and low-fat/skim milk instead) and promotion of physical activity from a young age and especially among females can work well hand-in-hand. In addition, health practitioners should continue to measure and monitor the weight status of its population during any routine medical visit at all ages. This could allow physicians to prevent unnecessary weight gain and provide appropriate diet and activity recommendations, as well as direct patients to nutritionists, dieticians, or other specialists as needed.
ACKNOWLEDGEMENTS
This work is supported by the United Arab Emirates Environmental Agency – Abu Dhabi (EAD). The authors would like to thank the University of North Carolina’s Collaborative Studies Coordinating Center (CSCC), the interviewers, nurses, dietitians, data coders, and respondents in the UAE who were involved in the UNC-Indoor Air, Health and Nutrition Study. In addition, thanks to Phil Bardsley for programming assistance, Frances Dancy for administration help, and Tom Swasey for graphics assistance. All errors are the authors alone.
Footnotes
CONFLICTS OF INTEREST
The authors have no conflicts of interest.
REFERENCES
- Al-Amiri HA, Al-Otaibi JA, Al-Foudari MY, Heji AHB. The nutritive value of selected commonly consumed Kuwaiti dishes. Int J Food Sci Nutr. 2009;60:668–676. doi: 10.3109/09637480802002408. [DOI] [PubMed] [Google Scholar]
- Al-Hazzaa HM. Health-enhancing physical activity among Saudi adults using the International Physical Activity Questionnaire (IPAQ) Public Health Nutr. 2007;10:59–64. doi: 10.1017/S1368980007184299. [DOI] [PubMed] [Google Scholar]
- Al-Hourani HM, Henry CJ, Lightowler HJ. Prevalence of overweight among adolescent females in the United Arab Emirates. Am J Hum Biol. 2003;15:758–764. doi: 10.1002/ajhb.10212. [DOI] [PubMed] [Google Scholar]
- Al-Isa AN, Moussa MA. Factors associated with overweight and obesity among Kuwaiti kindergarten children aged 3-5 years. Nutr Health. 1999;13:125–139. doi: 10.1177/026010609901300301. [DOI] [PubMed] [Google Scholar]
- Al-Kandari YY. Prevalence of obesity in Kuwait and its relation to sociocultural variables. Obes Rev. 2006;7:147–154. doi: 10.1111/j.1467-789X.2006.00231.x. [DOI] [PubMed] [Google Scholar]
- Al Frayh AR, Shakoor Z, Gad El Rab MO, Hasnain SM. Increased prevalence of asthma in Saudi Arabia. Ann Allergy Asthma Immunol. 2001;86:292–296. doi: 10.1016/s1081-1206(10)63301-7. [DOI] [PubMed] [Google Scholar]
- Ali HI, Bernsen RM, Baynouna LM. Barriers to weight management among Emirati women: a qualitative investigation of health professionals’ perspectives. Int Q Comm Health Educ. 2008;29:143–159. doi: 10.2190/IQ.29.2.d. [DOI] [PubMed] [Google Scholar]
- Amine EK, Samy M. Obesity among female university students in the United Arab Emirates. J R Soc Health. 1996;116:91–96. doi: 10.1177/146642409611600206. [DOI] [PubMed] [Google Scholar]
- Barquera S, Hernández L, Tolentino ML, Espinosa J, Leroy J, Rivera J, et al. Energy from beverages is on the rise among Mexican adolescents and adults. J Nutr. 2008;138:2454–2461. doi: 10.3945/jn.108.092163. [DOI] [PubMed] [Google Scholar]
- Berger G, Peerson A. Giving young Emirati women a voice: participatory action research on physical activity. Health Place. 2009;15:117–124. doi: 10.1016/j.healthplace.2008.03.003. [DOI] [PubMed] [Google Scholar]
- Booth M. Assessment of physical activity: an international perspective. Res Q Exerc Sport. 2000;71:S114–120. [PubMed] [Google Scholar]
- Carter AO, Elzubeir M, Abdulrazzaq YM, Revel AD, Townsend A. Health and lifestyle needs assessment of medical students in the United Arab Emirates. Med Teach. 2003;25:492–496. doi: 10.1080/01421590310001605633. [DOI] [PubMed] [Google Scholar]
- Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. Br Med J. 2000;320:1240–1243. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craig CL, Marshall AL, Sjorstrom M. International physical activity questionnaire: 12-country reliability and validity. 2003 doi: 10.1249/01.MSS.0000078924.61453.FB. [DOI] [PubMed] [Google Scholar]
- Dashti B, Al-Awadi F, Khalafawi MS, Sawaya W, Al-Amiri H. Soluble and insoluble dietary fibre in thirty-two Kuwaiti dishes. Food Chemistry. 2003;83:557–561. [Google Scholar]
- Dashti B, Al-Awadi F, AlKandari R, Ali A, Al-Otaibi J. Macro- and microelements contents of 32 Kuwaiti composite dishes. Food Chemistry. 2004;85:331–337. [Google Scholar]
- Dashti BH, Al-Awadi F, Khalafawi MS, Al-Zenki S, Sawaya W. Nutrient contents of some traditional Kuwaiti dishes: proximate composition, and phytate content. Food Chemistry. 2001;74:169–175. [Google Scholar]
- Dietz WH. The role of lifestyle in health: the epidemiology and consequences of inactivity. Proc Nutr Soc. 1996;55:829–840. doi: 10.1079/pns19960082. [DOI] [PubMed] [Google Scholar]
- ESHA Research . In: Food Processor and Genesis SQL Database sources. ESHA Research, editor. Salem; OR: 2006. [Google Scholar]
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303:235–241. doi: 10.1001/jama.2009.2014. [DOI] [PubMed] [Google Scholar]
- Hagströmer M, Oja P, Sjöström M. The International Physical Activity Questionnaire (IPAQ): a study of concurrent and construct validity. Public Health Nutr. 2006;9:755–762. doi: 10.1079/phn2005898. [DOI] [PubMed] [Google Scholar]
- Hallal PC, Victora CG. Reliability and Validity of the International Physical Activity Questionnaire (IPAQ) Med Sci Sports Exerc. 2004;36:556. doi: 10.1249/01.mss.0000117161.66394.07. [DOI] [PubMed] [Google Scholar]
- Ibrahim AJ, Abdulbari B, Andrew B. Prevalence of Asthma among Qatari Schoolchildren: International Study of Asthma and Allergies in Childhood, Qatar. Pediatr Pulmonology. 2006;41:80–86. doi: 10.1002/ppul.20331. [DOI] [PubMed] [Google Scholar]
- Institute of Medicine . In: Dietary Reference Intakes for Energy, Carbohydrates, Fiber, Fat, Protein and Amino Acids (Macronutrients) IOM, editor. IOM; Washington DC: 2002. [Google Scholar]
- International Monetary Fund . World Economic Outlook Database, April 2009: Nominal GDP list of countries. 2009. Data for the year 2008. [Google Scholar]
- IPAQ Research Committee . Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ) 2005. [Google Scholar]
- Kerkadi A. Evaluation of nutritional status of United Arab Emirates University female students. Emir J Agric Sci. 2003;15:42–50. [Google Scholar]
- Kerkadi A, Abo-Elnaga N, Ibrahim W. Prevalence of overweight and associated risk factors among primary female school children in Al-Ain City, UAE. Emir J Agric Sci. 2005;17:43–56. [Google Scholar]
- Kruger J, Kohl HW, Miles IJ. Prevalence of regular physical activity among adults - United States, 2001 and 2005. MMWR. 2007;56:1209–1212. [PubMed] [Google Scholar]
- Kuwait Institute for Scientific Research . In: Food Composition Tables for Kuwait Composite Dishes, 1998. Kuwait Institute for Scientific Research, editor. Kuwait Institute for Scientific Research; Kuwait: 1998. [Google Scholar]
- Kuwait Institute for Scientific Research . Kuwait Food Instruction Booklet. KISR; Kuwait City: 2010. [Google Scholar]
- Mabry RM, Reeves MM, Eakin EG, Owen N. Evidence of physical activity participation among men and women in the countries of the Gulf Cooperation Council: a review. Obes Rev. 2010;11:457–464. doi: 10.1111/j.1467-789X.2009.00655.x. [DOI] [PubMed] [Google Scholar]
- Malik M, Bakir A. Prevalence of overweight and obesity among children in the United Arab Emirates. Obes Rev. 2007;8:15–20. doi: 10.1111/j.1467-789X.2006.00290.x. [DOI] [PubMed] [Google Scholar]
- Moshfegh AJ, Rhodes DG, Baer DJ, Murayi T, Clemens JC, Rumpler WV, et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008;88:324–332. doi: 10.1093/ajcn/88.2.324. [DOI] [PubMed] [Google Scholar]
- Musaiger AO, Radwan HM. Social and dietary factors associated with obesity in university female students in United Arab Emirates. J R Soc Health. 1995;115:96–99. doi: 10.1177/146642409511500207. [DOI] [PubMed] [Google Scholar]
- Musaiger AO, Abuirmeileh NM. Food consumption patterns of adults in the United Arab Emirates. J R Soc Health. 1998;118:146–150. doi: 10.1177/146642409811800304. [DOI] [PubMed] [Google Scholar]
- Musaiger AO, Arab Taskforce for O, Physical Activity. Kingdom of B Recommendations of the First Conference on Obesity and Physical Activity in the Arab countries. Held in Bahrain, 24-26 September, 2002. Nutr Health. 2003a;17:117–121. doi: 10.1177/026010600301700202. [DOI] [PubMed] [Google Scholar]
- Musaiger AO, Lloyd OL, Al-Neyadi SM, Bener AB. Lifestyle factors associated with obesity among male university students in the United Arab Emirates. Nutr Food Sci. 2003b;33:145–147. [Google Scholar]
- Ng SW, Zaghloul S, Ali HI, Harrison G, Popkin BM. The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States. Obes Rev. 2011;12:1–13. doi: 10.1111/j.1467-789X.2010.00750.x. [DOI] [PubMed] [Google Scholar]
- Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA. 2010;303:242–249. doi: 10.1001/jama.2009.2012. [DOI] [PubMed] [Google Scholar]
- Piernas C, Popkin BM. Trends in snacking among U.S. children. Health Affairs. 2010a;29:398–404. doi: 10.1377/hlthaff.2009.0666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piernas C, Popkin BM. Snacking increased among U.S. adults between 1977 and 2006. J Nutr. 2010b;140:325–332. doi: 10.3945/jn.109.112763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Popkin BM. Patterns of beverage use across the lifecycle. Physiol Behav. 2010a;100:4–9. doi: 10.1016/j.physbeh.2009.12.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Popkin BM, Ng S, Mhurchu CN, Jebb S. Beverage patterns and trends in the United Kingdom. University of North Carolina; Chapel Hill: 2010b. [Google Scholar]
- Qahoush R, Stotts N, Alawneh MS, Froelicher ES. Physical activity in Arab women in Southern California. Eur J Cardiovascular Nursing. 2010;9:263–271. doi: 10.1016/j.ejcnurse.2010.03.002. [DOI] [PubMed] [Google Scholar]
- Rabbia A, El-Moneim HQ, Al-Majeed TQ, Alami H. Assessing health risk behaviours among secondary school students in Abu Dhabi. UAE; Abu Dhabi: 2004. [Google Scholar]
- Raper N, Perloff B, Ingwersen L, Steinfeldt L, Anand J. An overview of USDA’s Dietary Intake Data System. J Food Composition Analysis. 2004;17:545–555. [Google Scholar]
- Sheikh-Ismail LI, Henry CJ, Lightowler HJ, Aldhaheri AS, Masuadi E, Al Hourani HM. Prevalence of overweight and obesity among adult females in the United Arab Emirates. Int J Food Sci Nutr. 2008:1–8. doi: 10.1080/09637480802331179. [DOI] [PubMed] [Google Scholar]
- StataCorp . Stata Statistical Software: Release 11. StataCorp LP.; College Station, TX: 2009. [Google Scholar]
- UAE-GSHS. United Arab Emirates Global School-based Student Health Survey . In: Al-Matroushi MA, Fikry M, editors. 2005. [Google Scholar]
- UAEHALS . In: Measuring the Health of the Nation: United Arab Emirates Health and Lifestyle Survery. Badrinath P, Al-Shboul QA, Zoubeidi T, Gargoun AS, Ghubash R, El-Rufaie OE, editors. Al-Ain, UAE; United Arab Emirates University: 2000. [Google Scholar]
- Vyas S, Kumaranayake L. Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plan. 2006;21:459–468. doi: 10.1093/heapol/czl029. [DOI] [PubMed] [Google Scholar]
- Wasfi AS, El-Sherbiny AA, Gurashi E, Al Sayegh FU. Sport practice among private secondary-school students in Dubai in 2004. East Mediterr Health J. 2008;14:704–714. [PubMed] [Google Scholar]
- WHO . In: World Health Survey. WHO, editor. Geneva: [Google Scholar]
- WHO . Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation. World Health Organization; Geneva: 2000. [PubMed] [Google Scholar]
- Yeatts K, Sadig M, Olshan A, Leith D, Funk W, Masakiri F. evaluation of potential association of indoor air quality with asthma, respiratory symptoms, allergic rhinitis, and eczema: UAE-IAHN. University of North Carolina; Chapel Hill, NC: working paper. [Google Scholar]
- Zaghloul S, Waslien A, Al Somaie M, Parakash P. Low adherence of Kuwaiti adults to fruit and vegetable guidelines. East Mediterr Health J. doi: 10.26719/2012.18.5.461. In press. [DOI] [PubMed] [Google Scholar]