

Abstract
Chronic triceps insufficiency, causing prolonged disability, occurs due to a missed diagnosis of an acute rupture. We report a 25 year old male with history of a significant fall sustaining multiple injuries. Since then, he had inability in extending his right elbow for which he sought intervention after a year. Diagnosis of triceps rupture was made clinicoradiologically and surgery was planned. Intraoperative findings revealed a deficient triceps with a fleck of avulsed bone from olecranon. Ipsilateral double tendon graft including extensor carpi radialis longus and palmaris longus were anchored to triceps and secured with the olecranon. Six-months follow revealed a complete active extension of elbow and a full function at the donor site.
Keywords: Chronic triceps insufficiency, double tendon graft, triceps rupture
INTRODUCTION
The triceps tendon usually ruptures when there is fall on an outstretched hand with the elbow in incomplete extension with or without a concomitant blow to the posterior aspect of the elbow.1 Acute rupture of triceps following trauma usually occurs at the osteotendinous junction whereas a rupture at the myotendinous junction occurs less often.2 Predisposing factors include local steroid injection, olecranon bursitis, and hyperparathyroidism.3 Careful examinations of the active range of motion of the elbow determine the character of the tear, whether partial or complete.4
Initial diagnosis may be difficult because a palpable defect is not always present and pain may limit the motion. When the diagnosis is missed, it leads to prolonged disability to the extensor mechanism of the elbow. Making a clinicoradiological diagnosis using radiographs or ultrasound is important. MRI also plays a vital role in diagnosing this condition and determining its character.5
Here, we report a chronic triceps insufficiency managed with extensor carpi radialis longus and palmaris longus tendon grafts.
CASE REPORT
A 25-year-old male carpenter presented with a 1 year history of a significant fall sustaining multiple injuries. The major disabling injury following trauma was a fracture in both bones of left forearm which was treated with an open reduction and internal fixation. The patient also told a history of pain and swelling in the posterior aspect of the right elbow following the initial trauma. He was diagnosed as only soft tissue injury of right elbow. Soon after the swelling subsided, he noticed a depression in the posterior aspect of the elbow just above the olecranon for which he never sought any intervention. When he returned to his work as a carpenter after healing of other fractures, he felt disability limiting his activity which included inability to hammer and lack of extension. Clinical examination revealed a depression just above the olecranon at the osteotendinous junction of triceps. The limb was always kept in extension. He was able to do everything related with flexion, pronation, and supination, but was depending only on gravity for extention. There was obvious wasting of arm and forearm when compared with the other limb. There was no instability detected in the elbow. Radiographs revealed avulsion of a fleck of bone from the olecranon which migrated proximally attributing to the chronicity of the conditions [Figure 1]. The other limb regained full function with no abnormality.
Figure 1.
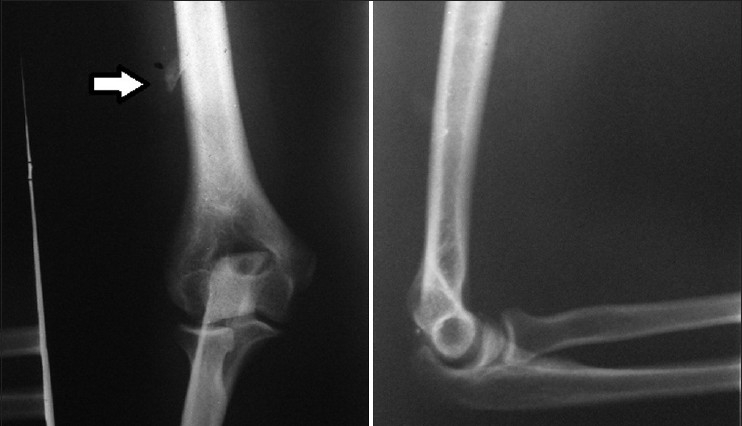
Plain X-ray of the elbow (anteroposterior and lateral view) showing avulsion of a fleck of bone from olecranon (write arrow)
Surgery was planned to fill the defect in the triceps and to reinforce it to the olecranon. The exposure of the tendon by midline posterior exposure showed a gap of 7 cms [Figure 2a]. Extensor carpi radialis longus tendon was released from its insertion by a small horizontal incision over the second metacarpal base. The tendon was pulled out through another proximal incision. The palmaris longus tendon was released at the level of flexor crease of the wrist and also pulled out through a proximal incision.
Figure 2.

(a) Intraoperative picture showing the insufficient triceps. (b) Anchoring the graft to the olecranon. (c) Postpulvertaft weaving of the graft to the triceps
After harvest, a double-stranded graft measuring 15 cm in length and 6 mm in width was made and sutured together. A medial to lateral horizontal tunnel was drilled measuring 6.5 mm in the olecranon. The double-stranded graft was passed through the tunnel with equal length on both sides. The grafts on either side were brought together proximally making four strands which were sutured as a single unit [Figure 2b]. The proximally retracted triceps was anchored to the quadruple strand of the graft by the pulvertaft weave technique [Figure 2c]. A full range of motion of the elbow was checked, and an above elbow plaster slab was given with the elbow in 15° of flexion.
The postoperative period was uneventful, and sutures were removed on the twelfth day. The above elbow plaster slab was maintained for 6 weeks to allow adequate tendon to bone healing. Elbow mobilization was initiated after 6 weeks. By 10 weeks, the patient regained full range of motion of the elbow [Figure 3]. On assessment of function using mayo elbow performance score, the maximum score of 100 was obtained which attributes to the full functional status of the patient.6
Figure 3.

Clinical photograph showing postoperative range of motion
The study has been reviewed by the appropriate ethics committee and has therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1964 declaration of Helsinki.
DISCUSSION
Chronic triceps insufficiency, causes prolonged disability. The tear usually occurs when there is eccentric load to a contracting triceps, most commonly during sports.7,8 The best management is to avoid misdiagnosis and to treat the condition at the earliest.9 Acute ruptures are successfully managed with nonabsorbable sutures passed through drill holes in the olecranon and anchored to the triceps.10 A chronic rupture is difficult to be reattached because of the retracted muscle belly.9 The literature provides various methods for correction oflarge triceps insufficiencies. It includes a turn down flap of triceps, anconeus rotation flap, allograft of tendo Achillis, and autograft of hamstring tendon.11,12
The use of extensor carpi radialis longus and palmaris longus to compensate a insufficient triceps has never been reported previously. Extensor carpi radialis longus muscle has been used in various types of procedures for corrective hand surgery and is a proper muscle for correction of finger clawing.13 Similarly, palmaris longus tendon is also being used for various procedures without significant functional impairment of the donor site.14 The easy availability of these tendons under regional anesthesia from the same limb without causing any significant functional impairment of the donor site led to their choice for our procedure.
Tendon to bone healing is said to be more secure, successful and functionally adaptive and hence preferred in this case.15–17 The diameter of the tendon was fit to the size of the tunnel to prevent any wear and tear of the tendon. Until adequate tendon to bone healing was achieved, the limb was immobilised. The patient achieved complete range of motion after 10 weeks with adequate physiotherapy. At the end of rehabilitation, the patient had almost full strength of extension. Functionally, as graded by the mayo elbow scoring system, the patient had maximum points and a full function of the affected elbow.6
ACKNOWLEDGMENTS
We are very thankful to our Professor and Head of the department Dr Senthilnathan, for his sincere guidance.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Bradford S. Bennett. Triceps tendon rupture: Case report and a method of repair. J Bone Joint Surg Am. 1962;44:741–44. [Google Scholar]
- 2.Aso K, Torisu T. Muscle belly tear of the triceps. Am J Sports Med. 1984;12:485–7. doi: 10.1177/036354658401200614. [DOI] [PubMed] [Google Scholar]
- 3.Yeh PC, Dodds SD, Smart LR, Mazzocca AD, Sethi PM. Distal triceps rupture. J Am Acad Orthop Surg. 2010;18:31–40. doi: 10.5435/00124635-201001000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Farrar EL, Lippert FG. Avulsion of the triceps tendon. Clin Orthop Relat Res. 1981;161:242–6. [PubMed] [Google Scholar]
- 5.Tiger E, Mayer DP, Glazer R. Complete avulsion of the triceps tendon: MRI diagnosis. Comput Med Imaging Graph. 1993;17:51–4. doi: 10.1016/0895-6111(93)90074-w. [DOI] [PubMed] [Google Scholar]
- 6.Morrey BF, An KN, Chao EYS. Functional evaluation of the elbow joint. In The Elbow and Its Disorders. 2nd ed. Philadelphia: W. B. Saunders; 1993. pp. 16–52. [Google Scholar]
- 7.Mair SD, Isbell WM, Gill TJ, Schlegel TF, Hawkins RJ. Triceps tendon ruptures in professional football players. Am J Sports Med. 2004;32:431–4. doi: 10.1177/0095399703258707. [DOI] [PubMed] [Google Scholar]
- 8.Singh RK, Pooley J. Complete rupture of the triceps brachii muscle. Br J Sports Med. 2002;36:467–9. doi: 10.1136/bjsm.36.6.467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Inhofe PD, Moneim MS. Late presentation of triceps rupture.A case report and review of the literature. Am J Orthop (Belle Mead NJ) 1996;25:790–2. [PubMed] [Google Scholar]
- 10.Sierra RJ, Weiss NG, Shrader MW, Steinmann SP. Acute Triceps Ruptures: Case report and retrospective chart review. J Shoulder Elbow Surg. 2006;15:130–4. doi: 10.1016/j.jse.2005.01.004. [DOI] [PubMed] [Google Scholar]
- 11.Clayton ML, Thirupathi RG. Rupture of the triceps tendon with olecranon bursitis. A case report with a new method of repair. Clin Orthop Relat Res. 1984;184:183–5. [PubMed] [Google Scholar]
- 12.Sierra RJ, Steinmann SP. Repair and reconstruction of traumatic deficiency of the triceps. Curr Orthop Pract. 2008;19:280–7. [Google Scholar]
- 13.Malaviya GN. ECRL- A wrist extensor with multiple uses in deformity correction. Indian J Lepr. 2008;80:1–6. [PubMed] [Google Scholar]
- 14.Isenberg JS, Fusi S. Immediate tendon Achilles reconstruction with composite palmaris longus grafts. Ann Plast Surg. 1995;34:209–11. doi: 10.1097/00000637-199502000-00018. [DOI] [PubMed] [Google Scholar]
- 15.Newsham-West R, Nicholson H, Walton M, Milburn P. Long-term morphology of a healing bone-tendon interface: A histological observation in the sheep model. J Anat. 2007;210:318–27. doi: 10.1111/j.1469-7580.2007.00699.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.St Pierre P, Olson EJ, Elliott JJ, O’Hair KC, McKinney LA, Ryan J. Tendon healing to cortical bone compared with healing to a cancellous trough.A biomechanical and histological evaluation in goats. J Bone Joint Surg Am. 1995;77:1858–66. doi: 10.2106/00004623-199512000-00010. [DOI] [PubMed] [Google Scholar]
- 17.Ekdahl M, Wang JH, Ronga M, Fu FH. Graft healing in anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2008;16:935–47. doi: 10.1007/s00167-008-0584-0. [DOI] [PubMed] [Google Scholar]