

Abstract
Given the importance of physical activity (PA) for weight control, identifying strategies to achieve higher PA levels is imperative. We hypothesized that performing a greater variety of self-reported moderate-to-vigorous activities (MVPAs) would relate to higher objectively measured MVPA minutes in two groups who were successfully maintaining their body weight: weight loss maintainers (WLM/n = 226) and normal-weight individuals (NW/n = 169). The Paffenbarger Questionnaire and RT3 accelerometer were used to determine variety/number of different MVPAs performed and MVPA minutes, respectively. The variety/number of different activities performed by WLM and NW was similar (1.8 ± 1.2 versus 1.7 ± 1.2, P = 0.52). Regression analyses showed that greater variety (P < 0.01) and WLM status (P < 0.05) were each positively related to greater MVPA minutes/day and meeting the ≥250 MVPA minutes/week guideline for long-term weight maintenance. The association between greater variety and higher MVPA was similar in NW and WLM. Future studies should test whether variety can facilitate engagement in higher MVPA levels for more effective weight control.
1. Introduction
Engaging in high levels of physical activity is a key strategy for successful maintenance of weight loss [1]. A study of nearly 4,000 participants in the National Weight Control Registry (NWCR), the largest longitudinal study of successful weight loss maintainers, indicated participants expend 2,621 ± 2,252 kcal per week through physical activity, which is equivalent to approximately 60 minutes of moderate-intensity physical activity per day [2]. Additionally, long-term followup of participants in behavioral weight loss programs has shown that those who are most successful at maintaining their weight loss report activity levels similar to those of NWCR participants [3, 4].
Many individuals, particularly those who are obese, are insufficiently active, and increasing physical activity can be a challenge [5, 6]. Thus, strategies that assist individuals in adopting and sustaining high levels of physical activity to help facilitate a healthy body weight are needed. Prior studies have identified multiple strategies for increasing physical activity adoption and maintenance, such as providing home or clinic-based exercise programs [7], increasing access to active behaviors (e.g., adding exercise equipment in the home) [8], and reducing access to sedentary behaviors (e.g., limiting time to watch television) [9], using pedometers to track activity and progress toward physical activity goals [10], and accumulating exercise throughout the day in multiple short bouts (≥10 min) [11, 12].
Performing a variety of different types of activities may be another strategy to increase physical activity levels [13]. The National Health and Nutrition Examination Survey (NHANES) showed that individuals who reported engaging in a variety of different activities (i.e., walking + other leisure-time activities) were more likely to meet national physical activity recommendations compared to those who reported no variety (i.e., only walking) [14]. Likewise, in an 18-month behavioral weight loss intervention, overweight participants who reported physical activity variety (i.e., ≥2 different activities) at 6 months had higher self-reported activity-related energy expenditure and a lower body mass index (BMI) at 18 months than those who did not report physical activity variety (i.e., only 1 activity) [15]. Thus, while the above findings suggest that physical activity variety may contribute to higher physical activity levels within the context of behavioral weight loss treatment, it is unclear whether physical activity variety is associated with higher physical activity in individuals who have achieved long-term success in controlling their body weight.
In the current study, we examined the relationship between physical activity variety, defined as the number of different types of self-reported moderate-to-vigorous activities performed in one week, and minutes spent in objectively measured moderate-to-vigorous physical activity (MVPA) in two groups of individuals who have successfully maintained their body weight long-term: (1) weight loss maintainers with previous history of overweight/obesity and (2) normal-weight individuals without a history of overweight. Normal-weight participants were included as a comparison group given that weight loss maintainers represent a unique group of individuals who report strict adherence to multiple behavioral strategies in order to maintain their body weight [16]. Due to their unique characteristics and history, it is possible that the association between physical activity variety and MVPA could be different for weight loss maintainers and normal-weight individuals. However, based on previous research showing a relationship between physical activity variety and higher physical activity levels across diverse groups and settings [14, 15], we predicted that engagement in a greater variety of moderate-to-vigorous activities would be associated with higher MVPA daily minutes in both the weight loss maintainer and normal-weight groups.
2. Methods
2.1. Subjects and Procedures
Participants were enrollees in the cross-sectional “LITE” study that compared weight control behaviors of weight loss maintainers and normal-weight controls. Study methods and sample characteristics have been reported previously [17]. A convenience sample of men and women was recruited through advertisements placed in national and local publications intended for a general audience. Persons interested in participating were asked to either call a toll-free number or to visit a website. Participants were recruited from across the United States, although most were from New England, California, and the Washington, DC area.
Individuals were screened by phone to determine study eligibility. Weight loss maintainers had a history of overweight or obesity (BMI ≥25) but were currently normal weight (BMI = 18.5–24.9), having maintained a ≥10% loss of their lifetime maximum body weight for at least 5 years. Normal-weight participants had a current BMI between 18.5 and 24.9 and no history of overweight or obesity. Participants in both groups were weight stable (±10 lb) for at least 2 years prior to enrollment. Of 813 individuals who responded to advertisements and a brief online screening tool, 528 were deemed eligible. Of these, 480 signed consent forms and participated in the study assessments. Participants were given $50 upon completion of all study assessments. The study protocol was approved by The Miriam Hospital Institutional Review Board, Providence, RI, USA.
2.2. Measures
2.2.1. Demographics and Weight
Participants reported information about age, gender, marital status, ethnicity/race, type of employment, and education. Weight and weight history were assessed via self-report methods that have been previously validated [18].
2.2.2. Physical Activity Variety
Questions on the Paffenbarger Physical Activity Questionnaire [19] regarding average number of city blocks walked per day, and weekly frequency and duration of sports and recreational activities performed were used to determine variety or number of different activities performed during the past 7 days [15]. Only activities that were performed at a moderate or vigorous intensity and for ≥10 minutes in duration were included given that engagement in these activities is considered necessary for improving health and achieving a healthy body weight [1, 12]. The intensity of sports and recreational activities was determined using the Paffenbarger coding scheme. For walking to be counted as an activity, participants had to report walking the equivalent of at least 12 blocks per day (i.e., 1 mile at a moderate intensity). Treadmill walking reported as a sports and recreational activity was not distinguished as a separate activity from walking ≥12 blocks/day. Climbing stair flights, walking <12 blocks/day, and sports and recreational activities that were performed for <10 minutes were not considered to contribute to variety.
2.2.3. Objectively Measured MVPA
The RT3 research activity monitor (Stayhealthy, Inc., Monrovia, CA, USA) was used to objectively measure daily minutes spent in MVPA. This device converts accelerations or movements from vertical, horizontal, and anterior-posterior planes into counts, with greater magnitude or intensity of acceleration over a given time period generating a higher number of counts. Participants were sent the device in a postage-paid envelope with instructions on how to activate the device and wear it on their waistband during all waking hours for 7 consecutive days, except while bathing or swimming. Each device was programmed with the participant's personal data (sex, age, height, and weight) and set to capture movements continuously in 1-minute intervals. The RT3 has shown to be a strong predictor of oxygen consumption during sedentary and treadmill activities [20, 21] and a more precise measure of physical activity at the group level compared to its Tri-Trac predecessor [22].
Consistent with previously documented methods for analyzing RT3 data, a minimum of 4 days on which the device was worn for ≥10 hours each day was required for data to be considered valid [23, 24]. RT3 nonwear times, defined as periods of ≥30 consecutive minutes of zero counts (permitting intervals of up to 2 consecutive minutes registering 1–100 counts/min), were deleted from analysis. The remaining time was partitioned according to intensity level. Based on previous RT3 validation research [21] and a recent study that used the RT3 to compare MVPA patterns in weight loss maintainers, normal-weight, and obese groups [25], we computed time spent in MVPA using a threshold of ≥984 counts/min.
2.3. Statistics
Descriptive statistics are presented in tables as means ± SD for continuous measures and percentages for categorical responses. Chi-square analyses were used to compare proportions across categories. Independent t-tests were conducted to assess differences between the groups on demographic characteristics, weight, accelerometer daily wear time, MVPA minutes/day, and reported variety/number of different types of moderate-to-vigorous activities performed. Linear regression was used to examine the associations of physical activity variety and group status (weight loss maintainers versus normal weight) with objectively measured MVPA minutes/day, adjusting for age, gender, years of education, marital status, BMI, and accelerometer daily wear time. Logistic regression was used to assess whether physical activity variety and group status were associated with achieving the ≥250 MVPA minutes/week recommendation for optimal long-term weight maintenance [1]. For this analysis, MVPA minutes/week was calculated by multiplying average daily MVPA minutes by 7 (days).
3. Results
Of 413 participants who were sent an accelerometer and the PPAQ, 394 (95%) met valid accelerometer wear requirements and provided complete data on the PPAQ. The characteristics of these 226 weight loss maintainers and 169 normal-weight participants are presented in Table 1. Both groups were similar in age (48.8 ± 12.9 years), gender (84% female), marital status (66% married), race/ethnicity (94% Caucasian), employment status (82% employed), and job type (95% in professional or clerical positions). A greater proportion of normal-weight participants was college educated, compared to the weight loss maintainers. Both groups were normal weight, although the weight loss maintainers had a slightly higher BMI. On average, weight loss maintainers had lost nearly 29 kg and maintained ≥10% weight loss for 13.7 ± 9.6 years. There were no differences in accelerometer wear time between the groups, with the weight loss maintainers and normal-weight participants wearing the accelerometer for an average of 14.8 ± 2.0 hours/day on 7.5 ± 0.9 days. As reported previously, weight loss maintainers spent an average of 6 minutes more per day in MVPA, compared to normal-weight participants (58 versus 52 min/d) [17]. The variety/number of different activities performed by the weight loss maintainers and normal-weight participants was similar (1.8 ± 1.2 versus 1.7 ± 1.2, P = 0.52). Additionally, when participants who reported no moderate-to-vigorous activities were excluded, the variety/number of activities performed by WLM (n = 180) and NW (n = 141) remained similar (2.2 ± 1.0 versus 2.0 ± 1.0, P = 0.10).
Table 1.
Characteristics of weight loss maintainer (WLM) and always normal-weight (NW) participants.
| WLM (N = 226) |
NW (N = 169) |
P* | |
|---|---|---|---|
| Age (yrs) | 48.8 ± 12.4 | 47.0 ± 13.5 | 0.17 |
| % Female | 82.3 | 86.4 | 0.33 |
| % White Non-Hispanic | 95.1 | 92.9 | 0.39 |
| % Married | 69.9 | 60.9 | 0.07 |
| % ≥4-year college degree | 78.3 | 87.0 | 0.03 |
| % Employed | 79.6 | 81.7 | 0.70 |
| % Professional or clerical job | 95.0 | 95.6 | 0.99 |
| Current BMI (kg/m2) | 22.1 ± 1.7 | 21.3 ± 1.5 | <0.001 |
| Lifetime maximum weight (kg) | 91.1 ± 17.7 | 62.6 ± 18.1 | <0.001 |
| Duration of weight loss maintenance (yrs) | 13.7 ± 9.6 | — | — |
| Valid (≥10 h wear time) accelerometer days | 7.5 ± 0.8 | 7.5 ± 0.9 | 0.48 |
| Daily accelerometer wear time (h/day) | 15.0 ± 2.2 | 14.6 ± 1.8 | 0.06 |
| MVPA min/d | 58.3 ± 37.7 | 51.6 ± 27.3 | 0.04 |
| PA variety (number of different activities performed) | 1.8 ± 1.3 | 1.7 ± 1.2 | 0.52 |
*P values are based on independent t-tests for continuous variables and Chi-square tests for categorical variables.
3.1. Associations of Physical Activity Variety and Group Status with Objectively Measured MVPA
We next examined the independent and joint associations of physical activity variety and group status with MVPA minutes per day. Given that the physical activity variety × group status interaction was not significant (P = 0.73), the results of the main effects linear regression model for MVPA minutes per day are shown (Table 2). Greater physical activity variety (P < 0.001) and weight loss maintainer status (P < 0.05) were independently related to greater daily time spent in MVPA, after adjustment for demographic characteristics (age, gender, educational level, marital status, current BMI) and daily accelerometer wear time. Figure 1 presents estimated MVPA minutes per day in the weight loss maintainer and normal-weight groups by reported number of different moderate-to-vigorous activities performed. Across both groups combined, the number of moderate-to-vigorous activities ranged from 0 to ≥4, with 73 participants (18.5%) reporting 0 activities, 105 reporting 1 activity (26.6%), 112 (28.4%) reporting 2 activities, 74 reporting 3 activities (18.7%), and 30 (15.4%) reporting 4 or more activities. Each 1 unit increase in the number of different moderate-to-vigorous activities performed was associated with an additional 9.4 ± 1.3 daily minutes spent in MVPA, representing an additional 56.2 ± 8.3 kcal expended per day based on RT3-derived estimates.
Table 2.
Associations of physical activity variety and group status with moderate-to-vigorous physical activity (MVPA) minutes per day.
| Variable | Standardized β | t | P |
|---|---|---|---|
| MVPA variety | 0.38 | 6.11 | <0.001 |
| Group status (weight loss maintainers) | 0.11 | 2.28 | 0.02 |
| Age | −0.17 | −3.38 | 0.01 |
| Gender (male) | 0.04 | 0.87 | 0.39 |
| Education (≥4-year college degree) | 0.05 | 1.03 | 0.30 |
| Marital status (nonmarried) | −0.003 | −0.07 | 0.94 |
| Current BMI (kg/m2) | −0.07 | −1.12 | 0.27 |
| Daily accelerometer wear time | 0.05 | 1.16 | 0.25 |
| Model R2 = 0.20, F (8, 393) = 12.1, P < 0.001 |
MVPA variety: number of different types of activities performed; group status: weight loss maintainers versus normal-weight individuals.
Figure 1.
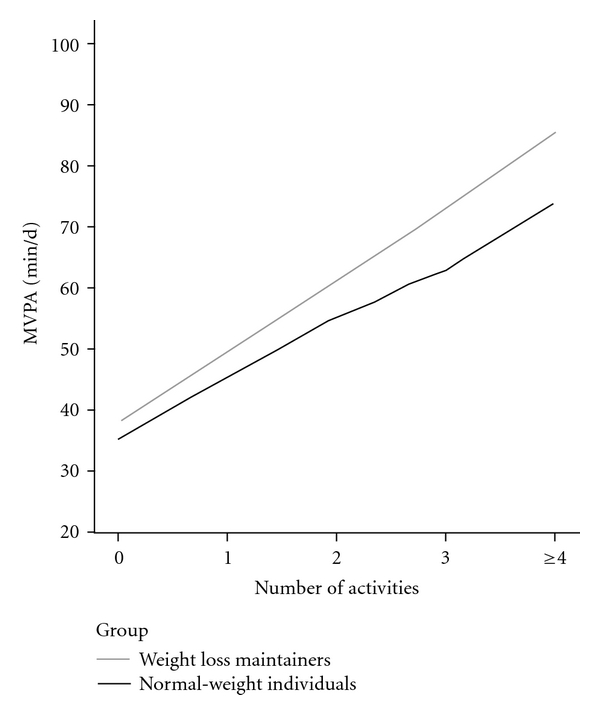
Estimated moderate-to-vigorous physical activity (MVPA) minutes in Weight Loss Maintainers and Normal-weight groups by reported variety or number of different activities performed. Estimated mean MVPA minutes/day adjusted for age, gender, education level, marital status, current BMI, and daily accelerometer wear time.
Similarly, logistic regression analyses showed that greater physical activity variety (OR = 1.78 [1.37–2.30], P < 0.001), weight loss maintainer status (OR = 0.23 [0.08–0.69], P = 0.002), and lower BMI (OR = 0.81 [0.69–0.95], P = 0.01) were independently associated with meeting the ≥250 MVPA minutes/week guideline for optimal weight maintenance [1]. The physical activityvariety × group status interaction was not significant (P = 0.25).
4. Discussion
Given the continuing obesity epidemic and growing evidence that indicates greater amounts of physical activity are needed for successful long-term weight control [1], it is important to identify strategies that can assist individuals in adopting and maintaining high levels of physical activity. This study examined whether performing a greater variety of different types of moderate-to-vigorous physical activities was related to greater time spent in MVPA among weight loss maintainers and normal-weight individuals without a history of overweight/obesity. We found that, independent of group, greater variety was associated with higher daily MVPA minutes and meeting the 250 MVPA minutes per week recommendation for optimal long-term weight maintenance [1]. These findings are consistent with previous studies of the general population [14] and in overweight/obese individuals undergoing behavioral weight loss treatment [15].
However, the present study is the first to show a relationship between greater physical activity variety and higher objectively measured MVPA duration and energy expenditure in two groups of individuals who have had long-term success in maintaining a normal body weight. We found that for each additional different type of moderate-to-vigorous activity performed, participants on average spent an additional 9 minutes in MVPA and expended 56 more kcal per day. Thus, for example, participants who reported engaging in 3 different activities during the previous week spent on average an additional 18 minutes in MVPA and expended 112 more calories per day compared to participants who reported engaging in only 1 activity. While our findings do not imply causation, they do warrant additional longitudinal research to examine whether incorporating variety into a physical activity routine may be an efficacious strategy to achieve higher MVPA levels for enhanced weight control.
The relationship between greater physical activity variety and engagement in higher MVPA levels may be potentially explained by a number of physiological and psychological factors. For example, alternating different physical activities that involve different muscle groups and energy systems (aerobic, anaerobic) might promote greater exercise consistency by affording more time for recovery and decreasing risk of overuse injuries [13, 26]. Participating in a variety of activities may also facilitate greater exercise adherence via increased enjoyment [27] and decreased boredom [13, 26]. Greater access to a variety of activities may increase the likelihood that individuals will find an exercise activity or a combination of exercise activities that they like and will perform regularly [27]. Additionally, research based on the behavioral economics model suggests that motivation to exercise is enhanced when individuals can choose from a variety of physical activities versus only one physical activity [28, 29]. Consequently, adding a variety component to a physical activity prescription may aid individuals in achieving and maintaining high levels of physical activity. Future research is needed to investigate potential mechanisms that underlie the relationship between variety and higher MVPA levels.
Whereas increased variety of healthy physical activities is associated with greater time spent in MVPA, it is also possible that decreased variety of unhealthy sedentary activities might contribute to lesser time spent being sedentary and higher overall physical activity levels. Given that sedentary behaviors, independent of physical activity, have shown to be detrimentally associated with BMI and other cardiometabolic risk factors [30, 31], future studies that examine the association between variety and sedentary behaviors are needed.
Our findings should be interpreted within the context of certain limitations. The cross-sectional nature of our study does not allow us to determine whether greater variety contributes to higher MVPA levels or alternatively whether individuals with higher MVPA levels naturally incorporate more variety into their physical activity routine. As variety in physical activity is rarely measured, the importance of factors such as the time frame for assessing variety (i.e., a week, month, year) and frequency of occurrence of different activities within the time frame (i.e., once a week, twice a month) are not known. While the use of an objective measure of physical activity is a strength of this investigation, it is important to note that hip-worn accelerometers like the RT3 used in this study may be limited in their ability to accurately estimate the intensity of activities not performed on flat surfaces [20]. Thus, it is possible that MVPA was underestimated in individuals who more frequently engaged in activities that involved an incline or greater upper body movement. Additionally, the accelerometer count threshold we used to identify MVPA was determined in a leaner, younger male sample [21] and thus may have affected validity in our older, largely female sample. Given the homogeneity of our sample with respect to gender (female) and race (White Non-Hispanic), our results may not be generalizable to men or other ethnic populations. Similarly, participants in this study were all normal weight and had high physical activity levels on average. Thus, future investigations should examine the potential importance of variety for increasing physical activity in overweight and inactive populations. Finally, it is important to note that just as altering the variety of different types of activities performed could potentially increase MVPA duration and energy expenditure, so could altering the frequency, intensity, and duration of a single activity, independent of changes in physical activity variety.
In summary, this study examined the relationship between physical activity variety and objectively measured MVPA levels in weight loss maintainers and normal-weight individuals who both had long-term success in maintaining their body weight. In both groups, physical activity variety was related to greater engagement in MVPA and likelihood of accumulating ≥250 MVPA minutes/week, consistent with physical activity guidelines for optimal long-term weight maintenance [1]. Future studies are needed to test whether incorporating variety or different types of activities (e.g., walking and cycling) can facilitate engagement in higher levels of MVPA within interventions aimed at promoting and maintaining physical activity.
Conflict of Interests
All authors have no conflict of interests.
Authors' Contribution
D. S. Bond, H. A. Raynor, S. Phelan, J. Steeves, and R. Wing contributed to conception and design of the study. R. Wing and S. Phelan obtained the research funding and supervised study implementation and data collection. D. S. Bond and R. Daniello performed statistical analyses. D. S. Bond wrote the initial draft of the paper, and all authors contributed to interpretation of the data and the writing of the paper. All authors read and approved the final paper.
Acknowledgments
Appreciation is expressed to Dustin Jordan for assisting with data collection. This research was supported by the National Institutes of Health Grant DK066787. Dr. Bond is supported by the National Institutes of Health Grant DK083438.
References
- 1.Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Medicine and Science in Sports and Exercise. 2009;41(2):459–471. doi: 10.1249/MSS.0b013e3181949333. [DOI] [PubMed] [Google Scholar]
- 2.Catenacci VA, Ogden LG, Stuht J, et al. Physical activity patterns in the national weight control registry. Obesity. 2008;16(1):153–161. doi: 10.1038/oby.2007.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jakicic JM, Marcus BH, Lang W, Janney C. Effect of exercise on 24-month weight loss maintenance in overweight women. Archives of Internal Medicine. 2008;168(14):1550–1559. doi: 10.1001/archinte.168.14.1550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tate DF, Jeffery RW, Sherwood NE, Wing RR. Long-term weight losses associated with prescription of higher physical activity goals. Are higher levels of physical activity protective against weight regain? The American Journal of Clinical Nutrition. 2007;85(4):954–959. doi: 10.1093/ajcn/85.4.954. [DOI] [PubMed] [Google Scholar]
- 5.Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, Mcdowell M. Physical activity in the United States measured by accelerometer. Medicine and Science in Sports and Exercise. 2008;40(1):181–188. doi: 10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- 6.Tudor-Locke C, Brashear MM, Johnson WD, Katzmarzyk PT. Accelerometer profiles of physical activity and inactivity in normal weight, overweight, and obese U.S. men and women. International Journal of Behavioral Nutrition and Physical Activity. 2010;7, article 60 doi: 10.1186/1479-5868-7-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Perri MG, Martin AD, Leermakers EA, Sears SF, Notelovitz M. Effects of group- versus home-based exercise in the treatment of obesity. Journal of Consulting and Clinical Psychology. 1997;65(2):278–285. doi: 10.1037//0022-006x.65.2.278. [DOI] [PubMed] [Google Scholar]
- 8.Jakicic JM, Winters C, Lang W, Wing RR. Effects of intermittent exercise and use of home exercise equipment on adherence, weight loss, and fitness in overweight women a randomized trial. Journal of the American Medical Association. 1999;282(16):1554–1560. doi: 10.1001/jama.282.16.1554. [DOI] [PubMed] [Google Scholar]
- 9.Otten JJ, Jones KE, Littenberg B, Harvey-Berino J. Effects of television viewing reduction on energy intake and expenditure in overweight and obese adults: a randomized controlled trial. Archives of Internal Medicine. 2009;169(22):2109–2115. doi: 10.1001/archinternmed.2009.430. [DOI] [PubMed] [Google Scholar]
- 10.Bravata DM, Smith-Spangler C, Sundaram V, et al. Using pedometers to increase physical activity and improve health: a systematic review. Journal of the American Medical Association. 2007;298(19):2296–2304. doi: 10.1001/jama.298.19.2296. [DOI] [PubMed] [Google Scholar]
- 11.Jakicic JM, Wing RR, Butler BA, Robertson RJ. Prescribing exercise in multiple short bouts versus one continuous bout: effects on adherence, cardiorespiratory fitness, and weight loss in overweight women. International Journal of Obesity. 1995;19(12):893–901. [PubMed] [Google Scholar]
- 12.Haskell WL, Lee IM, Pate RR, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Medicine and Science in Sports and Exercise. 2007;39(8):1423–1434. doi: 10.1249/mss.0b013e3180616b27. [DOI] [PubMed] [Google Scholar]
- 13.Sherwood NE, Jeffery RW. The behavioral determinants of exercise: implications for physical activity interventions. Annual Review of Nutrition. 2000;20:21–44. doi: 10.1146/annurev.nutr.20.1.21. [DOI] [PubMed] [Google Scholar]
- 14.Fitzhugh EC, Thompson DL. Leisure-time Walking and compliance with ACSM/AHA aerobic-related physical activity recommendations: 1999–2004 NHANES. Journal of Physical Activity and Health. 2009;6(4):393–402. doi: 10.1123/jpah.6.4.393. [DOI] [PubMed] [Google Scholar]
- 15.Steeves J, Thompson D, Raynor H. Does engaging in a variety of physical activities improve maintenance of physical activity and body mass index reduction during an adult behavioral obesity intervention? Obesity. 2010;18(supplement 2):p. S94. [Google Scholar]
- 16.Thomas JG, Bond DS, Hill JO, Wing RR. The national weight control registry: a study of ‘successful losers’. ACSM's Health and Fitness Journal. 2011;15(2):8–12. [Google Scholar]
- 17.Phelan S, Roberts M, Lang W, Wing RR. Empirical evaluation of physical activity recommendations for weight control in women. Medicine and Science in Sports and Exercise. 2007;39(10):1832–1836. doi: 10.1249/mss.ob013e31812383c3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.McGuire MT, Wing RR, Klem ML, Lang W, Hill JO. What predicts weight regain in a group of successful weight losers? Journal of Consulting and Clinical Psychology. 1999;67(2):177–185. doi: 10.1037//0022-006x.67.2.177. [DOI] [PubMed] [Google Scholar]
- 19.Paffenbarger RS, Wing AL, Hyde RT. Physical activity as an index of heart attack risk in college alumni. The American Journal of Epidemiology. 1978;108(3):161–175. doi: 10.1093/oxfordjournals.aje.a112608. [DOI] [PubMed] [Google Scholar]
- 20.Howe CA, Staudenmayer JW, Freedson PS. Accelerometer prediction of energy expenditure: vector magnitude versus vertical axis. Medicine and Science in Sports and Exercise. 2009;41(12):2199–2206. doi: 10.1249/MSS.0b013e3181aa3a0e. [DOI] [PubMed] [Google Scholar]
- 21.Rowlands AV, Thomas PWM, Eston RG, Topping R. Validation of the RT3 triaxial accelerometer for the assessment of physical activity. Medicine and Science in Sports and Exercise. 2004;36(3):518–524. doi: 10.1249/01.mss.0000117158.14542.e7. [DOI] [PubMed] [Google Scholar]
- 22.Jacobi D, Perrin AE, Grosman N, et al. Physical activity-related energy expenditure with the RT3 and TriTrac accelerometers in overweight adults. Obesity. 2007;15(4):950–956. doi: 10.1038/oby.2007.605. [DOI] [PubMed] [Google Scholar]
- 23.Chen C, Jerome GJ, LaFerriere D, Young DR, Vollmer WM. Procedures used to standardize data collected by RT3 triaxial accelerometers in a large-scale weight-loss trial. Journal of Physical Activity and Health. 2009;6(3):354–359. doi: 10.1123/jpah.6.3.354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jakicic JM, Gregg E, Knowler W, et al. Activity patterns of obese adults with type 2 diabetes in the look AHEAD study. Medicine and Science in Sports and Exercise. 2010;42(11):1995–2005. doi: 10.1249/MSS.0b013e3181e054f0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Catenacci VA, Grunwald GK, Ingebrigtsen JP, et al. Physical activity patterns using accelerometry in the National Weight Control Registry. Obesity. 2010;19:1163–1170. doi: 10.1038/oby.2010.264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Knapik JJ, Rieger W, Palkoska F, Van Camp S, Darakjy S. United States Army physical readiness training: rationale and evaluation of the physical training doctrine. Journal of Strength and Conditioning Research. 2009;23(4):1353–1362. doi: 10.1519/JSC.0b013e318194df72. [DOI] [PubMed] [Google Scholar]
- 27.Glaros NM, Janelle CM. Varying the mode of cardiovascular exercise to increase adherence. Journal of Sport Behavior. 2001;24:42–62. [Google Scholar]
- 28.Epstein LH, Roemmich JN. Reducing sedentary behavior: role in modifying physical activity. Exercise and Sport Sciences Reviews. 2001;29(3):103–108. doi: 10.1097/00003677-200107000-00003. [DOI] [PubMed] [Google Scholar]
- 29.Vara LS, Epstein LH. Laboratory assessment of choice between exercise or sedentary behaviors. Research Quarterly for Exercise and Sport. 1993;64(3):356–360. doi: 10.1080/02701367.1993.10608822. [DOI] [PubMed] [Google Scholar]
- 30.Healy GN, Wijndaele K, Dunstan DW, et al. Objectively measured sedentary time, physical activity, and metabolic risk the Australian Diabetes, Obesity and Lifestyle Study (AusDiab) Diabetes Care. 2008;31(2):369–371. doi: 10.2337/dc07-1795. [DOI] [PubMed] [Google Scholar]
- 31.Bankoski A, Harris TB, McClain JJ, et al. Sedentary activity associated with metabolic syndrome independent of physical activity. Diabetes Care. 2011;34(2):497–503. doi: 10.2337/dc10-0987. [DOI] [PMC free article] [PubMed] [Google Scholar]