

Abstract
Background:
CD4 lymphocyte cells are often used as prognostic markers for monitoring the progression of immunosupression such as HIV infection.
Aim:
This study was conducted to assess the distribution of CD4 lymphocytes among apparently healthy human immunodeficiency virus (HIV) seronegative and seropositive populations in a Nigerian state.
Materials and Methods:
A total of 1520 apparently healthy subjects aged 18–64 years, composed of 800 males and 720 females attending some selected health institutions in the state, participated in the study. Ten milliliters of blood was collected from each subject; 5 ml of this was used for HIV antibodies sero-typing while the remaining 5 ml was anticoagulated and used for CD4 lymphocytes level determination. Only samples tested positive both with Capillus and Determine HIV test kits were further differentiated into sero-types with a standard diagnostic HIV test kit. The CD4 lymphocyte levels of all the sample were determined; mean CD4 levels of 205.1±0.09 and 287.4±0.3 cells/μl were recorded among females seropositives and seronagatives respectively. Statistical analysis by the Student t-test showed a significant difference in the mean CD4 lymphocyte count by gender.
Results:
Findings showed a mean CD4 level of 311.7±1.2 cells/μl among seropositive males while 399.3±0.6 cells/μl was recorded among seronegatives (t=5.86). The study also recorded a CD4 lymphocyte range of 232–464 cells/μl among apparently healthy seronegative population in this locality.
Conclusion:
The findings showed a significantly higher mean CD4 lymphocyte count among adult male HIV seronegatives (χ2=9.22) and seropositives (χ2=15.07) than their female counterparts. Further research work using the automation technique is suggested to confirm this new range for monitoring HIV subjects on antiretroviral therapy.
Keywords: CD4-lymphocytes, Human immunodeficiency virus, Seronegative, Seropositive
Introduction
Human immunodeficiency virus (HIV) was first reported in 1981 in the United States of America among the homosexuals,[1–5] but not until 1986 the first episode was documented in Nigeria among prostitutes[3] As in the year 2008, the global estimate of people living with HIV/AIDS was 33.4 million with Africa constituting about 60% of this figure. Over 2.7 million people were newly infected in the year.[6,7] Currently Nigeria ranked third with 7.5 million people living with the dreaded virus next to India and South Africa[7] The frequency of HIV/AIDS by gender in Port Harcourt, Nigeria, is at the ratio of 1:1 male to female[8] while death resulting from the infection alone makes it one of the 10 leading causes of death in children and women of 15–44 years of age world-wide.[9,10]
Morbidity and mortality rates due to HIV/AIDS are probably the highest in the world. Africa and indeed Nigeria are no exceptions. Richard reported that over 25 million deaths due to HIV/AIDS had already been recorded globally while not less than 10,000 youths are infected monthly in Nigeria.[11] In separate studies, Abdulazeez et al.[3] and FMOH/WHO[12] reported that over 1.2 million people have already developed clinical manifestations of acquired immunodeficiency syndrome (AIDS)] in Nigeria as at 2005. People living with HIV may not develop any symptoms for over 10 years but can still transmit the infection to others during the asymptomatic period. Most people infected with HIV are likely to develop AIDS if not treated or slowly develop AIDS due to their genetic difference that prevents the virus from damaging their immune system.
Terhost et al.[13] defined CD4 lymphocytes as a subset of thymocyte-derived lymphocytes which are continuously expressed in the peripheral blood and lymphoid tissue. The definition of an AIDS patient nowadays is a person who is HIV seropositive and has CD4 less than 200 cells/ μl even if the person appears apparently healthy.[14]
CD4 lymphocyte cells are a type of immune cells otherwise known as T-helper cells which are often used as prognostic markers for monitoring the progression of immunosupression such as HIV infection. A study carried out in Tanzania reported that gender and geographical differences are some of the factors affecting the values of the CD4 level among immunosuppressed subjects.[15]
In a situation where permanent cure of the virus remains a mirage, prevention from the infection and proper management of those already living with the virus are ways to keep people alive. Use of antiretroviral drugs plays a vital role in this regard. Apart from physical examination of those on antiretroviral therapy, determination of the CD4 lymphocyte level of the patients is an important way of monitoring their responses to treatment. Ordinarily every human being has the tendency to recover from any disease condition even without any treatment due to the ability of the body immune system to recognize and destroy foreign body as quickly as possible. CD4 lymphocyte cells are the key elements in body immune systems responsible for such body defense. Ironically, with HIV infection, these cells are attacked and destroyed by the virus, thereby destroying the defense machinery of the body hence, making it more vulnerable to any disease condition without any resistance. The higher the viral load the greater the havoc on the CD4 lymphocytes and the lower the immunity of the host. This is why CD4 lymphocytes level determination is very crucial, as a barometer for measuring the immunity of HIV-infected people, especially those on therapy. In a study conducted by Clark and Shaw, it was reported that AIDS symptoms usually start to manifest when the CD4 lymphocyte level is below 300 cells/μl, while in another study, it was reported that the destruction rate of CD4 lymphocyte cells in infected persons was 12 cells /μl per fortnight. Also, in untreated cases, the average survival time after the manifestation of clinical signs and symptoms of AIDS is about 1.5 years.[15]
This study therefore attempted to determine a CD4 lymphocyte reference range in this part of the globe so that it can serve as a guide for effective management of HIV-infected people on highly active antiretroviral therapy (HAART).
Materials and Methods
Study population
A total of 1520 subjects aged 18–64 years, composed of 800 males and 720 females attending Federal Medical Center, Specialist Hospital, General Hospitals in Ganye, Mubi, Garkida and Numan were randomly selected for the study. Other participants were subjects attending Kowa Hospital, Peace Hospital, Adamawa Hospital, Yola Biomedics Laboratories and Health Centers in Tola, Pella, and Fufore all in Adamawa state of Nigeria. The subjects were apparently healthy individuals seeking medical check-up for military recruitment, marriage, blood donation, and those seeking admission into secondary and tertiary institutions in the state. They also included some apparently healthy volunteers among the staff of the health institutions and some subjects attending HIV voluntary counseling and testing clinics. Prior to the commencement of sample collection, approval from Research and Ethics committee of the State Ministry of Health was obtained in accordance with the Helsinki Declaration guidelines. Also, consent of the participants was sought and obtained as only volunteers were enrolled in the study.
Collection and laboratory analysis of specimens
Ten milliliters of blood was collected from each of the subjects by vein puncture. Five milliliters was put in plain test tubes held at room temperature for 20 minutes and then spun to remove the serum needed for HIV antibody typing. The remaining 5 ml was put in containers with ethylene diamine tetra acetic acid (EDTA), mixed properly and used for the CD4 lymphocyte count.
A Capilus HIV screening kit (Trinity Biotech, United Kingdom) was used for the antibody detection while a Standard Diagnostic (Bioline, Korea) kit was employed for classifying all seropositive cases into HIV-1, HIV-2, and HIV-1+2. Commercial Dynal beads (Dynal Asa Oslo Norway) were employed to quantify the CD4 level in seropositive and seronegative samples following the manufacturer's instructions.
HIV screening technique
A Capillus HIV screening device composed of slide and latex reagent was employed. One drop of latex reagent and a drop of each test serum were mixed in the well of the slide. The mixture was allowed to flow by capillary action through the slide channel. Appearance of visible agglutination on the slide channel was recorded as “reactive” while milky white appearance without agglutination was considered “nonreactive.”
A system diagnostics reagent cassette was used to test the serotype of all HIV-reactive sera. A drop of the serum was put in the test window of the reagent cassette and allowed for 5 minutes for the serum to flow through control and test column of the cassette. Appearance of two pinkish lines in the cassette within 5 minutes showed the presence of HIV serotype with the control. Whenever the line appeared before the line of control band, it was an indication of the presence of HIV-1 and when the line appeared after the control band, it was an indication of the presence of HIV-2 in the serum. When there was appearance of three pinkish lines, it was an indication of the presence of both HIV-1 and HIV-2 serotypes. The Dynal bead method was employed to determine the CD4 count as earlier described by Idoko et al.[16]
Statistical analysis
Data obtained from the tests were entered and analyzed using SPSS Version 16 software of computer (SPSS Inc., USA). The test of significance was performed using the chi-square test for CD4 distribution with respect to HIV serotypes and Student t-test for CD4 distribution by gender and by HIV serostatus. Each CD4 mean deviation was computed using the standard deviation formula. The level of significance for statistical difference was based on P<0.05.
Results
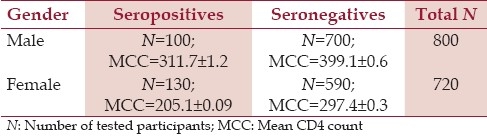
Table 1 depicts the distribution of mean CD4 lymphocytes by gender among the cohort seropositive and seronegative subjects. The mean CD4 lymphocyte count was lower in females compared to males across serostatus and also in seropositive compared to seronegative within gender. Statistical analysis by the Student t-test showed a significant difference in the mean CD4 lymphocyte distribution by sex (t=5.86).
Table 1.
Distribution of mean CD4 lymphocytes by gender
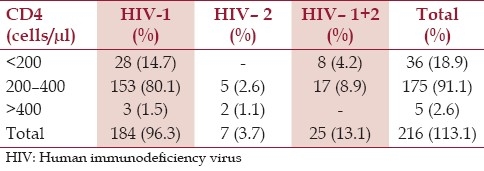
The distribution of the mean CD4 lymphocyte level in HIV seropositive and seronegative populations is as shown in Table 2 while the frequency of 191 seropositive cases by HIV types and CD4 lymphocyte levels is as shown in Table 3. Most of the seropositive 184 (96.3%) had type 1 HIV while most 175 (91.1%) had CD4 lymphocyte count within 200–400 range. The result also showed a significantly higher mean CD4 lymphocyte count among adult male HIV seronegatives (χ2=9.22) and seropositives (χ2= 15.07) than their female counterparts.
Table 2.
Mean CD4 lymphocyte cell concentration in HIV seropositive and seronegative populations
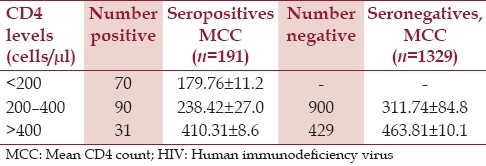
Table 3.
CD4 lymphocyte cell distribution by HIV serotypes (n=191)
Discussion
Findings in this study showed a significantly higher mean CD4 lymphocyte count among adult male HIV seronegatives (χ2=9.22 ) and seropositives (χ2= 15.07) than their female counterparts. This result is in contrast with the findings of Urassa and his associates[17] conducted among adult Tanzanians in which the mean CD4 lymphocytes level was higher among adult females than their male counterparts. The reason for the difference between the present study and the previous one could probably be due to geographical variation. Another reason could be attributed to difference in the method of assay. While the Dynal bead manual technique was employed in this study, automation was used in the previous one.
The present result also showed that 47.0% of HIV seropositive subjects had mean CD4 count between 200 cells/μl and 400 cells/μl, 36.8% had CD4 lymphocytes less than 200 cells/μl while 16.2% of the subjects had CD4 lymphocytes higher than 400 cells/μl with all the subjects still appearing apparently healthy. These findings disagree with the results of Reeves[18] Erhabor et al.,[19] which reported that with CD4 lymphocytes less than 300 cells/μl AIDS symptoms are likely to start manifesting. The reason for the difference between this observation and the previous one could probably be due to variation in the geographical location and immune status of the subjects. Meanwhile, this finding is in consonance with the result of Idoko and his associates[16] reporting similar views that subjects with CD4 lymphocytes lower than 300 cells/μl could still be apparently healthy.
CD4 lymphocyte count is a prognostic marker for monitoring the response of HIV-infected patients to antiretroviral therapy. In this study, a CD4 lymphocyte range of 232–464 cells/μl among apparently healthy seronegative subjects was recorded. Going by Clark and Shaw[20] results and findings of MacDonnell and his co-workers,[21] part of the values recorded within normal values in this study would have been considered abnormally low with such subjects probably incorrectly labeled AIDS patients. However, with this newly documented lymphocyte range, symptoms of AIDS may only start to manifest when the CD4 lymphocyte count is below 232 cells/μl.
Urassa and co-workers[16] had earlier reported that the CD4 lymphocyte level varies with geographical setting, race, and gender among immunosuppressed subjects. This range differs considerably from the reagent kit manufacturer's recommended range which was put at 250–500 cells/μl. The scenario is not surprising because the manufacturer's values were probably obtained from entirely different geographical setting and race since the test kit was imported from Norway.
Conclusion
The findings showed a significantly higher mean CD4 lymphocyte count among adult male HIV seronegatives (χ2=9.22) and seropositives (χ2= 15.07) than their female counterparts. Also, the CD4 range of 232–464 cells/μl was recorded among apparently healthy seronegative subjects. Further research work using the automation technique was suggested to confirm this new range before it could be recommended as a useful reference for monitoring HIV subjects on antiretroviral therapy.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Sharp DA. Controversial HIV/AIDS hypothesis. Lancet. 1999;35:1129–30. [Google Scholar]
- 2.Sepkowitz K. AIDS: The first twenty years. N Engl J Med. 2001;344:1764–72. doi: 10.1056/NEJM200106073442306. [DOI] [PubMed] [Google Scholar]
- 3.Abdulazeez AA, Alo EB, Nassar AS. Harwnization of HIV testing in Nigeria: A missing step in HIV/AIDS control. Niger J Biomed Sci. 2006;2:23–6. [Google Scholar]
- 4.Funnyé AS, Akhtar AJ. Syphilis and human immunodeficiency virus co-infection. J Natl Med Assoc. 2003;95:363–82. [PMC free article] [PubMed] [Google Scholar]
- 5.Selik A. AIDS trends in United States from 1978 to 1982. Am J Med. 1984;76:493–500. doi: 10.1016/0002-9343(84)90669-7. [DOI] [PubMed] [Google Scholar]
- 6.FMOH Republic of Nigeria National HIV Seroprevalence sentinel survey. FMOH Expert committee Report series. 2008 [Google Scholar]
- 7.UNAIDS/WHO. AIDS Epidemic Update: 2008 report on Global AIDS epidemics. [Last Accessed on 2011 Apr 10]. Available from: http://www.int/hiv/epi/updates/en/indes/htm .
- 8.Archibong AE, Ikpi A. Human Immunodeficiency virus (HIV) prevalence and paediatric surgical practice in the Developing countries. J Med Lab Sci. 2002;11:34–8. [Google Scholar]
- 9.Leofler JP. Nigeria: The Medicine Group. Ltd; 1992. Surgeons and AIDS in African surgery; pp. 95–6. [Google Scholar]
- 10.Gerbending JL. Protecting health care workers from HIV infection. Contemp Intern Med. 1991;2:45–54. [Google Scholar]
- 11.Richard CO. 1st ed. Harcourt, Nigeria: Fine Job Publications Port; 2006. The untold origin and lies about HIV/AIDS; pp. 40–7. [Google Scholar]
- 12.FMOH. Republic of Nigeria/WHO National guidelines for HIV/AIDS voluntary counselling and testing (VCT) services in Nigeria. 2003:1–91. [Google Scholar]
- 13.Terhorst CV, Agthreen A, Reinherz LL. Biochemical analysis of Human T-Lymphocyte differentiation antigen T4 and T8. Science. 1980;209:520–52. doi: 10.1126/science.6967228. [DOI] [PubMed] [Google Scholar]
- 14.Goldman L, Ausiello D. 23rd ed. Philadelphia, Pa: Saunders Elsevier; 2009. Cacil Medicine; pp. 26–7. [Google Scholar]
- 15.Wang C, Vlahov D, Galai N, Bareta J, Strathdee SA, Nelson KE, et al. Motality in HIV seropositive virus and senoregative persons in the era of HAART: Implications for when to initiate therepy. J Infect Dis. 2004;190:1046–54. doi: 10.1086/422848. [DOI] [PubMed] [Google Scholar]
- 16.Idoko JA, Isamade EI, Sirisena ND. CD4 7-Lymphocyte count in HIV infected and healthy Nigeria population. Niger Med Pract. 2001;3:53–56. [Google Scholar]
- 17.Urassa WK, Mbana EM, Swai AB, Gain H, Nhalu FS, Biber Feld G. Lyrnphocytes sub-set enumeration in HIV seronegative and HIV seropositive adults in Dar es salem. Tanzania. Determination of reference values in males and females and comparison of two flow cytometric methods. J Immunol Methods. 2009;277:65–74. doi: 10.1016/s0022-1759(03)00174-1. [DOI] [PubMed] [Google Scholar]
- 18.Reeves GK. The overall distribution of survival time for AIDS patients in United Kingdom. Philos Trans R Soc Lond B Biol Sci. 1989;325:147–51. doi: 10.1098/rstb.1989.0079. [DOI] [PubMed] [Google Scholar]
- 19.Erhabor OA, Ejele CA, Nwauche FT, Busaari O. CD4 T- helper Lymphocyte counts decline at a mean rate of 12 calls per 8 weeks in untreated HIV–infected Africans. Nigerian Perspective Nigerian Biomed Sci Jour. 2002;1:38–41. [Google Scholar]
- 20.Clark SJ, Show GM. The acute retroviral syndrome and pathogenesis of HIV infections. Semin Immunol. 1993;5:149–50. doi: 10.1006/smim.1993.1018. [DOI] [PubMed] [Google Scholar]
- 21.Mc Donell KB, Chamiel JS, Poggensee P. Predicting progression to AIDS: Combined usefulness of CD4 Lymphocytes count and 24P antigenemia. Am J Med. 1990;89:706–12. doi: 10.1016/0002-9343(90)90210-5. [DOI] [PubMed] [Google Scholar]